

Abstract
Rectus femoris origin injuries in adult athletes are uncommon. In the acute phase, conservative treatment seems to have a favourable outcome, with surgical repair reserved for unsuccessful cases only. However, a group of patients may develop chronic pain and disability after recovery from the acute phase due to heterotopic calcification occurring at the site of injury. Open and arthroscopic excision of such calcifications has been described in the literature although arthroscopic excision of large calcified lesions in the rectus femoris has not been reported previously. A relevant case is presented and discussed.
Keywords: Calcific lesion, Hip arthroscopy, Rectus femoris origin injury, Tendon avulsion
The rectus femoris is the most commonly injured muscle of the quadriceps muscle group as it crosses both the hip and knee joints. The most common injury to the rectus femoris is an intramuscular strain to the musculotendinous junction.1 Rectus femoris origin (RFO) injuries, including an avulsion of the direct or indirect heads with or without a bony fragment and partial or complete tears of the tendons proximal to the musculotendinous junction, have been reported in the paediatric and adolescent populations but not as much in adult athletes.2 Ouellette et al reviewed 3,160 pelvis and hip magnetic resonance imaging (MRI) scans retrospectively and found that the incidence of RFO injuries was 0.5 %.1
Patients usually present with acute onset of groin pain after an injury to the hip. Diagnosis includes plain x-rays that may demonstrate an avulsion fracture. Computed tomography and MRI often show signal changes in the injured tendon(s) consistent with partial or complete tears, retraction and buckling of the tendon(s) in complete tears, avulsion fractures and calcification in chronic cases, and they can rule out other hip pathology.1–3
In the acute phase following trauma, treatment can either be conservative or surgical repair. Conservative treatment includes rest, elevation and anti-inflammatories while maintaining the leg in extension and allowing quadriceps isometric exercises. No return to training should be allowed until full stretch of the muscle has been achieved. Surgical repair has also been described as a primary treatment or when conservative management fails in such injuries.4
Rarely, some patients may develop calcification after resolution of the acute phase of the injury. In these cases, the necrotic tissue resulting from the tear is replaced by fi-brinoid mass, leucocytes and histiocytes. Fibroblasts deposit calcium microcrystals in the tendon, causing calcification. Open excision of calcified lesions through an anterior approach has been described.5 However, arthroscopic excision of a large lesion in the rectus femoris has not been reported. We present the case of a 24-year-old man who presented with a large calcification in the rectus femoris that was treated successfully by hip arthroscopy.
Case history
A 24-year-old British man of Asian origin, who is a keen sportsman, presented with 8 months’ history of right-sided hip pain, which started after an acute incident involving a great deal of kicking against a punch bag. He had no previous problems of either hips and both his past medical and family histories were insignificant. He was seen two weeks following the injury by his general practitioner, who treated him with a short period of bed rest followed by progressive weight bearing using crutches over eight weeks. This improved his symptoms initially.
Nevertheless, after commencing physiotherapy exercises in the form of quadriceps stretching, the patient felt gradual deterioration with increased pain and restricted movements of the hip, preventing him from performing sports. On examination, there was no major muscle wasting of the right leg, a significant limp or a palpable mass. Straight leg raise was 90° and abduction 50° bilaterally. However, flexion of the right hip was limited to 95° due to discomfort compared with 120° on the left side. Internal rotation with hip flexion was also limited to 10° compared with 25° on the left.
X-rays showed a calcified lesion in the RFO (Figs 1,2). Subsequent MRI revealed a comet-shaped focus of low signal measuring 28mm, consistent with calcification in the reflected head of the RFO, associated with a tear of the tendon. There was also degenerative labral damage in the hip (Fig 3). As a result, an arthroscopy was performed to address both the intra and extra-articular pathologies. A lateral portal was used for the arthroscope with an anterola-teral portal for instrumentation. The large bony lesion was removed using a burr and the labral tear debrided (Figs 4,5). Post-operatively, the patient was able to flex to 110° without pain or restriction and allowed to fully weight bear. Two weeks later, he was started on stretching exercises and at six weeks graduated strengthening exercises of the quadriceps. He was able to return to full training within eight weeks.
Figure 1.

Anteroposterior x-ray of both hips with arrow pointing to calcified lesion in the rectus femoris origin
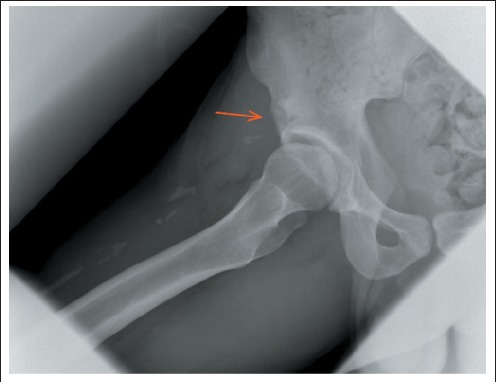
Figure 2.

Lateral x-ray of right hip with arrow pointing to calcified lesion in the rectus femoris origin
Figure 3.
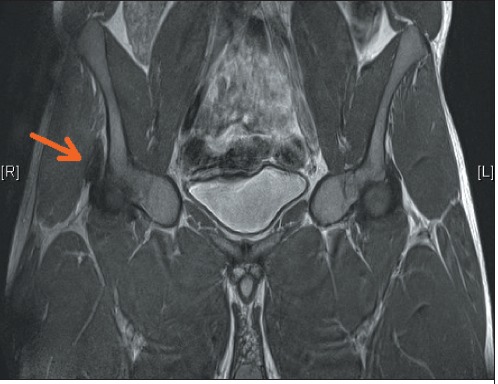
Magnetic resonance imaging demonstrating a tear and comet-shaped low signal focus of calcification in rectus femoris
Figure 4.

Post-operative anteroposterior x-ray of both hips with arrow pointing to excised lesion
Figure 5.
Post-operative lateral x-ray of right hip with arrow pointing to excised lesion
Discussion
A better understanding of RFO injuries followed the increased use of MRI, which allowed more detailed descriptions. The mechanism of injury typically relates to a strong contraction of the rectus femoris, which is common while kicking against a forcible block.2 The resultant site of injury is dependant on the age group. In children and adolescents an avulsion fracture tends to occur at the apophysis and in young adults the tendon tears at the musculotendinous junction whereas in elderly patients fibres fail at the weakened sites of degeneration.2
Treatment of RFO injuries remains controversial. Gamradt et al reported a series of 11 professional American football players with avulsion injuries to the RFO who were managed conservatively with return to full sporting activities within 6-12 weeks.2 On the other hand, Irmola et al treated five athletes with proximal avulsion of the direct head of the rectus femoris by surgical repair using two bone anchors placed into the anterior inferior iliac spine.4 Full recovery occurred in 5-10 months.
Heterotopic calcification in the rectus femoris tendon is a sign of chronicity of the injury and differential diagnoses should include avulsion fractures, calcific tendinitis, os acetabuli, sesamoid bones in the tendon and myositis os-sificans as well as tumours such as juxtacortical chondro-ma, chondrosarcoma and synovial sarcoma.3 A careful assessment of the patient's presentation and investigations is therefore required to reach the correct diagnosis. This case illustrates that arthroscopic surgery is a feasible option in such cases and allows a rapid recovery.
Conclusions
In our case report, hip arthroscopy was performed to address both intra and extra-articular problems simultaneously. This may offer an alternative to open surgical excision of large calcified lesions of the rectus femoris, especially with concomitant intra-articular pathology, and allows for a shorter hospital stay, and much earlier mobilisation and rehabilitation.
References
- 1.Ouellette H, Thomas BJ, Nelson E, Torriani M. MR imaging of rectus femoris origin injuries. Skeletal Radiol. 2006;35:665–672. doi: 10.1007/s00256-006-0162-9. [DOI] [PubMed] [Google Scholar]
- 2.Gamradt SC, Brophy RH, Barnes R, et al. Nonoperative treatment for proximal avulsion of the rectus femoris in professional American football. Am J Sports Med. 2009;37:1,370–1,374. doi: 10.1177/0363546509333477. [DOI] [PubMed] [Google Scholar]
- 3.Sarkar JS, Haddad FS, Crean SV, Brooks P. Acute calcific tendinitis of the rectus femoris. J Bone Joint Surg Br. 1996;78:814–816. [PubMed] [Google Scholar]
- 4.Irmola T, Heikkila JT, Orava S, Sarimo J. Total proximal tendon avulsion of the rectus femoris muscle. Scand J Med Sci Sports. 2007;17:378–382. doi: 10.1111/j.1600-0838.2006.00564.x. [DOI] [PubMed] [Google Scholar]
- 5.Braun-Moscovici Y, Schapira D, Nahir AM. Calcific tendinitis of the rectus femoris. J Clin Rheumatol. 2006;12:298–300. doi: 10.1097/01.rhu.0000249896.43792.62. [DOI] [PubMed] [Google Scholar]