

Abstract
Previous caries experience correlates to future caries risk; thus, early identification of lesions has importance for risk assessment and management. In this study, we aimed to determine if Quantitative Light-induced Fluorescence (QLF) parameters—area (A [mm2]), fluorescence loss (∆F [%]), and ∆Q [%×mm2]—obtained by image analyses can predict lesion progression. We secured consent from 565 children (from 5-13 years old) and their parents/guardians and examined them at baseline and regular intervals over 48 months according to the International Caries Detection Assessment System (ICDAS), yearly radiographs, and QLF. QLF images from surfaces with ICDAS 0/1/2/3/4 at baseline that progressed (N = 2,191) to cavitation (ICDAS 5/6) or fillings and surfaces that did not progress to cavitation/fillings (N = 4,141) were analyzed independently for A, ∆F, and ∆Q. Linear mixed-effects models were used to compare means and slopes (changes over time) between surfaces that progressed and those that did not. QLF A, ∆F, and ∆Q increased at a faster rate for surfaces that progressed than for surfaces that did not progress (p = .0001), regardless of type of surface or baseline ICDAS score. AUC for ICDAS ranged from 0.65 to 0.80, but adding QLF information improved AUC (0.82-0.87, p < .0005). We concluded that faster changes in QLF variables can indicate lesion progression toward cavitation and be more clinically relevant than actual QLF values.
Keywords: dental caries, prospective study, visual examination, early diagnosis, fluorescence imaging
Introduction
Previous caries experience has been the only risk factor that consistently correlates to future caries risk (Bader et al., 2008). Therefore, the detection of caries lesions at their earliest stage can significantly assist in determining future risk (Zero et al., 2011). However, it is known that not all lesions progress to cavitation (Backer Dirks, 1966; Ferreira Zandoná et al., 2012); thus, identifying which of these early lesions are likely to progress will allow dentists to provide focused early preventive intervention (Zero et al., 2011; Ferreira Zandoná et al., 2012).
There has been considerable interest in developing methodologies that can help dentists to detect caries at early stages. The International Caries Detection and Assessment System (ICDAS), a visual method that assesses the severity of dental caries using 7 scores (0-6), has been shown to be a reliable method to assess early lesions (Ekstrand et al., 2007; Ismail et al., 2008; Varma et al., 2008). Additionally, we have reported that these early lesions (ICDAS 1 or 2) can be monitored by visual examination. When it is observed that they transition to a moderate lesion (ICDAS 3 or 4), the lesions can be used as surrogates of cavitation in a high-risk population (Ferreira Zandoná et al., 2012). Quantitative Light-induced Fluorescence (QLF) is a technology-based method that has been stated to have high sensitivity for the detection of early lesions (Diniz et al., 2012; Jablonski-Momeni et al., 2012; Souza et al., 2012). Because this method is quantitative (Ando et al., 2001; Karlsson et al., 2007; Kühnisch et al., 2007), it allows for longitudinal monitoring of lesion progression (Ferreira Zandoná et al., 2000; Tranaeus et al., 2001; Kambara et al., 2003). The combined use of ICDAS with QLF (Ferreira Zandoná et al., 2010) allows for the earlier detection of caries lesions, avoiding the pitfalls that have been associated with QLF: the confounding effects of developmental defects, fluorosis (Pretty et al., 2006), stain (Shi et al., 2001), swollen gingival margin, presence of plaque, and quality of fluorescence images (Heinrich-Weltzien et al., 2005).
The objective of this four-year longitudinal study was to determine if QLF parameters (∆F - %; ∆area - mm2; and ∆Q - mm2 x %) obtained by the analyses of fluorescent images could be used to predict lesion progression toward cavitation.
Study Population & Methods
As previously reported (Ferreira Zandoná et al., 2010, 2012; Fontana et al., 2011), children (N = 565) from public schools (kindergarten to 9th grade) in Aguas Buenas, Puerto Rico were recruited as approved by the institutional review board committees from Indiana University (IU-IRB #0608-15) and the University of Puerto Rico (UPR-IRB#A1340107). Parental consent was obtained along with assent from the child for children older than 7 yrs. The sample size was chosen based on preliminary data, to allow for a sufficient number of clinically significant lesions at the end of the study. Inclusion criteria were age (5-13 yrs), no medical problem contraindicating participation, and tolerance for oral examination, including radiographs, digital photographs, and QLF examinations. Both caries-free and caries-active children, with at least one permanent molar and at least one unrestored surface, were recruited.
Examinations—which consisted of an oral soft tissue examination, a visual examination according to the ICDAS criteria, which range from 0 to 6 (Ferreira Zandoná et al., 2010), and an examination with QLF, all completed by a single calibrated examiner—were conducted at baseline, 8, 12, 20, 24, 28, 32, 36, 40, 44, and 48 mos. The occlusal and buccal surfaces of all permanent molars and the lingual surfaces of upper molars were examined, and fluorescence images were acquired with Quantitative Light-induced Fluorescence (QLF Pro, Inspektor Research Systems B.V., Amsterdam, The Netherlands) in a controlled darkened environment, immediately after the ICDAS examination. Bitewing radiographs were obtained yearly, but the results are not included in these analyses. Details of the ICDAS examinations were published previously (Ferreira Zandoná et al., 2012). The study complied with the STROBE criteria.
Fluorescence Image Analyses
QLF images from surfaces with ICDAS scores 0/1/2/3/4 at baseline that progressed to cavitation (ICDAS scores 5/6) or fillings (N = 2,191) at any subsequent examination and a random sample of surfaces that did not progress to cavitation/filling (N = 4,141) at the end of the four-year study were analyzed independently for average area (∆A [mm2]), fluorescence loss (∆F [%]), and ∆Q [%×mm2], with dedicated software (QLF 2.00g, Inspektor Research Systems B.V., Amsterdam, The Netherlands) as previously described (Ando et al., 2001) (Fig. 1). A patch was placed on the last image of the lesion on the visit that preceded cavitation, and that patch was copied on all previous images including the baseline visit images.
Figure 1.

Examples of reflectance and fluorescent images of lesions that progressed to cavitation and did not progress to cavitation based on baseline ICDAS scores.
Statistical Analyses
The last visit with QLF image analyses was determined for each tooth surface. Visits were re-numbered as the number of 4-month periods prior to the last visit for the tooth surface. Summary statistics (mean, standard deviation, standard error, range) for QLF ∆A, ∆F, and ∆Q were calculated by visit and whether or not the surface progressed to cavitation or filling by the end of the study period. Linear mixed-effects models were used to compare the means and slopes (changes over time) between surfaces that progressed and those that did not progress. The models included random effects for each participant, participant-by-tooth, and participant-by-tooth-by-surface to model within-participant correlations between observations. Analyses were performed overall (adjusted for surface and baseline ICDAS as well as the demographic characteristics age, gender, race, and ethnicity), by surface (adjusted for baseline ICDAS and demographics), and by baseline ICDAS (adjusted for surface and demographics). These models indicate the average trajectories of the QLF parameters over time for lesions that ultimately progressed and those that did not. Additionally, slopes representing the changes in QLF measurements over time were calculated for each individual surface; one slope was estimated over all time-points for each surface for each participant. The surface type (buccal, lingual, occlusal), individual QLF slopes, baseline ICDAS score, last ICDAS (at final visit if no cavitation, at visit before cavitation if surface cavitated), last QLF values, and the interactions between baseline ICDAS and QLF slopes were included in a logistic regression model to calculate the area under the receiver operating characteristic (ROC) curve (AUC). To evaluate the associations between the ICDAS levels and QLF ∆F with data from all time-points, QLF ∆F values were compared among ICDAS levels in a linear mixed-effects model which included random effects for participant, participant-by-tooth, and participant-by-tooth-by-surface to model within-participant correlations between observations and included surface type and demographics as covariates.
Results
There were 338 children who completed the examinations at the 48-month visit. Details have previously been published (Ferreira Zandoná et al., 2012). The surfaces that cavitated and, thus, had the images analyzed from each of the examination periods are from 359 children at baseline, 317 at visit 1, 272 at visit 2, 281 at visit 3, 244 at visit 4, 220 at visit 5, 168 at visit 6, 136 at visit 7, 116 at visit 8, 71 at visit 9, 46 at visit 10, and 46 at visit 11. On average, there were images of 2.3 to 3.3 surfaces analyzed from each of the visits, ranging from 1 to 16 images per child. (Characteristics of the lesions are provided in Appendix Table 1.) Fillings were included as part of the study outcome definition. Progression was not considered after sealants were placed. Caregivers were asked to complete yearly questionnaires, which included an item about fluoride treatments received at the dentist’s office. Nearly 90% of the respondents indicated that the child received a fluoride treatment at least once per year.
All the QLF parameters (QLF A, ∆F, and ∆Q) increased at an overall faster rate (i.e., larger slope) on average for surfaces that progressed than for surfaces that did not progress (p = .0001) to cavitation, regardless of type of surface or baseline ICDAS score (Appendix Tables 2 and 3). Since the differences were significant for all parameters, only ∆F values are presented.
As can be seen in Fig, 2, independent of surface type (buccal, occlusal, or lingual), surfaces that progressed to cavitation had significantly more fluorescence loss (∆F) than surfaces that did not progress (p < .0001).The rate of progression (slope difference) of lesions that progressed to cavitation was significantly greater (progressed faster) than that of those that did not progress (p < .0001). QLF ∆F values tended to be higher at baseline for lesions that progressed to cavitation and had a progressive increase prior to cavitation. QLF ∆F values tended to be higher for lesions on occlusal surfaces compared with those on buccal or lingual surfaces.
Figure 2.
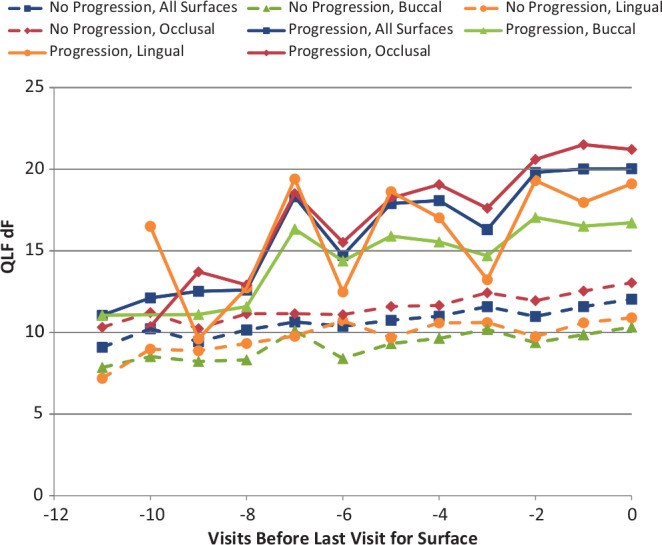
Fluorescence loss (∆F) from baseline to last visit before cavitation as determined by ICDAS based on progression status and surface.
The results based on the ICDAS scores at baseline can be seen in Fig. 3. Independent of the ICDAS score at baseline, lesions that progressed to cavitation had QLF ∆F values increasing at a faster rate than those of lesions that did not progress to cavitation. This was true for all surfaces and for all QLF parameters.
Figure 3.
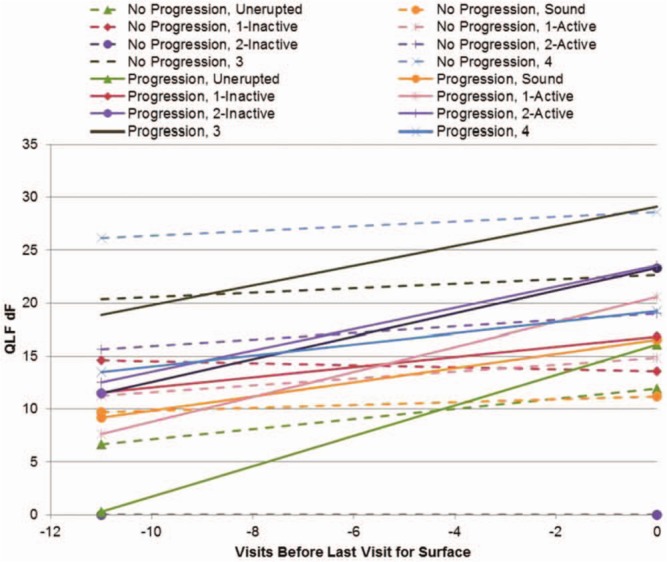
Regression slopes for QLF ∆F values by ICDAS scores at baseline for lesions that progressed to cavitation and lesions that did not progress to cavitation, based on the number of visits that preceded cavitation.
Because of the differences in progression rates observed between lesions that progressed to cavitation and those that did not, the slopes for the QLF parameters were calculated for each surface (individual slopes for every surface evaluated), and the individual slopes and last QLF measurement were used to predict cavitation. As indicated in Fig. 4, the AUC for ICDAS alone was low for buccal and lingual surfaces and still below 0.80 for occlusal surfaces. When the QLF information was also included in the model, significant improvements in AUC were observed for buccal and lingual surfaces. The increases in the AUC with the addition of the QLF parameters were statistically significant (p = .0005 for lingual surfaces, p ≤ .0001 for all other comparisons).
Figure 4.
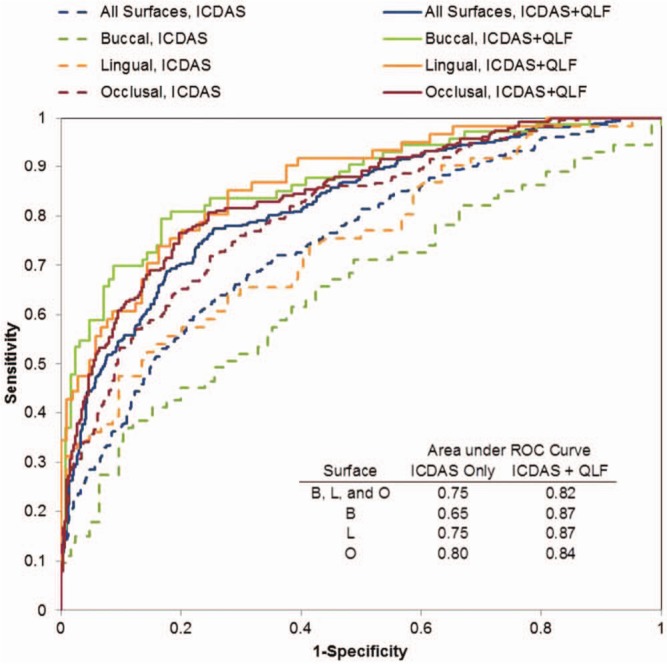
Receiver operating characteristic (ROC) curves to predict progression with and without the inclusion of QLF parameters.
QLF ∆F values were lower for ICDAS 0 than for all other scores (p = .0298 vs. ICDAS 1 active, p < .0001 vs. all others); lower for ICDAS 1 active than for ICDAS 1 inactive (p = .0031) and for all higher scores (p < .0001); lower for ICDAS 1 inactive than for ICDAS 2 inactive (p = .0147), ICDAS 2 active (p < .0001), ICDAS 3 (p < .0001), and ICDAS 4 (p < .0001); and lower for ICDAS 2 inactive and ICDAS 2 active than for ICDAS 3 and ICDAS 4 (p < .0001) (Appendix Table 2). There was no difference between ICDAS 2 inactive and ICDAS 2 active. There was no difference among ICDAS 2 active or inactive and ICDAS 3 or 4.
Discussion
Detection of early lesions is the cornerstone for the modern management of dental caries. The ability to determine which of these early lesions will progress to cavitation and how fast they are progressing can provide the dentist with a quantifiable way to assess the efficacy of preventive approaches, essential for clinical decision-making.
Several clinical studies have used QLF (Tranaeus et al., 2001; Kambara et al., 2003; Meller et al., 2006; Karlsson et al., 2007). However, there are few reports of longitudinal studies with QLF that follow caries lesions longer than 6 mos (Ferreira Zandoná et al., 2000, 2003a; Kambara et al., 2003; Karlsson et al., 2007; Mattousch et al., 2007; van der Veen et al., 2007). The interpretation of QLF images without the aid of visual examinations is challenged by confounding effects, as previously reported (Pretty et al., 2006). To avoid this issue, we have proposed to combine the use of QLF with a visual criterion (ICDAS), to benefit from the high sensitivity of the QLF and high specificity of the visual method (Ferreira Zandoná et al., 2010). In this study, we report on the natural progression of dental lesions as monitored by QLF over a 4-year period.
The progression of dental lesions is not a continuous process; neither is there a single pathway that lesions follow. Lesions can progress to cavitation, arrest, or reverse (Backer Dirks, 1966; Ferreira Zandoná et al., 2012). Using the ICDAS criteria to follow the natural progression of dental lesions, we have found that surfaces that transition to moderate-sized lesions (ICDAS 3 or 4) are likely to progress to cavitation (Ferreira Zandoná et al., 2012). The activity of early lesions (ICDAS 1 and 2) was shown to be rather difficult to determine, since some lesions deemed inactive, by clinical signs, did progress to cavitation (Ferreira Zandoná et al., 2012). The results of the longitudinal analyses of the QLF images indicate that this methodology allows for the identification of the lesions that are progressing at an earlier stage than was clinically possible. That is, lesions that clinical assessment would indicate as progressing only when a moderate severity (ICDAS scores 3 and 4) is reached can be shown to be progressing by the rapid changes in QLF values at the early stages (ICDAS 1 and 2). In the early stages, lesions can be truly reversing or progressing, and there is also a higher variability on the calls (Nelson et al., 2011); however, by focusing the analyses on true progressions, it could be demonstrated that QLF was able to identify the surfaces that are likely to become cavitated.
Several studies have used QLF in vivo to evaluate differences between and among different fluoride products, indicating that the method can separate different treatment groups (Feng et al., 2007; Karlsson et al., 2007) or to follow lesions after removal of fixed orthodontic appliances, indicating the ability of the method to quantitate changes in the lesions (Mattousch et al., 2007; van der Veen et al., 2007). In the present study, the QLF parameters (∆F and ∆Q) were able to demonstrate the natural progression of dental caries and distinguish between lesions that progressed to cavitation and those that did not progress. Analysis of the data from the questionnaires indicated that approximately 90% of the study participants received a professional fluoride treatment at least once a year, but any potential impact was not included in the analyses. In vitro, QLF has been shown to have a good correlation with mineral loss, but this correlation did not hold when there was surface loss in a study of artificial lesions (Meharry et al., 2012). ICDAS score 3 is lesions with microcavitation or surface loss. In this clinical study, QLF was able to monitor the changes in the lesions that were scored as ICDAS 3 at baseline as well as the lesions scored as ICDAS 1 and 2, but with intact surfaces. An in vivo study that compared the ability of QLF and other methods to discriminate between and among ICDAS scores found, as in our study, that although the QLF values for each of the scores were statistically significantly different, the absolute value differences were relatively small and not likely to be of clinical significance (Rechmann et al., 2012). Additionally, the actual values provided by various devices can differ, as we have reported (Ferreira Zandoná et al, 2003b). This longitudinal off-site study caused considerable wear on the equipment, requiring different devices to be used, which may explain the drops observed in the ΔF values at -3 and -6 visits. Thus, it is more probable that the rapid changes will be more clinically significant in predicting progression than the actual values.
In conclusion, QLF is able to monitor changes in lesion severity and discriminate between lesions that are rapidly progressing and those that are arrested. The value of this technology may lie in its ability to follow lesions through time and determine changes, more than in providing a quantitative value that relates to a clinical score.
Supplementary Material
Acknowledgments
The authors thank the following individuals for their assistance: Ms. Sharon Gwinn, Ms. Myrna Hernandez, Ms. Melissa Mau, Ms. Mildred Riviera, Ms. Jennifer Tran, and Drs. Evaristo Delgado, Hafsteinn Eggertsson, and Pedro Hernandez and the supporting staffs at the Indiana University School of Dentistry, Oral Health Research Institute and University of Puerto Rico.
Footnotes
This study was supported by grant R01 DE017890-05 from the National Institute of Dental and Craniofacial Research, National Institutes of Health, Bethesda, MD, USA.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
A supplemental appendix to this article is published electronically only at http://jdr.sagepub.com/supplemental.
References
- Ando M, van Der Veen MH, Schemehorn BR, Stookey GK. (2001). Comparative study to quantify demineralized enamel in deciduous and permanent teeth using laser- and light-induced fluorescence techniques. Caries Res 35:464-470. [DOI] [PubMed] [Google Scholar]
- Backer Dirks O. (1966). Posteruptive changes in dental enamel. J Dent Res 45:503-511. [Google Scholar]
- Bader JD, Perrin NA, Maupomé G, Rush WA, Rindal BD. (2008). Exploring the contributions of components of caries risk assessment guidelines. Community Dent Oral Epidemiol 36:357-362. [DOI] [PubMed] [Google Scholar]
- Diniz MB, Boldieri T, Rodrigues JA, Santos-Pinto L, Lussi A, Cordeiro RC. (2012). The performance of conventional and fluorescence-based methods for occlusal caries detection: an in vivo study with histologic validation. J Am Dent Assoc 143:339-350. [DOI] [PubMed] [Google Scholar]
- Ekstrand KR, Martignon S, Ricketts DJ, Qvist V. (2007). Detection and activity assessment of primary coronal caries lesions: a methodologic study. Oper Dent 32:225-235. [DOI] [PubMed] [Google Scholar]
- Feng Y, Yin W, Hu D, Zhang YP, Ellwood RP, Pretty IA. (2007). Assessment of autofluorescence to detect the remineralization capabilities of sodium fluoride, monofluorophosphate and non-fluoride dentifrices. A single-blind cluster randomized trial. Caries Res 41:358-364. [DOI] [PubMed] [Google Scholar]
- Ferreira Zandoná A, van der Veen M, Stookey GK. (2000). Indiana pilot clinical study of quantitative light fluorescence. In: Proceedings of 4th Indiana Conference on Early Detection of Dental Caries II, May 19–22, 1999. Stookey GK, editor. Indianapolis, IN: Indiana University School of Dentistry, pp 219–230. [Google Scholar]
- Ferreira Zandoná A, Eggertsson H, Wefel J, Barry K, Ofner S, Eckert G. (2003a). Clinical validation study of QLF at Indiana. In: Early Detection of Dental Caries III: Proceedings of the 6th Indiana Conference. Stookey GK, editor. Indianapolis, IN: Indiana University School of Dentistry, pp. 363-373. [Google Scholar]
- Ferreira Zandoná A, Fontana M, Wefel J, Donly K, Segura A, Stookey GK. (2003b). An in vitro comparison study between QLF units. Caries Res 37:284-285. [Google Scholar]
- Ferreira Zandoná A, Santiago E, Eckert G, Fontana M, Ando M, Zero DT. (2010). Use of ICDAS combined with quantitative light-induced fluorescence as a caries detection method. Caries Res 44:317-322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferreira Zandoná A, Santiago E, Eckert GJ, Katz BP, Pereira de, Oliveira S, Capin OR, et al. (2012). The natural history of dental caries lesions: a 4-year observational study. J Dent Res 91:841-846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fontana M, Santiago E, Eckert GJ, Ferreira-Zandoná AG. (2011). Risk factors of caries progression in a Hispanic school-aged population. J Dent Res 90:1189-1196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinrich-Weltzien R, Kühnisch J, Ifland S, Tranaeus S, Angmar-Månsson B, Stosser L. (2005). Detection of initial caries lesions on smooth surfaces by quantitative light-induced fluorescence and visual examination: an in vivo comparison. Eur J Oral Sci 113:494-498. [DOI] [PubMed] [Google Scholar]
- Ismail AI, Sohn W, Tellez M, Willem JM, Betz J, Lepkowski J. (2008). Risk indicators for dental caries using the International Caries Detection and Assessment System (ICDAS). Community Dent Oral Epidemiol 36:55-68. [DOI] [PubMed] [Google Scholar]
- Jablonski-Momeni A, Stucke J, Steinberg T, Heinzel-Gutenbrunner M. (2012). Use of ICDAS-II, fluorescence-based methods, and radiography in detection and treatment decision of occlusal caries lesions: an in vitro study. Int J Dent 2012:371595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kambara M, Uemura M, Miyake T, Doi T, Nakashima S, Eckert GJ. (2003). Results of clinical trial of fluoride dentifrices using QLF. In: Early Detection of Dental Caries III. Stookey GK, editor. Indianapolis, IN: Indiana University. [Google Scholar]
- Karlsson L, Lindgren LE, Trollsås K, Angmar-Månsson B, Tranaeus S. (2007). Effect of supplementary amine fluoride gel in caries-active adolescents. A clinical QLF study. Acta Odontol Scand 65:284-291. [DOI] [PubMed] [Google Scholar]
- Kühnisch J, Ifland S, Tranaeus S, Hickel R, Stösser L, Heinrich-Weltzien R. (2007). In vivo detection of non-cavitated caries lesions on occlusal surfaces by visual inspection and quantitative light-induced fluorescence. Acta Odontol Scand 65:183-188. [DOI] [PubMed] [Google Scholar]
- Mattousch TJ, van der Veen MH, Zentner A. (2007). Caries lesions after orthodontic treatment followed by quantitative light-induced fluorescence: a 2-year follow-up. Eur J Orthod 29:294-298. [DOI] [PubMed] [Google Scholar]
- Meharry MR, Dawson D, Wefel JS, Harless JD, Kummet CM, Xiao X. (2012). The effect of surface defects in early caries assessment using quantitative light-induced fluorescence (QLF) and micro-digital-photography (MDP). J Dent 40:955-961. [DOI] [PubMed] [Google Scholar]
- Meller C, Heyduck C, Tranaeus S, Splieth C. (2006). A new in vivo method for measuring caries activity using quantitative light-induced fluorescence. Caries Res 40:90-96. [DOI] [PubMed] [Google Scholar]
- Nelson S, Eggertsson H, Powell B, Mandelaris J, Ntragatakis M, Richardson T, et al. (2011). Dental examiners consistency in applying the ICDAS criteria for a caries prevention community trial. Community Dent Health 28:238-242. [PubMed] [Google Scholar]
- Pretty IA, Tavener JA, Browne D, Brettle DS, Whelton H, Ellwood RP. (2006). Quantification of dental fluorosis using fluorescence imaging. Caries Res 40:426-434. [DOI] [PubMed] [Google Scholar]
- Rechmann P, Rechmann BM, Featherstone JD. (2012). Caries detection using light-based diagnostic tools. Compend Contin Educ Dent 33:582-584, 586, 588-593. [PubMed] [Google Scholar]
- Shi XQ, Tranaeus S, Angmar-Månsson B. (2001). Comparison of QLF and DIAGNOdent for quantification of smooth surface caries. Caries Res 35:21-26. [DOI] [PubMed] [Google Scholar]
- Souza JF, Boldieri T, Diniz MB, Rodrigues JA, Lussi A, Cordeiro RC. (2012). Traditional and novel methods for occlusal caries detection: performance on primary teeth. Lasers Med Sci 28:287-295. [DOI] [PubMed] [Google Scholar]
- Tranaeus S, Al-Khateeb S, Björkman S, Twetman S, Angmar-Månsson B. (2001). Application of quantitative light-induced fluorescence to monitor incipient lesions in caries-active children. A comparative study of remineralisation by fluoride varnish and professional cleaning. Eur J Oral Sci 109:71-75. [DOI] [PubMed] [Google Scholar]
- van der Veen MH, Mattousch T, Boersma JG. (2007). Longitudinal development of caries lesions after orthodontic treatment evaluated by quantitative light-induced fluorescence. Am J Orthod Dentofacial Orthop 131:223-228. [DOI] [PubMed] [Google Scholar]
- Varma S, Banerjee A, Bartlett D. (2008). An in vivo investigation of associations between saliva properties, caries prevalence and potential lesion activity in an adult UK population. J Dent 36:294-299. [DOI] [PubMed] [Google Scholar]
- Zero DT, Zandoná AF, Vail MM, Spolnik KJ. (2011). Dental caries and pulpal disease. Dent Clin North Am 55:29-46. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.