

Abstract
Background:
The objectives of this study were to quantitatively assess the geographic heterogeneity of cancer prevalence in selected Western Countries and to explore the associations between its determinants.
Methods:
For 20 cancer sites, 5-year cancer prevalence, incidence, and survival were observed and age standardised for the mid 2000s in the United States, Nordic European Countries, Italy, Australia, and France.
Results:
In Italy, 5-year crude prevalence for all cancers was 1.9% in men and 1.7% in women, while it was ∼1.5% in all other countries and sexes. After adjustment for the different age distribution of the populations, cancer prevalence in the United States was higher (20% in men and 10% in women) than elsewhere. For all cancers combined, the geographic heterogeneities were limited, though relevant for specific cancers (e.g., prostate, showing >30% higher prevalence in the United States, or lung, showing >50% higher prevalence in USA women than in other countries). For all countries, the correlations between differences of prevalence and differences of incidence were >0.9, while prevalence and survival were less consistently correlated.
Conclusion:
Geographic differences and magnitude of crude cancer prevalence were more strongly associated with incidence rates, influenced by population ageing, than with survival rates. These estimates will be helpful in allocating appropriate resources.
Keywords: cancer prevalence, incidence, survival, ageing
Cancer prevalence indicates, at a given point in time, the number of persons living in a population after a cancer diagnosis (Capocaccia et al, 2002). Since prevalent cancer cases may have greater health needs than the general population, prevalence is a basic epidemiological measure for health planning and resource allocation helpful to estimate the impact of the expenditures for cancer on the health-care system.
Cancer prevalence depends on both the frequency of cancer (incidence) and its prognosis (survival). The higher the incidence and/or the better the survival, the larger the number of patients living with cancer. The ageing of the population increases the incidence of cancer, and hence it affects prevalence too. While reliable cancer incidence, mortality, and survival statistics are routinely available from cancer registries (Berrino et al, 2007; Engholm et al, 2010; Ferlay et al, 2010), estimates of prevalence are less frequently published (Engholm et al, 2010; AIHW, 2008; Colonna et al, 2008; Horner et al, 2009; Maddams et al, 2009; Guzzinati et al, 2012). Although estimates of prevalence are available at the Globocan website (Ferlay et al, 2010; Bray et al, 2012), systematic comparisons between prevalence in different countries are scanty and scarcely updated (Capocaccia et al, 2002; Micheli et al, 2002; Pisani et al, 2002; Verdecchia et al, 2002).
The first aim of the present paper was to compare prevalence of all cancers combined and for major cancer sites among countries where population-based cancer registry data on prevalence, incidence, and survival were recently published. These countries were the United States (Horner et al, 2009), Australia (AIHW, 2010), and some European countries – namely Nordic Countries (Engholm et al, 2010), Italy (AIRTUM Working Group, 2010), and France (Colonna et al, 2008). The second aim was to evaluate quantitatively the influence on geographic heterogeneity of determinants of prevalence such as incidence, survival, and age distribution. This evaluation could be helpful in defining important measures for the health-care systems (i.e., prevention, care pattern) and in allocating resources.
Materials and methods
In this study, we considered 5-year prevalence that represents the number of patients alive with a cancer diagnosed by <5 years. This period was taken into consideration as it is the time of highest demands on the oncology health services, including diagnosis, first treatment, and most intensive follow-up. Five-year prevalence was also fully comparable among different areas, as it was simply observed by the considered registries, and it was entirely based on incidence and follow-up data collected in the previously observed 5 years (Pisani et al, 2002).
Data used in the present study are summarised in Table 1. We collected incidence, 5-year survival, and 5-year prevalence data for the United States, Nordic European Countries (Denmark, Faroe Islands, Finland, Iceland, Norway, and Sweden), Italy, Australia, and France in the mid 2000s. Countries included in this study were representative of their areas with required estimates of incidence, survival, and prevalence available in the mid 2000s in quinquennia of age and for all age groups (0–99). For the United States, we selected data from the Surveillance, Epidemiology, and End Results (SEER) Program (SEER, 2012), including indicators for all races. For the Nordic Countries, data derived from NORDCAN (Engholm et al, 2010), for Italy, from the Italian Network of Cancer Registries – AIRTUM (Guzzinati et al, 2012), and for Australia, from the Australian Institute of Health and Welfare (AIHW, 2008, 2010). For France, we selected age-standardised incidence rates (1998–2002 period) from Cancer Incidence in Five Continents (Curado et al, 2007), 5-year age-standardised relative survival derived from EUROCARE-4 study (period of diagnosis: 1995–1999; cohort approach) (Berrino et al, 2007), and 5-year crude and age-standardised prevalence from a specific publication (Colonna et al, 2008).
Table 1. Cancer registries (CRs) included in the study, period of incidence, total number of incident cancer cases, population covered (and percentage on the total population of the country), period of survival, and year of prevalence.
| Country (CRs) | [Reference] website | Years of incidence | Incident cases | Average population (millions) | % Of country population covered by CRs | Survival period | Year of prevalence (1 January) |
|---|---|---|---|---|---|---|---|
| United States (SEER) |
[SEER, 2012] www.seer.cancer.gov |
1999–2003 |
623,439 |
27 |
10 |
1999–2003 |
2006 |
| Nordic European Countriesa (NORDCAN) |
[Engholm et al, 2010] www-dep.iarc.fr/NORDCAN.htm |
1999–2003 |
571,191 |
24 |
100 |
1999–2003 |
2006 |
| Italy (AIRTUM) |
[AIRTUM Working Group, 2010] www.registri-tumori.it |
1999–2003 |
464,262 |
16 |
28 |
1999–2003 |
2006 |
| Australia |
[AIHW, 2008, 2010] www.aihw.gov.au/acim-books |
1998–2002 |
437,793 |
19 |
100 |
1998–2004 |
2005 |
| France | [Colonna et al, 2008] | 1998–2002 | 183,136 | 8 | 12 | 1995–1999 | 2002 |
Abbreviation: SEER=Surveillance, Epidemiology, and End Results.
Denmark, Faroe Islands, Finland, Iceland, Norway, and Sweden.
Twenty malignant cancer sites based on International Classification of Disease, revision 10 (WHO, 1992) were included in the present comparison. The ‘head and neck' site was not considered due to its inconsistent definitions adopted in different countries, while ‘gallbladder' and ‘soft tissue' because data were not available for all the analysed countries.
Incidence rates and 5-year prevalence were standardised on the European standard population (18 age groups). Five-year survival was age standardised using the following age classes: 0–44, 45–59, 60–74, and ⩾75 years, using the International Cancer Survival Standard (ICSS) (Corazziari et al, 2004). Since no appreciable change in comparisons emerged when using the USA population as standard population, only the estimates based on the European standard population have been shown.
Using the SEER estimates (the largest population) as reference, the differences (Δ%) between the country-specific 5-year prevalence, incidence, and 5-year survival were calculated by sex and cancer site. The relationships between percentage differences of age-standardised 5-year prevalence (AP), age-standardised incidence (AI) and 5-year age-standardised relative survival (RS) were evaluated using the crude and weighted (by the number of incidence cases) Pearson's correlation coefficients. With the aim to calculate these correlations for all countries (i.e., including the United States), all the measures were rescaled and the differences were calculated vs the pooled estimates based on the average of the five countries.
Results
In the mid 2000s, Italy was the country showing the highest 5-year crude cancer prevalence among the sites combined, 1.9% among men and 1.7% among women (Web Appendix 1). They were 25–30% higher among men and 20–25% higher among women than those reported in other analysed countries, where corresponding proportions were ∼1.5% in men and 1.4% in women.
The above-described patterns of geographic differences in cancer prevalence were substantially modified by age standardisation (Web Appendix 2). Five-year age-standardised prevalence, age-standardised incidence, and 5-year age-standardised relative survival for the United States, Nordic Countries, Italy, Australia, and France are shown in Table 2 for men and in Table 3 for women.
Table 2. Five-year age-standardised prevalence (AP, per 100 000)a, age-standardised incidence rate (AI, per 100 000)a, and 5-year relative survival (RS)b in the United States (SEER), Nordic Countries (NORDCAN), Italy (AIRTUM), Australia, and France with differences (Δ%) in comparison with the corresponding estimates in the United States. MEN, all ages.
| |
|
Nordic Countries |
Italy |
Australia |
France |
||||
|---|---|---|---|---|---|---|---|---|---|
| Site (ICD10) | United States | Δ% | Δ% | Δ% | Δ% | ||||
|
All cancers excluding non-melanoma | |||||||||
| AP | 1655 | 1175 | −29 | 1405 | −15 | 1470 | −11 | 1271 | −23 |
| AI | 542 | 415 | −23 | 500 | −8 | 509 | −6 | 494 | −9 |
| RS |
67% |
55% |
−18 |
52% |
−22 |
58% |
−12 |
46% |
−31 |
|
Oesophagusc
(C15) | |||||||||
| AP | 12 | 7 | −43 | 7 | −42 | — | — | 18 | 51 |
| AI | 8 | 6 | −23 | 6 | −23 | — | — | 14 | 86 |
| RS |
17% |
9% |
−47 |
10% |
−43 |
— |
— |
12% |
−34 |
|
Stomach (C16) | |||||||||
| AP | 19 | 17 | −9 | 45 | 143 | 21 | 16 | 23 | 22 |
| AI | 10 | 12 | 19 | 26 | 152 | 13 | 29 | 14 | 40 |
| RS |
24% |
20% |
−18 |
30% |
24 |
24% |
1 |
23% |
−3 |
|
Colon and rectum (C18–C21) | |||||||||
| AP | 186 | 152 | −18 | 206 | 11 | 224 | 21 | 172 | −7 |
| AI | 58 | 51 | −13 | 64 | 10 | 71 | 22 | 60 | 2 |
| RS |
66% |
56% |
−16 |
59% |
−11 |
61% |
−8 |
57% |
−14 |
|
Liver (C22) | |||||||||
| AP | 11 | 4 | −65 | 31 | 170 | 8 | −30 | 15 | 30 |
| AI | 9 | 5 | −40 | 21 | 144 | 6 | −29 | 16 | 81 |
| RS |
11% |
6% |
−43 |
15% |
39 |
3% |
−69 |
8% |
−27 |
|
Pancreas (C25) | |||||||||
| AP | 10 | 8 | −21 | 11 | 11 | 7 | −27 | 7 | −28 |
| AI | 12 | 11 | −12 | 13 | 8 | 10 | −16 | 9 | −27 |
| RS |
5% |
4% |
−22 |
6% |
12 |
5% |
−16 |
8% |
44 |
|
Trachea, bronchus, and lung (C33–C34) | |||||||||
| AP | 95 | 51 | −46 | 95 | 0 | 63 | −34 | 99 | 4 |
| AI | 76 | 49 | −36 | 81 | 6 | 58 | −24 | 70 | −7 |
| RS |
14% |
10% |
−30 |
13% |
−6 |
11% |
−23 |
12% |
−13 |
|
Skin melanoma (C43) | |||||||||
| AP | 99 | 70 | −30 | 53 | −47 | 226 | 127 | 37 | −62 |
| AI | 23 | 16 | −29 | 12 | −47 | 53 | 132 | 11 | −53 |
| RS |
91% |
83% |
−9 |
80% |
−12 |
90% |
−1 |
82% |
−10 |
|
Prostate (C61) | |||||||||
| AP | 732 | 521 | −29 | 397 | −46 | 509 | −30 | 431 | −41 |
| AI | 176 | 120 | −32 | 88 | −50 | 119 | −32 | 122 | −30 |
| RS |
98% |
78% |
−21 |
87% |
−12 |
85% |
−13 |
78% |
−20 |
|
Kidney (C64–66, C68) | |||||||||
| AP | 62 | 33 | −46 | 68 | 10 | 45 | −28 | 50 | −20 |
| AI | 18 | 12 | −36 | 19 | 5 | 14 | −24 | 16 | −10 |
| RS |
63% |
52% |
−18 |
67% |
7 |
66% |
4 |
60% |
−5 |
|
Bladder (C67, D09.0, D30.3, 41.4) | |||||||||
| AP | 132 | 105 | −20 | 185 | 40 | 52 | −61 | 66 | −50 |
| AI | 34 | 31 | −7 | 50 | 48 | 18 | −46 | 23 | −32 |
| RS |
83% |
74% |
−11 |
78% |
−6 |
62% |
−25 |
63% |
−24 |
|
Brain (C70–C72) | |||||||||
| AP | 15 | 37 | 143 | 16 | 5 | 14 | −9 | 14 | −8 |
| AI | 8 | 13 | 59 | 9 | 14 | 8 | 3 | 7 | −12 |
| RS |
25% |
21% |
−16 |
21% |
−17 |
13% |
−47 |
17% |
−31 |
|
Thyroid (C73) | |||||||||
| AP | 21 | 8 | −61 | 26 | 25 | 14 | −35 | 16 | −21 |
| AI | 4 | 2 | −55 | 5 | 14 | 3 | −33 | 4 | −12 |
| RS |
92% |
79% |
−15 |
88% |
−5 |
88% |
−5 |
75% |
−18 |
|
Hodgkin lymphoma (C81) | |||||||||
| AP | 13 | 11 | −15 | 17 | 33 | 10 | −20 | 11 | −18 |
| AI | 3 | 3 | −19 | 4 | 29 | 2 | −22 | 3 | −14 |
| RS |
80% |
85% |
6 |
81% |
2 |
85% |
6 |
77% |
−4 |
|
Non-Hodgkin lymphoma (C82–C85, C96) | |||||||||
| AP | 78 | 48 | −38 | 62 | −21 | 66 | −16 | 38 | −51 |
| AI | 23 | 15 | −35 | 18 | −21 | 20 | −12 | 15 | −33 |
| RS |
62% |
55% |
−12 |
59% |
−5 |
62% |
−1 |
49% |
−21 |
|
Multiple myelomac
(C90)d | |||||||||
| AP | 18 | 14 | −20 | 19 | 5 | 19 | 3 | 16 | −9 |
| AI | 7 | 6 | −19 | 7 | 3 | 7 | 0 | 5 | −26 |
| RS |
37% |
36% |
−5 |
46% |
23 |
— |
— |
39% |
3 |
|
Leukaemias (C91–C95) | |||||||||
| AP | 47 | 35 | −25 | 34 | −27 | 42 | −9 | 34 | −27 |
| AI | 16 | 12 | −25 | 14 | −13 | 13 | −21 | 13 | −16 |
| RS | 48% | 56% | 15 | 45% | −7 | 48% | −1 | 51% | 5 |
Standardised on the European population.
Standardised on the International Cancer Survival Standards.
Unavailable data are represented by ‘—'.
C88 is also included in Italy (4.4% of C88 and C90 cases in men).
Table 3. Five-year age-standardised prevalence (AP, per 100 000)a, age-standardised incidence rate (AI, per 100 000)a and 5-year relative survival (RS)b in the United States (SEER), Nordic Countries (NORDCAN), Italy (AIRTUM), Australia, and France with differences (Δ%) in comparison with the corresponding estimates in the United States. WOMEN, all ages.
| |
|
Nordic Countries |
Italy |
Australia |
France |
||||
|---|---|---|---|---|---|---|---|---|---|
| Site (ICD10) | United States | Δ% | Δ% | Δ% | Δ% | ||||
|
All cancers excluding non-melanoma | |||||||||
| AP | 1320 | 1117 | −15 | 1233 | −7 | 1242 | −6 | 1094 | −17 |
| AI | 409 | 351 | −14 | 351 | −14 | 380 | −7 | 314 | −23 |
| RS |
64% |
59% |
−7 |
61% |
−4 |
64% |
0 |
60% |
−6 |
|
Oesophagusc
(C15) | |||||||||
| AP | 3 | 2 | −20 | 2 | −32 | — | − | 2 | −22 |
| AI | 2 | 2 | 0 | 1 | −47 | — | − | 2 | −2 |
| RS |
20% |
13% |
−35 |
13% |
−35 |
— |
− |
15% |
−23 |
|
Stomach (C16) | |||||||||
| AP | 10 | 10 | 1 | 25 | 160 | 10 | 6 | 10 | 7 |
| AI | 5 | 6 | 27 | 13 | 165 | 6 | 18 | 6 | 13 |
| RS |
30% |
23% |
−21 |
35% |
18 |
25% |
−15 |
31% |
4 |
|
Colon and rectum (C18–C21) | |||||||||
| AP | 142 | 124 | −13 | 135 | −5 | 157 | 10 | 108 | −24 |
| AI | 43 | 39 | −10 | 41 | −5 | 49 | 13 | 35 | −19 |
| RS |
67% |
60% |
−10 |
60% |
−10 |
62% |
−7 |
59% |
−12 |
|
Liver (C22) | |||||||||
| AP | 4 | 2 | −49 | 9 | 108 | 3 | −30 | 3 | −26 |
| AI | 3 | 3 | −19 | 7 | 126 | 2 | −39 | 3 | −12 |
| RS |
12% |
8% |
−37 |
16% |
29 |
10% |
−16 |
10% |
−16 |
|
Pancreas (C25) | |||||||||
| AP | 8 | 6 | −23 | 8 | −3 | 7 | −18 | 6 | −29 |
| AI | 9 | 9 | −3 | 9 | −1 | 8 | −16 | 6 | −38 |
| RS |
7% |
5% |
−35 |
9% |
29 |
5% |
−33 |
7% |
5 |
|
Trachea, bronchus, and lung (C33–C34) | |||||||||
| AP | 82 | 38 | −53 | 29 | −64 | 38 | −53 | 22 | −73 |
| AI | 50 | 27 | −46 | 18 | −64 | 26 | −48 | 12 | −76 |
| RS |
19% |
14% |
−27 |
17% |
−10 |
14% |
−25 |
17% |
−11 |
|
Skin melanoma (C43) | |||||||||
| AP | 73 | 77 | 6 | 54 | −26 | 168 | 131 | 47 | −36 |
| AI | 16 | 16 | 5 | 11 | −29 | 37 | 142 | 12 | −22 |
| RS |
95% |
90% |
−4 |
88% |
−7 |
94% |
0 |
87% |
−8 |
|
Breast (C50) | |||||||||
| AP | 532 | 483 | −9 | 517 | −3 | 488 | −8 | 515 | −3 |
| AI | 135 | 110 | −19 | 116 | −14 | 115 | −15 | 122 | −10 |
| RS |
91% |
85% |
−7 |
86% |
−5 |
88% |
−3 |
83% |
−8 |
|
Cervix uteri (C53) | |||||||||
| AP | 27 | 39 | 44 | 30 | 11 | 25 | −7 | 37 | 38 |
| AI | 8 | 10 | 26 | 7 | −8 | 8 | 0 | 9 | 23 |
| RS |
65% |
67% |
2 |
57% |
−13 |
72% |
10 |
67% |
2 |
|
Corpus uteri (C54) | |||||||||
| AP | 96 | 83 | −13 | 72 | −25 | 60 | −37 | 56 | −42 |
| AI | 25 | 20 | −19 | 17 | −32 | 15 | −39 | 15 | −41 |
| RS |
83% |
83% |
−1 |
77% |
−8 |
82% |
−2 |
73% |
−13 |
|
Ovary (C56) | |||||||||
| AP | 38 | 48 | 24 | 37 | −3 | 30 | −21 | 35 | −7 |
| AI | 14 | 16 | 17 | 13 | −6 | 11 | −20 | 12 | −13 |
| RS |
39% |
40% |
1 |
38% |
−3 |
40% |
1 |
35% |
−10 |
|
Kidney (C64–C66, C68) | |||||||||
| AP | 33 | 19 | −41 | 30 | −9 | 24 | −28 | 22 | −33 |
| AI | 9 | 7 | −28 | 8 | −11 | 7 | −23 | 7 | −22 |
| RS |
66% |
55% |
−17 |
68% |
3 |
66% |
0 |
63% |
−4 |
|
Bladder (C67, D09.0, 30.3, 41.4) | |||||||||
| AP | 33 | 29 | −12 | 34 | 4 | 13 | −60 | 9 | −73 |
| AI | 9 | 9 | 1 | 9 | 2 | 5 | −44 | 3 | −63 |
| RS |
80% |
68% |
−15 |
77% |
−3 |
55% |
−31 |
60% |
−25 |
|
Brain (C70–C72) | |||||||||
| AP | 13 | 54 | 326 | 12 | −5 | 10 | −18 | 16 | 26 |
| AI | 6 | 14 | 162 | 6 | 9 | 5 | −2 | 5 | −12 |
| RS |
30% |
23% |
−23 |
27% |
−11 |
13% |
−57 |
19% |
−37 |
|
Thyroid (C73) | |||||||||
| AP | 65 | 26 | −60 | 83 | 28 | 43 | −34 | 57 | −12 |
| AI | 12 | 5 | −63 | 14 | 14 | 8 | −33 | 12 | 0 |
| RS |
95% |
85% |
−10 |
92% |
−3 |
95% |
0 |
90% |
−5 |
|
Hodgkin lymphoma (C81) | |||||||||
| AP | 11 | 9 | −23 | 15 | 34 | 8 | −25 | 9 | −18 |
| AI | 2 | 2 | −21 | 3 | 25 | 2 | −21 | 2 | −11 |
| RS |
84% |
86% |
2 |
85% |
1 |
86% |
2 |
82% |
−2 |
|
Non-Hodgkin lymphoma (C82–85, C96) | |||||||||
| AP | 57 | 37 | −36 | 45 | −22 | 49 | −15 | 29 | −49 |
| AI | 16 | 11 | −31 | 13 | −17 | 14 | −7 | 10 | −35 |
| RS |
69% |
60% |
−13 |
60% |
−13 |
63% |
−10 |
53% |
−24 |
|
Multiple myelomac
(C90)d | |||||||||
| AP | 12 | 10 | −15 | 14 | 16 | 12 | −1 | 12 | −4 |
| AI | 4 | 4 | −14 | 5 | 14 | 4 | −2 | 4 | −16 |
| RS |
37% |
38% |
3 |
46% |
25 |
− |
− |
43% |
17 |
|
Leukaemias (C91–C95) | |||||||||
| AP | 28 | 24 | −16 | 22 | −21 | 27 | −5 | 23 | −19 |
| AI | 9 | 8 | −18 | 9 | −4 | 9 | −5 | 8 | −13 |
| RS | 49% | 61% | 24 | 45% | −8 | 47% | −3 | 52% | 6 |
Standardised on European population.
Standardised on the International Cancer Survival Standards.
Unavailable data are represented by ‘—'.
C88 is also included in Italy (4.0% of C88 and C90 cases in women).
Overall age-standardised 5-year prevalence for all cancer sites (excluding non-melanoma skin cancer) in the United States was 1655 per 100 000 men and 1320 per 100 000 women, largely higher than in other countries. In men, Australia ranked second with 11% lower proportions than in the United States, where prostate cancer represented 44% of all prevalent cases (732 per 100 000 or 0.7% of all men). The 5-year prevalence of prostate cancer was much lower in all the other countries, from 521 per 100 000 in the Nordic Countries to 397 per 100 000 in Italy (28% of all patients). The differences in prostate 5-year prevalence paralleled those seen in incidence, although the 5-year survival in the United States (98%) was markedly higher than elsewhere (78–87%) (Table 2). The highest age-standardised 5-year prevalence for all other cancers (prostate and non-melanoma skin cancer excluded) in men was observed in Italy (1 008 per 100 000), followed by Australia (961), United States (923), France (840), and Nordic Countries (654).
Among women, breast cancer represented 40% or more of diagnosed cancers (Table 3), and 5-year prevalence (∼0.5%) as well as 5-year survival rates (85–90%) were similar across countries. Corpus uteri and lung cancer were the third and fourth most prevalent cancer sites in USA women; in addition to non-Hodgkin lymphoma and leukaemia, they largely explained the overall higher prevalence among USA women.
In women, 5-year prevalence for lung cancer in United States (82 per 100 000) was two-fold higher than in all other countries. Between countries differences were of the same magnitude for age-adjusted incidence rates, while 5-year survival for lung cancer among USA women was slightly higher than elsewhere.
Patients with colorectal cancer represented >10% of all prevalence in each sex and country. Colorectal cancer prevalence was higher in Australia (both sexes) and in Italy (men) than in the United States, and lower in Nordic Countries and France. The geographic heterogeneity in incidence was of the same magnitude of that observed for 5-year prevalence, and 5-year relative survival ranged between 57% and 69% in all registries.
Among the selected countries, skin melanoma had the highest 5-year prevalence in Australia in both sexes (226 per 100 000 men and 168 per 100 000 women), due to the markedly higher incidence rates, while 5-year survival in Australia was as high as in the United States, and higher than in European countries.
Italy had the highest age-standardised prevalence for bladder (185 per 100 000 men and 34 per 100 000 women), kidney (68 per 100 000 men), thyroid (26 per 100 000 men and 83 per 100 000 women), stomach (45 per 100 000 men and 25 per 100 000 women), and liver (31 per 100 000 men and 9 per 100 000 women). For all these cancers, the excess in 5-year prevalence paralleled the one seen for incidence rates. In Nordic Countries, men had a lower 5-year prevalence (−29%) than in the United States for all the cancer sites combined. The difference was similar to the one seen for incidence (−23%) and, to a lesser extent, survival (−18%). The same pattern emerged in Nordic women with the exception of skin melanoma (77 per 100 000), ovarian cancers (48 per 100 000), and cervix uteri (39 per 100 000). In France, the 5-year prevalence was 20% lower than in the United States for all neoplasms, but it was higher for cancers of oesophagus, stomach, and liver for which France and Italy shared high incidence rates (Verdecchia et al, 2002). Five-year prevalence of cervical cancer was also 38% higher in France (37 per 100 000) than in the United States (27 per 100 000), though without any difference in survival. For most of the cancer sites, 5-year prevalence in Australia was lower than in the United States in both sexes, with the exception of melanoma (226 per 100 000 men and 168 per 100 000 women) and colorectal cancers (224 per 100 000 men and 157 per 100 000 women).
Correlation among prevalence, incidence, and survival
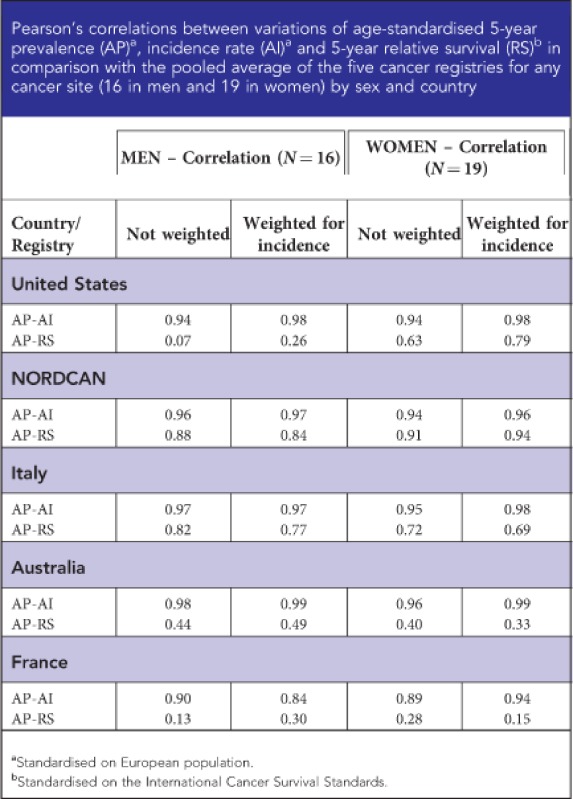
Figure 1 shows weighted correlations between differences of age-standardised 5-year prevalence, incidence rates, and 5-year relative survival, in comparison with the pool average of each indicator.
Figure 1.

Distribution of differences (vs Pooled average of the selected cancer registries) of age-standardised prevalence (AP)a, age-standardised incidence rates (AI)a, and 5-year relative survival (RS)b of major cancer sitesc in selected countries and Pearson's correlations (ρ)d. Each dot represents one cancer site.aStandardised on European population; bStandardised on the International Cancer Survival Standards; cCancer sites or types presented in Tables 2 and 3; dWeighted for the incidence of the specific cancer site or type.
In all countries, extremely high correlation coefficients (ρ>0.95) emerged between differences in 5-year prevalence and incidence in men and women (only in France ρ=0.84). There were lower correlations between differences in 5-year prevalence and survival both for men, particularly (ρ<0.50) in the United States, France, and Australia, and for women, in France and Australia (ρ<0.40). Correlations >0.80 between survival and prevalence emerged only for Nordic Countries. Crude correlation coefficients between differences in 5-year prevalence, incidence, and 5-year survival provided very similar results (Web Appendix 3). The correlation between incidence and 5-year survival was rather poor (ρ<0.50) in all countries and sexes (data not shown).
Discussion
In the examined countries, 5-year prevalence rates ranged from 1400 to 1900 per 100 000 men and from 1300 to 1700 per 100 000 women. This means that one every 60–70 persons of all ages living in the United States, Australia, and in European Countries in mid 2000s had a cancer diagnosis within the previous 5 years. For all cancers combined, the geographic differences were relatively modest, ranging from 1 per 50 men in Italy to 1 per 75 women in France. After adjustment for the different age distributions of the populations, 5-year prevalence in the United States was 20% higher than in other countries in men and 10% higher in women. These values represent nearly 50% an increase, in comparison with estimates conducted 10 years earlier (Pisani et al, 2002; Verdecchia et al, 2002).
Among men, the overall 5-year prevalence (crude and age standardised) and geographic heterogeneity were greatly influenced by prostate cancer prevalence, higher in the United States than in other countries. Between countries differences were of the same magnitude of those reported for prostate cancer incidence (>30% higher in United States than in other countries), which were mainly due to the different timing and extent of diffusion of the prostate cancer antigen (PSA) testing with its relevant impact on the economic burden of this disease (Roehrborn and Black, 2011).
In women, breast cancer accounted for 40% of the total prevalent cases. Small differences (<10%) in all the examined, as well as in other more developed countries (Maddams et al, 2009; Guzzinati et al, 2012), reflected limited geographic heterogeneity in both incidence rates (<20% differences) and survival (<10%) in the early 2000s. Female breast cancer incidence decreased in the United States since 2002 (SEER, 2012), it was stable in Australia (AIHW, 2010) and in Nordic Countries (Engholm et al, 2010), as well as in Italy after a long increasing period (Crocetti et al, 2010). The impact on incidence trends of different implementations of screening programs and the hormone replacement therapies (proportions and changes) across countries have been extensively explored (Canfell et al, 2008; Séradour et al, 2009; Verkooijen et al, 2009; Crocetti et al, 2010; Hofvind et al, 2012).
In both sexes, colorectal cancer was the second most prevalent cancer in almost all the analysed countries (Center et al, 2009). Between countries differences in prevalence were similar to those observed in incidence rates, with the highest age-adjusted 5-year prevalence reported in Australia (>30% higher than in France). In turn, differences in incidence rates were largely explained by uneven exposure to major risk factors for this neoplasm (i.e., high consumption of red meat and processed meat, substantial consumption of alcoholic drinks, body fatness, and abdominal fatness) (World Cancer Research Fund/American Institute for Cancer Research, 2007).
Prostate cancer accounts for >30% of prevalent cases in men and >40% in United States and Nordic Countries. A crucial role in prostate cancer epidemiology was played by PSA testing. The PSA testing was introduced in the United States at the beginning of the 1990s. The earlier PSA testing introduction and its quick and widespread diffusion, which caused a peak in prostate incidence in the early 1990s, explain the differences emerged in incidence and prevalence in comparison with other countries. Issues related to effectiveness of screening for prostate cancer (in terms of mortality reduction, quality of life, over diagnosis) are still debated (Schröder et al, 2012).
The proportion of women living after a lung cancer diagnosis in United States was nearly two-fold higher than in other countries as a consequence of the 50–70% higher incidence rate in the United States. This excess mirrored the proportion of smokers in the country 20 or more years before (IARC, 2004). Lung cancer incidence had just began to decrease among USA women (SEER, 2012) while it was still increasing among women in Italy (AIRTUM Working Group, 2010), Australia (AIHW, 2010), and Nordic Countries (Engholm et al, 2010).
Prevalence, incidence, and survival
Almost all the observed differences in 5-year prevalence of cancer seemed to be more influenced by the differences in incidence than those in survival, even if substantial differences in survival were reported in this study, as well as in other developed countries (Verdecchia et al, 2002; Coleman et al, 2008). In the United States, the highest 5-year prevalence for prostate, breast, corpus uteri, kidney (women) cancers, non-Hodgkin lymphoma, and leukaemia was strongly associated with higher incidence rates for the corresponding cancer sites. The outstanding role of incidence on prevalence was also clear when high prevalence of specific cancers emerged in some countries: e.g., melanoma and colon–rectum in Australia; stomach, liver, bladder, thyroid cancers, and Hodgkin lymphoma in Italy, cervix uteri and ovary in the Nordic Countries, and oesophagus in France.
The role of ageing on cancer prevalence
The study showed that geographic heterogeneity of cancer prevalence was greatly influenced by the age structure of the population examined and that, when interpreting geographic differences between countries, age standardization of prevalence becomes necessary. The population was younger in the United States and Australia, with a mean age of 38 years and 13% of people aged over 65 years, as compared with France and the Nordic countries (mean age: 40 years, 17% >65 years), and the oldest population was in Italy (mean age: 43 years, 20% of the population >65 years) (United Nations, 2012). This age distribution explained why 20–30% higher crude prevalence emerged in Italy in comparison with other examined countries (Crocetti et al, 2012). These excesses were equal to 4–5 additional prevalent cancer cases per 1000 men (i.e., similar to prostate cancer prevalence) and 3–4 additional prevalent cancer cases per 1000 women (i.e., similar to breast cancer prevalence).
Strength and limitations of the study
The major strength of the study was the comprehensive quantitative evaluation of all major indicators of cancer burden in selected cancer registries in the developed regions. Among the strengths of our study were the inclusion of updated estimates of prevalence (incidence and survival) of all malignant tumours for all ages and the comparison between countries using a reference population. In addition, the study took advantage of data collected by cancer registries according to an international protocol (http://cinportal.iarc.fr), with standard routine indicators of data completeness and quality (Curado et al, 2007; Ferlay et al, 2010).
The calendar years of available data were slightly different among the examined countries (Table 1). However, the impact of these discrepancies in the presented results seemed to be negligible. The present analysis includes comparisons of prevalence, incidence, and survival rates among the different countries. In general, interpretation of descriptive epidemiological studies should take into account possible differences in registration procedures, with particular attention on: (1) methods of cancer detection (affecting incidence); (2) types of treatment provided and access to treatment services (affecting survival); (3) cancer characteristics such as stage at diagnosis and histology type; and (4) coding practices, as well as accuracy and completeness of recording of all cancer cases. For bladder cancer, the comparison among countries may have been biased because the Nordic and some Italian cancer registries included also non-malignant cancers (Patriarca et al, 2001). This may have also been applied to cancers of the central nervous system (CNS), because Nordic Cancer registries included non-malignant cancers too, which, in adults, may be twice as frequent as malignant ones (CBTRUS, 2011).
Strictly speaking, prevalence is a function of overall survival, while in the present study relative survival was used because it was reported consistently in all countries. The impact of this approximation on correlation estimates, however, should be negligible.
Conclusions
Differences between countries of 5-year cancer prevalence were related to differences in incidence rates, strongly influenced by population ageing, and less strongly to differences in survival rates. This comprehensive comparison of 5-year prevalence, incidence, and 5-year survival is important to provide evidence for rational and appropriate resource allocations (Mariotto et al, 2006, 2011; Yabroff et al, 2008; Barlow, 2009), with particular priority to primary prevention of cancer (Micheli et al, 2009).
Acknowledgments
We thank the Cancer and Screening Unit of the Australian Institute of Health and Welfare for providing data for Australia and helpful comments. We also thank Mrs Luigina Mei for editorial assistance. This work was supported by the Italian Association for Cancer Research and by the Italian Ministry of Health (Programma Integrato Oncologia).
Web Appendix 1
Five-year crude prevalence rate (per 100 000, all ages) in the United States, Nordic Countries (NORDCAN), Italy, Australia, and France for the 10 most frequent types of cancer patients in each country.
Web Appendix 2
Five-year age-standardised prevalence (per 100 000, all ages) in the United States, Nordic Countries (NORDCAN), Italy, Australia, and France for the 10 most frequent types of cancer patients in each country.
Web Appendix 3
Appendix
Members of the AIRTUM working group
Antonella Zucchetto (Epidemiology and Biostatistics Unit, Aviano); Adele Caldarella (Tuscany Cancer Registry); Emanuela Bovo (Registro Tumori Veneto); Giovanna Tagliabue (Registro Tumori Varese, Fondazione IRCCS, Istituto Nazionale dei Tumori); Marina Vercelli (Liguria Cancer Registry at IRCSS AOU S.Martino-IST/UNIGE); Fabio Falcini (Romagna Cancer Registry); Giorgia Randi (Milan Cancer Registry); Saba Petrucci (Umbria Cancer Registry); Stefano Ferretti (Ferrara Cancer Registry); Fabio Pannozzo (Latina Cancer Registry); Lucia Mangone (Reggio Emilia Cancer Registry); Silvano Piffer (Trento Cancer Registry); Mario Fusco (Napoli Cancer Registry); Adriano Giacomin (Biella Cancer Registry); Francesco Tisano (Syracuse Province Registry); Maurizio Zarcone (Palermo Cancer Registry of Pathology).
The authors declare no conflict of interest.
Footnotes
Supplementary Information accompanies this paper on British Journal of Cancer website (http://www.nature.com/bjc)
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Supplementary Material
References
- AIRTUM Working Group Italian cancer figures, report 2010: Cancer prevalence in Italy. Patients living with cancer, long-term survivors and cured patients. Epidemiol Prev. 2010;34:1–188. [PubMed] [Google Scholar]
- AIHW (Australian Institute of Health and Welfare) Australian Cancer Incidence and Mortality Books. AIHW ACIM: Canberra; 2010. [Google Scholar]
- AIHW (Australian Institute of Health and Welfare), Cancer Australia & Australasian Association of Cancer Registries 2008Cancer Survival and Prevalence in Australia: Cancers Diagnosed from 1982 to 2004 Camberra: AIHW; Cancer Series no. 42. Cat. no. CAN 38. http://www.aihw.gov.au/publication-detail/?id=6442468141 (Accessed on 17 June 2013). [Google Scholar]
- Barlow WE. Overview of methods to estimate the medical costs of cancer. Med Care. 2009;47:S33–S36. doi: 10.1097/MLR.0b013e3181a2d847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berrino F, De Angelis R, Sant M, Rosso S, Bielska-Lasota M, Coebergh JW, Santaquilani M, EUROCARE Working group Survival for eight major cancers and all cancers combined for European adults diagnosed in 1995-99: results of the EUROCARE-4 study. Lancet Oncol. 2007;8:773–783. doi: 10.1016/S1470-2045(07)70245-0. [DOI] [PubMed] [Google Scholar]
- Bray F, Ren JS, Masuyer E, Ferlay J. Estimates of global cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer. 2012;132 (5:1133–1145. doi: 10.1002/ijc.27711. [DOI] [PubMed] [Google Scholar]
- Canfell K, Banks E, Moa AM, Beral V. Decrease in breast cancer incidence following a rapid fall in use of hormone replacement therapy in Australia. Med J Aust. 2008;188:641–644. doi: 10.5694/j.1326-5377.2008.tb01821.x. [DOI] [PubMed] [Google Scholar]
- Capocaccia R, Colonna M, Corazziari I, De Angelis R, Francisci S, Micheli A, Mugno E, EUROPREVAL Working Group Measuring cancer prevalence in Europe: the EUROPREVAL project. Ann Oncol. 2002;13:831–839. doi: 10.1093/annonc/mdf152. [DOI] [PubMed] [Google Scholar]
- CBTRUS 2011. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2004-2007. Source: Central Brain Tumor Registry of the United States, Hinsdale IL. Available at: /www.cbtrus.org/2011-NPCR-SEER/WEB-0407-Report-3-3-2011.pdf (Accessed on 17 June 2013).
- Center MM, Jemal A, Smith RA, Ward E. Worldwide variations in colorectal cancer. CA Cancer J Clin. 2009;59:366–378. doi: 10.3322/caac.20038. [DOI] [PubMed] [Google Scholar]
- Coleman M, Quaresima M, Berrino F, Lutz JM, De angelis R, Capocaccia R, Baili P, Rachet B, Gatta G, Hakulinen T, Micheli A, Sant M, Weir HK, Elwood JM, Tsukuma H, Koifman S, E Silva GA, Francisci S, Santaquilani M, Verdecchia A, Storm HH, Young JL, CONCORD Working Group Cancer Survival in five continents: a worldwide population-based study (CONCORD) Lancet Oncol. 2008;9:730–756. doi: 10.1016/S1470-2045(08)70179-7. [DOI] [PubMed] [Google Scholar]
- Colonna M, Danzon A, Delafosse P, Mitton N, Bara S, Bouvier AM, Ganry O, Guizard AV, Launoy G, Molinie F, Sauleau EA, Schvartz C, Velten M, Grosclaude P, Tretarre B. Cancer prevalence in France: time trend, situation in 2002 and extrapolation to 2012. Eur J Cancer. 2008;44:115–122. doi: 10.1016/j.ejca.2007.10.022. [DOI] [PubMed] [Google Scholar]
- Corazziari I, Quinn M, Capocaccia R. Standard cancer patient population for age standardising survival ratios. Eur J Cancer. 2004;40:2307–2316. doi: 10.1016/j.ejca.2004.07.002. [DOI] [PubMed] [Google Scholar]
- Crocetti E, Buzzoni C, Falcini F, Cortesi L, De Lisi V, Ferretti S, Tumino R, Russo A, Paci E. Disentangling the roles of mammographic screening and HRT in recent breast cancer incidence trends in Italy by analyses based on calendar time and time since screening activation. Breast J. 2010;16:350–355. doi: 10.1111/j.1524-4741.2010.00928.x. [DOI] [PubMed] [Google Scholar]
- Crocetti E, Buzzoni C, Quaglia A, Lillini R, Vercelli M, AIRTUM Working Group Ageing and other factors behind recent cancer incidence and mortality trends in Italy. J Geriatr Oncol. 2012;3:111–119. [Google Scholar]
- Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, Boyle P.2007Cancer Incidence in Five ContinentsVol. IX. IARC Sci. Publ. No. 160.IARC: Lyon [Google Scholar]
- Engholm G, Ferlay J, Christensen N, Bray F, Gjerstorff ML, Klint A, Køtlum JE, Olafsdóttir E, Pukkala E, Storm HH. NORDCAN-a Nordic tool for cancer information, planning, quality control and research. Acta Oncol. 2010;49:725–736. doi: 10.3109/02841861003782017. [DOI] [PubMed] [Google Scholar]
- Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer. 2010;46:765–781. doi: 10.1016/j.ejca.2009.12.014. [DOI] [PubMed] [Google Scholar]
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM.2010GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10 [Internet] IARC: Lyon; available at: http://globocan.iarc.fr (Accessed on 17 June 2013). [Google Scholar]
- Guzzinati S, Buzzoni C, De Angelis R, Rosso S, Tagliabue G, Vercelli M, Pannozzo F, Mangone L, Piffer S, Fusco M, Giacomin A, Traina A, Capocaccia R, Dal Maso L, Crocetti E, AIRTUM working group Cancer prevalence in Italy: an analysis of geographic variability. Cancer Causes Control. 2012;23:1497–1510. doi: 10.1007/s10552-012-0025-8. [DOI] [PubMed] [Google Scholar]
- Hofvind S, Sakshaug S, Ursin G, Graff-Iversen S. Breast cancer incidence trends in Norway—explained by hormone therapy or mammographic screening. Int J Cancer. 2012;130:2930–2938. doi: 10.1002/ijc.26280. [DOI] [PubMed] [Google Scholar]
- Horner MJ, Ries LAG, Krapcho M, Neyman N, Aminou R, Howlader N, Altekruse SF, Feuer EJ, Huang L, Mariotto A, Miller BA, Lewis DR, et al. 2009SEER Cancer Statistics Review, 1975-2006 NCI: Bethesda; http://seer.cancer.gov/csr/1975_2006/ based on November 2008 SEER data submission, posted to the SEER website (Accessed on 17 June 2013). [Google Scholar]
- IARC . Tobacco Smoke and Involuntary Smoking. IARC Monogr Eval Carcinog Risks Hum. Vol. 38. IARC: Lyon; 2004. [PMC free article] [PubMed] [Google Scholar]
- Maddams J, Brewster D, Gavin A, Steward J, Elliott J, Utley M, Moller H. Cancer prevalence in the United Kingdom: estimates for 2008. Br J Cancer. 2009;101:541–547. doi: 10.1038/sj.bjc.6605148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mariotto A, Yabroff RK, Feuer EJ, De Angelis R, Brown ML. Projecting the number of patients with colorectal carcinoma by phases of care in the US: 2000–2020. Cancer Causes Control. 2006;17:1215–1226. doi: 10.1007/s10552-006-0072-0. [DOI] [PubMed] [Google Scholar]
- Mariotto AB, Yabroff KR, Shao Y, Feuer EJ, Brown ML.2011Projections of the cost of cancer care in the United States: 2010-2020 J Natl Cancer Inst 103117–128.Erratum in: J Natl Cancer Inst 2011 Apr 20;103(8):699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Micheli A, Mugno E, Krogh V, Quinn MJ, Coleman M, Hakulinen T, Gatta G, Berrino F, Capocaccia R, EUROPREVAL Working Group Cancer prevalence in European registry areas. Ann Oncol. 2002;13:840–865. doi: 10.1093/annonc/mdf127. [DOI] [PubMed] [Google Scholar]
- Micheli A, Sanz N, Mwangi-Powell F, Coleman MP, Neal C, Ulrich A, Travado L, Santini LA, Grassi L, De Lorenzo F, Costa A, Dangou JM, Bisanti L, Seniori Costantini A, Abu-Rmeileh N, Kamal M, Federico M, Saracci R, Rennert G, Stefanini A, Cavalli F, Cazap E, Redmond K, O'Reilly S, Muti P, Casali P, Gatta G, Ferrari A, Koifman S, Bah E, Pastore G, Barr R, Lombardo C, Frazzingaro C, Ciampichini R, Baili P, ICCC-3 Session B Group International collaborations in cancer control and the third international cancer control congress. Tumori. 2009;95:579–596. doi: 10.1177/030089160909500502. [DOI] [PubMed] [Google Scholar]
- Patriarca S, Gafà L, Ferretti S, Vitarelli S, Cesaraccio R, Crocetti E, Ferrante M, Rollo P, Tagliabue G. Coding criteria of bladder cancer: effects on estimating survival. Epidemiol Prev. 2001;25:42–47. [PubMed] [Google Scholar]
- Pisani P, Bray F, Parkin DM. Estimates of the world-wide prevalence of cancer for 25 sites in the adult population. Int J Cancer. 2002;97:72–81. doi: 10.1002/ijc.1571. [DOI] [PubMed] [Google Scholar]
- Roehrborn CG, Black LK. The economic burden of prostate cancer. BJU Int. 2011;108:806–813. doi: 10.1111/j.1464-410X.2011.10365.x. [DOI] [PubMed] [Google Scholar]
- Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, Kwiatkowski M, Lujan M, Lilja H, Zappa M, Denis LJ, Recker F, Páez A, Määttänen L, Bangma CH, Aus G, Carlsson S, Villers A, Rebillard X, van der Kwast T, Kujala PM, Blijenberg BG, Stenman U-H, Huber A, Taari K, Hakama M, Moss SM, de Koning HJ, Auvinen A, for the ERSPC Investigators Prostate-cancer mortality at 11 years of follow-up. N Engl J Med. 2012;366:981–990. doi: 10.1056/NEJMoa1113135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SEER 2012. SEER*Stat Database: Incidence—SEER 9 Registries Research Data, Sub (1973-2006) www.seer.cancer.gov .
- Séradour B, Allemand H, Weill A, Ricordeau P. Changes by age in breast cancer incidence, mammography screening and hormone therapy use in France from 2000 to 2006. Bull Cancer. 2009;96:E16. doi: 10.1684/bdc.2009.0869. [DOI] [PubMed] [Google Scholar]
- United Nations 2012. United Nations 2010 estimates. http://esa.un.org/unpd/wpp/Excel-Data/population.htm (Accessed on 17 June 2013).
- Verdecchia A, Micheli A, Colonna M, Moreno V, Izarzugaza MI, Paci E, EUROPREVAL Working Group A comparative analysis of cancer prevalence in cancer registry areas of France, Italy and Spain. Ann Oncol. 2002;13:1128–1139. doi: 10.1093/annonc/mdf160. [DOI] [PubMed] [Google Scholar]
- Verkooijen HM, Bouchardy C, Vinh-Hung V, Rapiti E, Hartman P. The incidence of breast cancer and changes in the use of hormone replacement therapy: a review of the evidence. Maturitas. 2009;64:80–85. doi: 10.1016/j.maturitas.2009.07.015. [DOI] [PubMed] [Google Scholar]
- WHO . International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. World Health Organization: Geneva; 1992. [PubMed] [Google Scholar]
- World Cancer Research Fund/American Institute for Cancer Research . Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. AICR: Washington DC; 2007. [Google Scholar]
- Yabroff RK, Mariotto AB, Feuer EJ, Brown ML. Projections of the costs associated with colorectal cancer care in the United States, 2000–2020. Health Econ. 2008;17:947–959. doi: 10.1002/hec.1307. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.