

Abstract
WEBSITE FEATURE
A 40-year-old man with known hypertrophic cardiomyopathy presented with syncope after coughing. Physical examination revealed a systolic murmur that was accentuated by the Valsalva maneuver. An electrocardiogram suggested biventricular hypertrophy and biatrial enlargement (Fig. 1). Echocardiograms revealed asymmetric septal hypertrophy with a diastolic septal thickness of 2.3 cm, and evidence of flow acceleration across the right ventricular outflow tract (RVOT) and left ventricular outflow tract (LVOT) (Figs. 2 and 3).

Fig. 1 Electrocardiogram shows evidence of biventricular hypertrophy and biatrial enlargement.
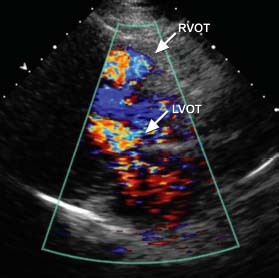
Fig. 2 Transthoracic echocardiogram (parasternal long-axis view) shows systolic flow acceleration across the right (RVOT) and left ventricular outflow tracts (LVOT).
Real-time motion image is available at www.texasheart.org/journal.
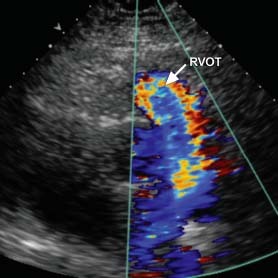
Fig. 3 Transthoracic echocardiogram (parasternal long-axis view) shows systolic flow acceleration across the right ventricular outflow tract (RVOT).
Real-time motion image is available at www.texasheart.org/journal.
Cardiac magnetic resonance images confirmed noncontiguous hypertrophy involving the basal septal, basal anterior, and apical walls of the left ventricle, as well as the inferior and free walls of the right ventricle (RV). A prominent muscle band in the RVOT contributed to dynamic obstruction across the RVOT (Figs. 4 and 5). Patchy hyperenhancement in the septum, visible in delayed-enhancement sequences after gadolinium administration, was consistent with myocardial fibrosis (Fig. 6). The subendocardium was not involved, suggesting a cause other than coronary disease.

Fig. 4 Cardiac magnetic resonance image shows noncontiguous left ventricular hypertrophy involving the basal septum and apex (arrows).
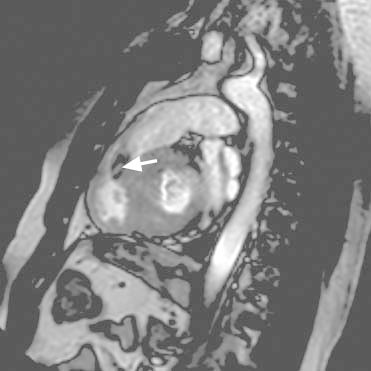
Fig. 5 Cardiac magnetic resonance image shows a hypertrophied muscle band in the right ventricular outflow tract contributing to dynamic obstruction indicated by flow acceleration (arrow).
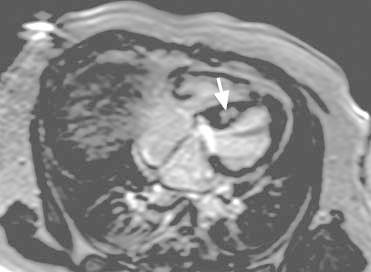
Fig. 6 Cardiac magnetic resonance image shows delayed enhancement in the interventricular septum after gadolinium administration (arrow), consistent with myocardial fibrosis that spares the subendocardium.
Angiography was performed to measure and characterize the gradient across the RVOT. There was a hemodynamically significant gradient of 54 mmHg (mean, 33 mmHg). When the patient coughed and then performed the Valsalva maneuver, the peak gradients increased to 94 mmHg and 106 mmHg, respectively. Potentiation of the peak gradient across the RVOT was observed after a premature ventricular contraction (Fig. 7). Because of the patient's unexplained syncope, a cardioverter-defibrillator was implanted for the primary prevention of sudden cardiac death. An atrial lead was also implanted to accommodate any future need for atrioventricular synchronous pacing. Transthoracic echocardiography was performed to evaluate the effect of RV pacing on the RVOT gradient. The peak gradient across the RVOT was 17 mmHg with RV pacing and 37 mmHg without RV pacing (Fig. 8).
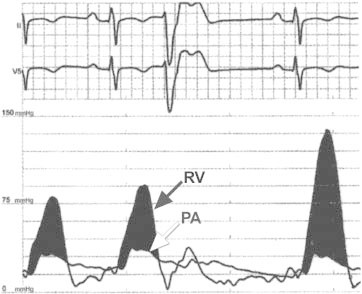
Fig. 7 Hemodynamic tracings from right-sided heart catheterization show simultaneous right ventricular (RV) pressure (across the RV outflow tract) and pulmonary artery (PA) tracings. This figure shows potentiation of the peak RV gradient (bottom tracing) after a premature ventricular contraction.
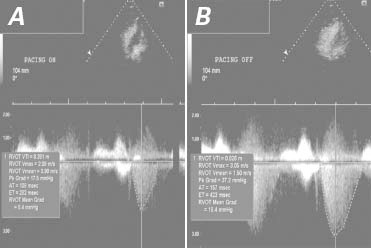
Fig. 8 Transthoracic echocardiograms show gradients across the right ventricular outflow tract. A) With pacing, the peak gradient was 17 mmHg at 72 beats/min. B) Without pacing, the peak gradient was 37 mmHg at approximately 72 beats/min.
AT = acceleration time; ET = ejection time; Grad = gradient; Pk = peak; RVOT = right ventricular outflow tract; Vmax = maximum velocity; Vmin = minimum velocity; VTI = velocity time integral
Comment
Right ventricular involvement has been reported in hypertrophic cardiomyopathy; however, its prevalence is variably described.1 Dual-chamber pacing has produced favorable hemodynamic effects in patients with symptomatic LVOT obstruction.2 In comparison, RV pacing reduced the gradient across our patient's RVOT.
Acknowledgment
We thank Dr. Richard Asinger for his help with hemodynamic evaluation and critical review of the manuscript.
Supplementary Material
Footnotes
Address for reprints: Sarah E. Nelson, MD, Department of Internal Medicine, Hennepin County Medical Center, 701 Park Ave., Minneapolis, MN 55415
E-mail: sthordse@gmail.com
References
- 1.Maron MS, Hauser TH, Dubrow E, Horst TA, Kissinger KV, Udelson JE, Manning WJ. Right ventricular involvement in hypertrophic cardiomyopathy. Am J Cardiol 2007;100(8): 1293–8. [DOI] [PubMed]
- 2.Fananapazir L, Epstein ND, Curiel RV, Panza JA, Tripodi D, McAreavey D. Long-term results of dual-chamber (DDD) pacing in obstructive hypertrophic cardiomyopathy. Evidence for progressive symptomatic and hemodynamic improvement and reduction of left ventricular hypertrophy. Circulation 1994;90(6):2731–42. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.