

SUMMARY
The crooked nose is unquestionably the most severe deformity of the nasal septum due to the simultaneous involvement of very important functional and aesthetic elements. As everyday interpersonal relations are primarily conducted face-to-face, deviation of the nasal pyramid from the median line is immediately obvious even to the least observant. The surgical procedures used to address this pathology must take into account the risk of relapse due to the elastic "memory" of the cartilage and avoid any undue weakening of the structure resulting in collapse of the nasal dorsum. The complexity of the problem requires techniques capable of addressing the situation radically and providing results that are stable over time. Extracorporeal septoplasty, spreader grafts and the crossbar graft are all particularly effective, not only in correcting deformity of the nasal pyramid but also in solving functional respiratory problems. The author describes the techniques in detail and discusses their strengths with respect to specific problems of the crooked nose.
KEY WORDS: Crooked nose, Extracorporeal septoplasty, Spreader grafts, Crossbar graft
RIASSUNTO
Il naso torto rappresenta senza dubbio l'espressione più grave della deviazione del setto nasale in quanto coesistono implicazioni funzionali ed estetiche di grande rilevanza. Infatti nei rapporti interpersonali quotidiani l'approccio "faccia a faccia" è quello più frequente e la deformità della piramide nasale rispetto alla linea mediana cattura immediatamente l'attenzione anche dell'osservatore meno attento. Le procedure chirurgiche utilizzate in questa patologia devono tenere conto del pericolo della recidiva, dovuto alla memoria elastica della cartilagine, e non devono indebolire esageratamente la struttura con conseguente crollo del dorso nasale. La complessità delle problematiche rende ragione della necessità di tecniche che affrontino radicalmente la situazione e che siano in grado di lasciare un risultato stabile nel tempo. In questa ottica risulta essere particolarmente efficace l'impiego della settoplastica extracorporea, degli spreader grafts, del crossbar graft che oltre a correggere la deformità della piramide nasale assicurano anche una soluzione al problema funzionale respiratorio. L'Autore descrive dettagliatamente le tecniche e ne discute i punti di forza nei confronti delle problematiche specifiche del naso torto.
Introduction
The term "crooked nose" is commonly used for all of the clinical conditions involving deviation of the nasal pyramid from the median line 1. In these cases, it can appear vaguely C-shaped or S-shaped or wholly displaced to one side or the other. The consequences for the patient are severe in both functional and aesthetic terms, as great difficulty in nasal respiration is always combined with unsightliness that cannot be hidden.
This pathology is frequently found in clinical practice today as the result of blunt trauma from sports or car accidents. Still more important than the social aspect of the crooked nose is its psychological impact on the person concerned. In our world, as we are all well aware, the face plays the crucial role in social relations as it is the first thing people see upon meeting. It is important for all of us to make a pleasing first impression on others in this sense, and the position of nose in the middle of the face means that any deviation is an unsightly element that immediately attracts attention. It is therefore easy to see that people with this type of deformity can be prey to severe complexes and insecurity.
Therapeutic problems
While it is clear from a social and aetiopathogenetic viewpoint that the crooked nose constitutes a problem of present-day relevance, it is not equally clear and widely known that the associated therapeutic problem lies essentially in the risk of relapse 2. In actual practice, what may appear to be a brilliant success immediately after surgery can be prove a failure a few months later on the reappearance of the deviation to some degree. This depends en tirely on the cartilaginous structures of the nasal pyramid, which retain the "memory" of the deviation due to their elasticity and tend to revert to their original position over time like a spring 3.
In physiopathological terms, this phenomenon is due to tissue deforming forces of an extrinsic and intrinsic nature that act on the cartilaginous nasal septum and cause relapse if they are not released during surgery.3 The extrinsic forces are those exerted on the septum by deviated nasal bones, upper lateral cartilages, and connections with the vomer, ethmoid and maxillary crest. The intrinsic forces can be the result of imperfect growth of the septal cartilage or from trauma altering the tissue ultrastructure, after which the deviated cartilaginous tissue always retains an inherent tendency to revert to its initial position.
The bony structures of the nasal pyramid also involved in the deviation remain in their new position once they have been repositioned in the centre. At most, double lateral osteotomy can prove useful to allow a greater degree of mobilization and ensure the elimination of all anatomical defects.
The difficulty in solving the problem of the crooked nose lies entirely in the cartilaginous structure, and especially the dorsal section of the nasal septum. While a deviated nasal septum can in fact be largely removed from a functional standpoint, it is necessary in any case to leave an L-shaped structure capable of supporting the nasal pyramid as a whole. In the case of the crooked nose, however, this structure must also be modified, as the deformity will otherwise remain present.
Another important therapeutic problem regards correction of the associated deformity of the upper lateral cartilages. The depression of the upper lateral cartilage on the concave side of the deviation is, in fact, often regarded as an indelible blemish even in cases where crookedness has been successfully corrected. The reason for this is the difficulty of reshaping these cartilaginous structures, which are of reduced thickness and consistency. At the same time, the exclusive use of onlay grafts to camouflage crookedness advocated by some authors often proves inadequate due to problems of resorption, and because it can contribute even more to collapse of the upper lateral cartilage.
Surgical techniques
Numerous techniques described in the literature involve the use of sections, incisions and morselization to modify the cartilaginous portion of the dorsal pillar of the septum and straighten the nose 4 5. Unfortunately, these methods often prove unsuccessful due to the above-mentioned "memory" of the deviation and to excessive weakening of the supporting pillar leading to collapse of the nasal dorsum. One technique offering good results involves extracorporeal reshaping of the nasal septum and grafting it back onto the nasal pyramid 6. In practical terms, the nasal septum is completely removed, reshaped and straightened outside the nose, replaced between the two mucoperichondrial flaps, and sutured into position inside the nose. This makes it possible to reorientate the nasal septum and secure a straight, reshaped part of it in a dorsal position. The drawback of the procedure lies in the practical difficulty of obtaining perfect alignment of the graft with the surrounding structures and the risk of mobility over time (Fig. 1).
Fig. 1.
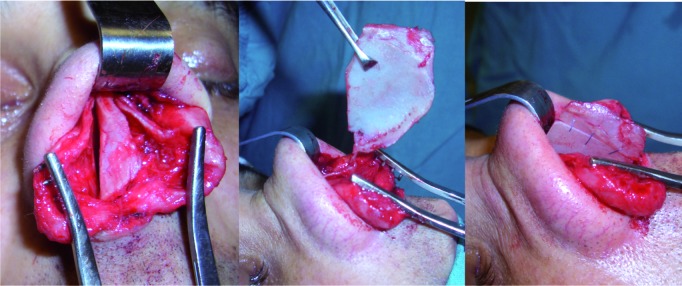
The Gubisch technique of extracorporeal reshaping of the nasal septum.
Considerable progress towards solving this problem came with the use of spreader grafts. The original technique devised by Sheen in 1984 involved positioning a rectangular strip of cartilage on either side of the dorsal septum harvested from the central part of the same 7. This method served fundamentally to strengthen the middle nasal vault during risky rhinoplasties, and hence prevent post-operative collapse. It also proved immediately useful in functional terms by broadening the angle of the internal nasal valve, and thus increasing respiratory airflow.
The technique was also used subsequently for support and splinting in cases of crooked nose. In practice, the graft taken from a straight central portion of the septum and sutured to its dorsal portion serves by virtue of its shape to counter the "cartilaginous memory" of the deviation. Its importance also relates to its role in strengthening the dorsal pillar, which makes it possible to make incisions for the purpose of reshaping with no risk of weakening the structure. The straight spreader graft is secured to the concave side of deviation in cases of C-shaped deviation of the dorsal septum (Fig. 2) and on the side opposite to the deviation, where there is an empty space between the septum and the upper lateral cartilages, in cases of linear deviation (Fig. 3). Many members of the most accredited schools of surgery in Europe and USA have used this method successfully in recent years to solve many of the problems regarding treatment of crooked nose 8-10. In the surgical protocol for this pathology, the same schools have adopted an open approach to the nasal pyramid, where a small columellar incision makes it possible to view all of the anatomical structures and suture the grafts precisely in position.
Fig. 2.
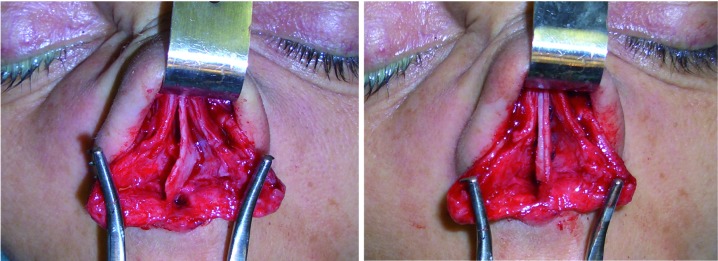
C-shaped deviation of the dorsal septum and its correction using a spreader graft on the concave side.
Fig. 3.
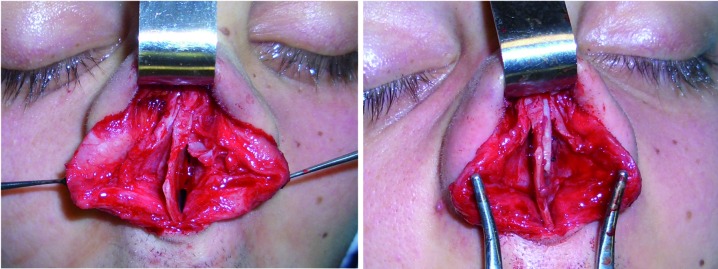
Linear deviation of the dorsal septum towards the right and its correction with a spreader graft on the opposite side.
This approach forms the background to the technique devised and published by the present author in 2003, which uses a "septal crossbar graft" to correct crooked nose 11. In practice, a rectangular graft of cartilage taken from a straight portion of the septum is embedded in the dorsal septum like a bar behind a door to prevent opening from the outside. The surgical technique involves the execution of a classical septoplasty, leaving in place an L-shaped structure of at least 15 mm in thickness, and the harvesting of a straight strip from the septum about 3-6 mm in height. A strip of cartilage from the vertical ethmoid plate can be used in revision rhinoplasties if no septal cartilage is available. Auricular cartilage is instead unsuitable for this technique due to its curvature and insufficient degree of robustness. Before insertion of the graft, it is necessary to make a series of incisions in the dorsal and caudal pillars of the L-shaped structure. Three incisions can be made for each of the two pillars, one on the inside and two on the outside at the points of greatest deviation. The next phase is insertion of the crossbar graft between the two incisions of the dorsal pillar on the concave side of the deviation (Fig. 4). Providing great anatomical stability and the maximum resistance to "cartilaginous memory" over time, this technique has proved particularly effective in the most severe cases of crooked nose.
Fig. 4.
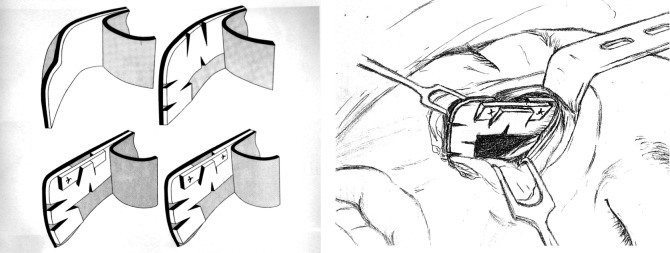
Diagrams for the correction of crooked nose using the Boccieri technique of the septal crossbar graft.
In these cases, a single spreader graft on the concave side may not provide sufficient thickness to correct the deformity. Moreover, the crossbar graft serves to open the internal nasal valve, which is collapsed on the concave side in these cases, to the evident functional benefit of nasal respiration 12 (Fig. 5).
Fig. 5.
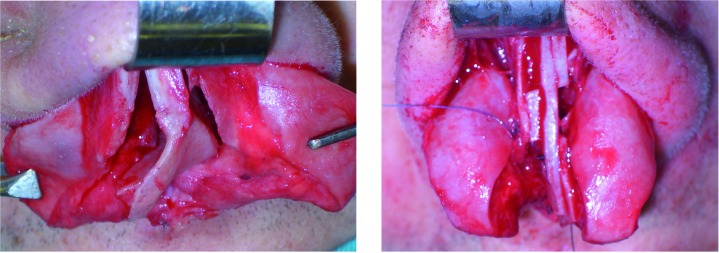
Dorsal deviation of the septum and its correction with a crossbar graft.
Fig. 6.
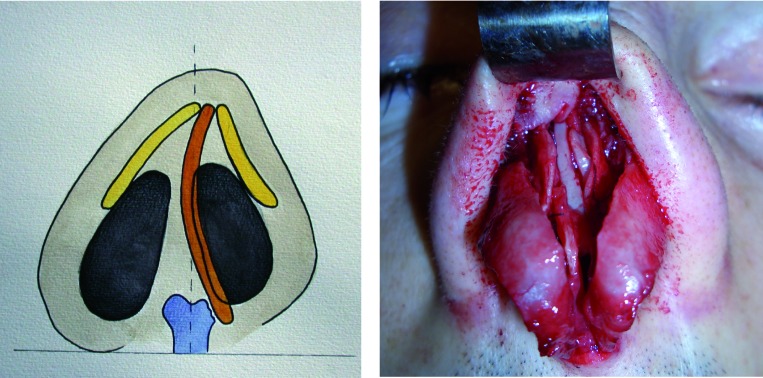
A. Schematic diagram showing the depression of the upper lateral cartilage on the concave side. B. Intraoperative photograph showing lateralization of the left upper lateral cartilage obtained with a septal crossbar graft.
Discussion
At present, there are essentially three techniques that can be considered to provide a lasting solution to dorsal deviation of the septum. The first is extracorporeal septoplasty, originally described by Galloway and Fomon and then adopted by Converse, Cottle, Rees, Sulsenti and Gubisch. The latter author developed an accentuated version that involves complete removal of the septum, reshaping with sutures and incisions to create a straight structure and grafting in place between the two flaps of the mucoperichondrium. A portion of the vertical ethmoid plate can be secured to one side of the "neo-septum" before insertion to make it straighter and sturdier. The technique offers a brilliant and radical solution to the problem of the crooked nose, but requires particular skill in the phase of reinsertion, and irregularity may remain in the area of the rhinion. In order to avoid this problem, Gubisch recommends systematic use of a suture between the upper lateral cartilages and the reshaped and replaced dorsal septum. This suture, which is very easy to perform in an open approach, reduces the risk of dorsal sagging from 1.5% to 0%.
The second is the use of spreader grafts. Toriumi and Ries suggested positioning a spreader graft on the concave side in C-shaped deviations both to restore the respiratory function and to harmonize the aesthetic line from the brow to the nasal tip. In cases of linear deviation of the nasal pyramid, it is instead necessary to position the spreader graft on the side opposite the deviation, where there is a gap between the septum and the upper lateral cartilages. In both cases, the use of spreader grafts makes it possible to secure lasting correction of the deviation and camouflage any residual crookedness. While Rohrich also supports of the technique of the unilateral spreader graft, Guyuron advocates the use of bilateral spreader grafts to counter the cartilaginous memory more firmly. Finally, Byrd suggests the use of a "septal extension graft" in place of the spreader graft on the concave side to control the projection and rotation of the nasal tip.
The spreader graft serves essentially as a splint on the dorsal septum while exerting lateral pressure from inside on the upper lateral cartilages. Use of an open approach makes it easy to suture the upper lateral cartilages to the septum and the spreader grafts previously placed in position. This last phase of the operation is important and should always be carried out to avoid curling of the upper lateral cartilages and associated post-operative deformity. While spreader grafts can be inserted in both a closed and open approach, the latter provides a clearer view of nasal structures and makes it possible to position and secure spreader grafts with greater ease and precision. It is of crucial importance to suture spreader grafts not only at the level of the caudal septum, but also in a more cephalic position. The latter suture is extremely difficult with the closed approach, but easy with the open.
The third technique for treatment of the crooked nose is the septal crossbar graft, introduced by the author in 2003, which is recommended above all for major deviations of the dorsal septum. The crossbar and spreader grafts share the same underlying philosophy, being both designed to strengthen the dorsal pillar of the L-shaped structure and make it possible to straighten and reshape the latter using multiple incisions with no risk of weakening it unduly.
The insertion of the septal crossbar graft entails use of the open approach both because great visibility and precision are required, and because sutures are needed in areas that cannot be reached with the closed approach. While the septal crossbar graft can be regarded as an intra-septal spreader graft, it makes it possible to double the space between the septum and the upper lateral cartilages compared to a single spreader graft. The septal crossbar graft is particularly useful in the correction of severe septal deviation and ensures the greatest degree of resistance to cartilaginous memory. In practical terms, it can be indicated when the distance of the point of greatest deviation of the nasal pyramid from the median line is more than 5 mm.
In such cases, a single spreader graft on the concave side may not provide sufficient thickness to correct the deformity. Moreover, the crossbar graft works effectively to open the internal nasal valve, which is collapsed on the concave side in these cases, and thus has an evident and important beneficial effect on nasal respiration. The procedures employing the spreader graft or crossbar graft are, in fact, very useful in improving respiratory functionality by establishing a correct angle of the internal nasal valve. It should be stressed that depression of the upper lateral cartilage on the concave side is often regarded as an indelible blemish in cases of crooked nose that can be successfully corrected with other techniques. This is due to the difficulty of reshaping these comparatively thin and flimsy cartilaginous structures. At the same time, the onlay grafts used by some surgeons to mask such forms of residual deformity often prove ineffective because of resorption problems and the fact that they are conducive to collapse of the upper lateral cartilage. The septal crossbar graft, however, produces upward pressure thrust that physiologically repositions and supports the upper lateral cartilage, which thus becomes capable of bearing small onlay grafts should they prove necessary (Fig. 5).
Conclusions
The crooked nose is still a difficult challenge even to expert surgeons. Progress in surgical techniques has made it possible to employ procedures that are more radical than in the past, and capable of eliminating the most common complications, such as insufficient treatment, structural weakening and relapse 13. We refer in particular to the use of extracorporeal septoplasty, spreader grafts and the septal crossbar graft, which offer satisfactory and longlasting results, but must be combined with sophisticated manual skills. This in no way rules out the supplementary use of other less invasive procedures to obtain even better results, such as small onlay grafts of morselized cartilage. The open approach has is also very helpful in treatment of crooked nose by improving intraoperative appraisal and facilitating suturing of grafts.
Appendix 1: clinical cases
Case 1
Patient age 24 years presenting a small osteocartilaginous hump with deviation to the right of the nasal pyramid as a whole. The caudal septum was considerably out of position and clearly visible in the right nostril. Rhinoplasty was performed involving excision of the hump and osteotomies. The deviation of the dorsal septum was addressed using extracorporeal reshaping of the cartilaginous septum, which was then sutured back in place between the two flaps of the mucoperichondrium.

Case 2
Patient age 22 years presenting a cartilaginous hump with bulbous nasal tip and deviation to the right of the lower two thirds of the nasal pyramid. Rhinoplasty carried out with hump excision and osteotomies, reshaping of the nasal tip and suturing of the domus. Application of a spreader graft on the left side of the dorsal septum resulted in realignment of the nasal pyramid with the median line. (The patient was operated on in the live surgery section of the 7th edition of "Nose and Surroundings Course" in 2007).

Case 3
Patient age 23 years presenting a small cartilaginous hump with C-shaped deviation of the nasal pyramid, the distance of the point of greatest deviation from the median line being over 5 mm. Rhinoplasty was performed involving hump excision and osteotomies. The application of a septal crossbar graft on the right side of the dorsal septum proved successful in correcting the severe deviation of the nasal pyramid.

References
- 1.Micheli Pellegrini V. Il naso torto. Padova: La Garangola; 1985. [Google Scholar]
- 2.Byrd HS, Salomon J, Flood J. Correction of the crooked nose. Plast Reconstr Surg. 1998;102:2148–2157. doi: 10.1097/00006534-199811000-00055. [DOI] [PubMed] [Google Scholar]
- 3.Courtiss EH. Septorhinoplasty of the traumatically deformed nose. Ann Plast Surg. 1978;1:443–452. doi: 10.1097/00000637-197809000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Lawson W, Reind AJ. Correcting functional problems. Facial Plast Surg Clin North Am. 1994;2:501–520. [Google Scholar]
- 5.Gomulinski L. La traduction morphologique des deformations septales. Leur correction au cours des rhinoplasties complexes. Ann Chir Plast. 1982;27:343–349. [PubMed] [Google Scholar]
- 6.Gubisch W. The extracorporeal septum plasty: a technique to correct difficult nasal deformities. Plast Reconstr Surg. 1995;95:672–682. doi: 10.1097/00006534-199504000-00008. [DOI] [PubMed] [Google Scholar]
- 7.Sheen JH. Spreader graft: A method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. 1984;73:230–237. [PubMed] [Google Scholar]
- 8.Toriumi DM, Ries WR. Innovative surgical management of the crooked nose. Facial Plast Clin North Am. 1993;1:63–78. [Google Scholar]
- 9.Vinayak BC, Trenitè GJN. External rhinoplasty. FACE. 1997;5:77–92. [Google Scholar]
- 10.Rohrich RJ. Rhinoplasty. Dorsal reduction and spreader graft. Dallas, Rhinoplasty Symposium. 2000;17:153–166. [Google Scholar]
- 11.Boccieri A, Pascali M. Septal crossbar graft for the correction of the crooked nose. Plast Reconstr Surg. 2003;111:629–638. doi: 10.1097/01.PRS.0000042205.27330.E4. [DOI] [PubMed] [Google Scholar]
- 12.Boccieri A. Evolution of the septal crossbar technique. Facial Plast Surg. 2006;22:255–265. doi: 10.1055/s-2006-954844. [DOI] [PubMed] [Google Scholar]
- 13.Sykes JM, Kim J, Shaye D, et al. The importance of the nasal septum in the deviated nose. Facial Plast Surg. 2011;27:413–422. doi: 10.1055/s-0031-1288928. [DOI] [PubMed] [Google Scholar]