

Abstract
Objective The endonasal endoscopic approach is currently under investigation for perisellar tumor surgery. A higher resection rate is to be expected and nasal complications should be minimized. Here, the authors report their technique of transnasal endoscopic neurosurgery after 218 procedures.
Methods Between October 2000 and September 2011, 210 patients received 218 endoscopic endonasal transsphenoidal procedures for perisellar lesions. Procedures were video recorded. The surgical technique was carefully analyzed. These cases were prospectively followed.
Results Standard technique was mononostril approach with 0-degree optics. 30-degree and—after availability—45-degree optics were used for assessment of radicality. On follow-up, magnetic resonance imaging revealed radical tumor resection in 94 out of 104 cases (90.3%). Recurrent tumor growth was observed in five younger patients (2.2%). There was no mortality and a low complication rate. Three patients (1.4%) complained postoperatively of nasal congestion or reduced nasal air flow; however, no complaints were considered to be severe.
Conclusion In comparison with other literature reports, the results are comparable or even better with respect to surgical radicality. The very low rate of nasal complaints is particularly remarkable. The technique has been shown to be safe and successful with a high radicality and only minor complications.
Keywords: endoscopy, mononostril, endonasal transsphenoidal approach, sellar lesions
Introduction
The microsurgical transsphenoidal approach was investigated and further established over almost a century of continuous research.1 Today it represents the gold standard for surgical treatment of sellar lesions.2,3,4,5,6 However, further developments of endoscopic techniques and their applications in neurosurgery7,8,9,10,11,12,13,14,15,16 have also influenced transnasal approaches, and continuous efforts to improve surgical techniques are still being made.17,18,19,20,21,22,23,24 An endonasal microscopic technique has been reported as an alternative to sublabial or septal incisions.25,26,27 However, despite these remarkable reports, current surgical strategies for transnasal approaches to the sellar region are diverging. Some surgeons still consider nasolabial approaches,26,28,29,30 others use an endonasal microscopic approach,27 and a third group of clinical researchers approach the region via an endonasal route under endoscopic view.17,18,19,23,24,25,31,32 The authors of the present study have applied the endoscopic technique for an endonasal approach of the sellar region since 1997. During this time, a distinct surgical technique was developed. Here, the results of this distinct surgical technique applied in 218 procedures since October 2000 are presented.
Clinical Material and Method
Patient Criteria
Between October 2000 and September 2011, 210 patients with pituitary adenomas and several other sellar and perisellar lesions underwent 218 procedures via an endonasal endoscopic transsphenoidal approach in its presented form at the Department of Neurosurgery of the University of Greifswald, University of Mainz, Saarland University, and Hannover Nordstadt Hospital. Twenty-one procedures for pituitary adenomas were performed by the authors as live surgery cases during neuroendoscopic workshops abroad in other European, Arabian, and Asian countries. All procedures were performed by one of the authors. The patient population consisted of 101 males and 109 females. The mean age at surgery was 58 years with a range of 23 to 83 years. A total of 151 patients could be prospectively followed.
Histology
The histological diagnoses included 152 endocrine inactive pituitary macroadenomas, 11 Rathke cleft cysts, 3 clivus chordomas, 1 osteolipoma, and 1 mucocele. Two patients had posttraumatic cerebrospinal fluid (CSF) fistula with encephalocele. Forty-one pituitary adenomas were hormone-secreting (28 growth hormone, 8 prolactinomas, 5 Cushing disease). Eighteen patients had recurrent tumor growth and underwent surgery having previously had transsphenoidal surgery. Five of these were recurrent cases having previously undergone surgery at our department with the endoscopic technique. Thirteen of the recurrent cases had surgery at another hospital and were referred to us for the recurrent procedure.
Perioperative Management
All patients underwent preoperative endocrine and visual function evaluations, including formal visual field testing. Postoperative visual evaluations were performed only in patients who showed preoperative visual impairment or presented visual symptoms postoperatively. Preoperatively and postoperatively, all patients received endocrine evaluations by an endocrinologist. The postoperative visits were performed during the patients' in-hospital stay within the first week after surgery and 6 weeks after surgery, followed by a variable time schedule depending on their hormonal findings. Preoperative and postoperative magnetic resonance imaging (MRI) was obtained as a routine. Also as a routine, a computed tomography (CT) scan with axial and coronal reformations was performed to define the bony boundaries of the sellar region, including the sphenoid cavity. If an MRI was not applicable, only CT was performed. All patients received a perioperative “stress dose” of hydrocortisone. Prophylactic antibiotic agents were administered routinely.
Surgical Technique
As a standard, all surgeries were performed in general anesthesia with orotracheal intubation. The procedures in the sellar region, and also the nasal approaches, were performed by the authors without collaboration from ear, nose, and throat (ENT) surgeons. The patient was maintained supine with the upper part of the body slightly elevated to ∼20 degrees and the head tilted to the left. The patient's head was fixed with a three-pin head-fixation system. Lateral fluoroscopy (C-arm) was routinely used for intraoperative imaging. MRI- or CT-based neuronavigation was administered (Fig. 1). The nose and the nasal cavities were prepared with application of a nasal decongestant and an alcohol-based disinfectant. The periumbilical abdomen was also prepared for fat graft harvesting. The patient, the C-arm, and the endoscopic equipment were sterile draped. For a detailed description of the endoscopic technique, please refer to the results section. After surgery, all patients were kept overnight at the intermediate car or intensive care unit. Patients were discharged within the first week after surgery unless complications occurred.
Figure 1.
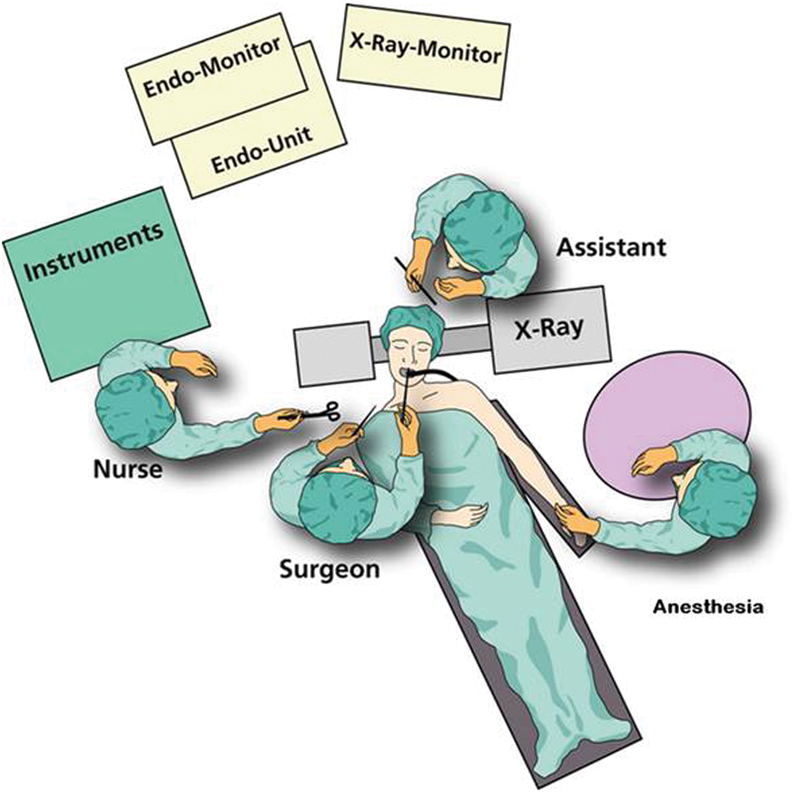
Positioning of the patients and endoscopy set up. Note that the endoscope is fixed in the holder, which is attached to the table on the right side of the patient. With this setting, the surgeon has two hands free for intraoperative maneuvers such as suction/irrigation and tumor resection.
The endoscopic equipment consisted of a series of various rigid-rod lens Hopkins optics, a xenon cold light source, a digital one-chip camera, a high-resolution video monitor screen, and a digital recording system (AIDA). All equipment was provided by Karl Storz Company (Tuttlingen, Germany). All procedures were video recorded. The surgical technique was carefully analyzed. Special attention was paid to the application of various optics, necessity of switching to the microscope, complications, advantages and disadvantages of the endoscopic technique, helpfulness of neuronavigation, surgical radicality, symptom relief, and postsurgical nasal complaints.
Postoperative Follow-Up
All patients were prospectively followed up (2 weeks to 8 years; mean 4.61 years) for this study until they were lost to follow-up in the outpatient clinic or, alternatively, with telephone interview. Follow-up examinations in outpatient clinic were performed at 3 months postoperatively and then on a yearly basis. The patients obtained a clinical investigation at 3 months postoperatively for nasal complaints and a postoperative MRI as control of radicality. The complications and nasal complaints during the postoperative hospital stay were investigated and documented in the chart by the authors. Nasal complaints at 3 months postoperatively were assessed and documented in the chart by physicians in the outpatient clinic during a routine follow-up. In some cases, the patients had ENT treatment because of nasal complaints. In these cases, the complaints were added retrospectively to our data.
Results
Detailed Account of Our Endoscopic Surgical Technique
As mentioned in the previous section, neuronavigation and lateral fluoroscopy were used as a routine. Neuronavigation was considered helpful in approaches through very asymmetric or atypical sphenoid cavities. Particularly useful was the neuronavigation in the approach to parasellar lesions like traumatic CSF fistula and to the approach of very small lesions such as the five macroadenomas. The lateral fluoroscopy was used in all cases for rapid orientation during surgery (Fig. 2A-D). A one-nostril approach was used in all patients. If possible, the approach was performed through the right nostril with the surgeon on the right side of the patient. An approach via the right nostril is far more convenient because the surgeon stands on the right side of the patient. This gives the surgeon the advantage of fixing the endoscope on the holder on the right side of the table, working with suction and irrigation in the left hand and performing the bone resection or tumor extirpation with the right—usually dominant—hand (Fig. 1). In our experience, this is the most convenient set up for a right-handed surgeon. If the right nostril is too narrow or the lesion is far more easily approached from the left, the left nostril is used. The latter approach occurred in eight cases so far. Reasons for the left-sided approach were septum deviation or a very narrow right nostril. All but two of the endoscopic transsphenoidal operations presented in the study were performed via an endonasal technique with the use of a nasal speculum; in two cases, the surgery was initially done as free nasal endoscopy, but later on a speculum was inserted after opening the sphenoid sinus to facilitate the use of the instruments. For surgery, 4-mm or 2.7-mm rigid endoscopes with Hopkins optics and 0 degree-angled optics were used for the approach and subsequent tumor removal. Scopes with 30 degree- and 45 degree-angled optics (the latter available since 2005) were employed for final inspection to improve radicality in macroadenomas and for tumor removal; this was especially useful if “a look around the corner” was required, such as in cavernous sinus or other far lateral located tumors. The surgical instruments were inserted adjacent to the endoscope through the same nostril. In most cases, a hydroflow device for irrigation and suction was used. In some cases, the lens cleaning irrigation-suction system (Clear Vision Device, Karl Storz Company) was applied.
Figure 2.
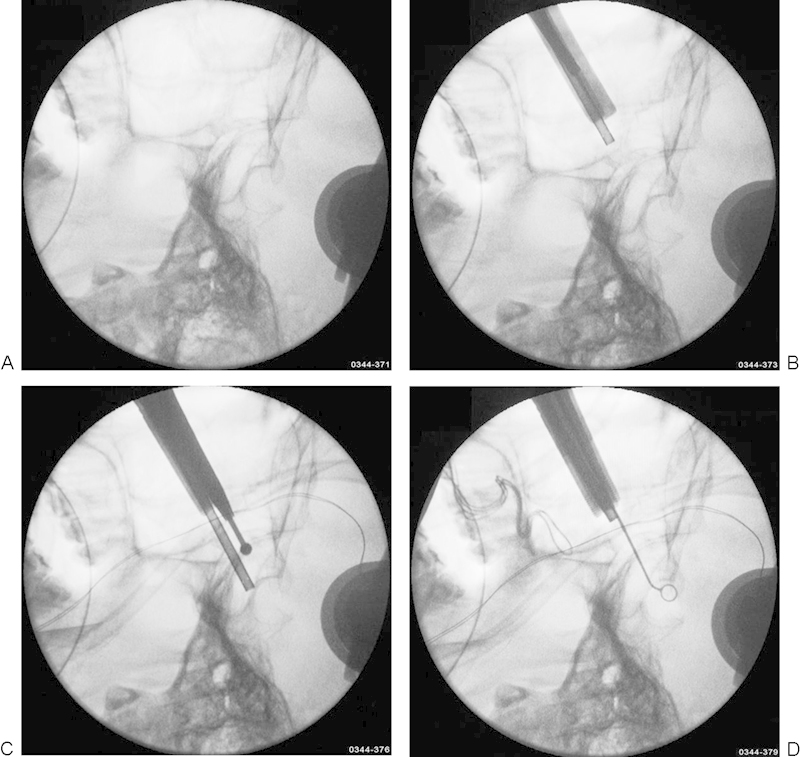
(A) Preoperative lateral fluoroscopy (C-arm) for depiction of the sella region. (B, C) Intraoperative lateral fluoroscopy for rapid orientation during opening the sphenoid floor. (D) Lateral fluoroscopy for orientation at the final removal of the lesion.
Our surgical standard procedure is performed as follows: after disinfection and vasoconstriction, the procedure starts with the endoscopic inspection of the nasal cavity. At the beginning—for inspection—the endoscope equipped with the 0-degree optics is held by the dominant (usually right) hand of the surgeon. Irrigation and suction is performed with the nondominant (usually left) hand. The nostril for the approach is chosen (Fig. 3A), after which the speculum is carefully inserted by the left hand under direct endoscopic control until it reaches the middle turbinate. It is further advanced, passing the inferomedial aspect of the middle turbinate under lateral fluoroscopy, to the sellar floor until the sphenoid sinus is reached. The nose is carefully dilated in several steps. With this use of the speculum, the nasal mucosa can be preserved through the whole surgical procedure, and almost any mucosal bleeding can be prevented. We consider the use of the speculum the first crucial step in our technique. After insertion of the speculum, the endoscope is then put in an endoscope holder. The sphenoid ostium is localized at the recessus sphenoethmoidalis (Fig. 3B). The septal mucosa is coagulated, incised, and mobilized to the side with the microdissector. Then the endoscope is removed and the nasal septum is broken directly at the sphenoid floor, pushing the speculum against the septum. This so-called speculum break technique is the second crucial step of the procedure, gaining a wide exposure of the sphenoid floor for an adequate approach of the lesion (Figs. 2B and 3C). After breaking the septum, the endoscope is again inserted and fixed to the endoscope holder. The speculum usually stays directly at the sphenoid floor by itself. The sphenoid ostium is entered with Kerrison rongeurs (Medetz Surgical Instruments, Dallas, Pennsylvania, USA) and the sphenoid floor is removed (Figs. 2C and 3D). With use of a small rongeur, usually a large piece of the sphenoid floor can be preserved for later reconstruction of the floor. Septi in the sphenoid cavity are removed with nasal forceps. If the sphenoid mucosa is very prominent, it has to be removed. Mostly, the mucosa only has to be pushed aside after mobilization with a microdissector. Then the sellar floor—often already infiltrated and broken by tumor tissue—can be localized (Figs. 2C and 3E). The sphenoethmoid planum is localized above the sellar floor, the clivus is localized below it, and the bony prominences of the intercavernous carotid arteries and the optic nerves are localized lateral to it. In most cases of macroadenomas, the sellar floor can be opened with the dissector and the opening enlarged with the rongeur. If the sellar floor is very thick, a high-speed drill or a punch is employed. In any case, the exposure of the lesion should be large enough since in our experience the third crucial step for surgical radicality is adequate tumor exposure. After adequate exposure is achieved, the dura is incised in a cruciate fashion. With various curettes, suction, and grasping forceps, the lesion is then removed in a piecemeal fashion (Figs. 2D and 3F). If the sellar diaphragm does not descend in tumors with suprasellar extension, a Valsalva maneuver might help to bring residual tumor tissue and the diaphragm down into sight (Fig. 3G). At the end of the procedure, the 0-degree optics are removed and the 30-degree and/or 45-degree optics are inserted (Fig. 3H). Particularly with the 45-degree optics, the lateral borders of the sella can easily be visualized and surgical radicality can be achieved. If an angled view to approach the lesion is required earlier, we prefer the 30-degree optics since, under which the lesion is easier to manipulate. This final inspection with the angled optics is the most crucial step, in our experience, to achieving radical tumor removal. In 35 of the last 139 cases, tumor remnants were identified with the angled optics at final inspection. After tumor removal, if the diaphragm is thin or a CSF leak occurred, closure of the sella was performed with an autologous periumbilical fat graft and fibrin glue. In cases with undamaged stable diaphragm, the sella was simply filled with fibrillar hemostypticum (Tabotamp Fibrillar, Surgicel Fibrillar; Ethicon, Somerville, New Jersey, USA). The sellar floor is reconstructed with bone pieces and, if indicated, the sphenoid cavity is filled with an additional fat/Gelfoam graft (Pfizer, New York, New York, USA) and the sphenoid floor is also reconstructed with bone pieces (Fig. 3I). The nasal septum is pushed back in its normal midline position by the small finger (in small noses, a dissector is used), inserted deeply into the other nostril. The nasal mucosa is put back over the sphenoid opening. The speculum is removed and a final inspection is performed with the 0-degree optics in a freehand technique (Fig. 3J). Usually, nasal packing is only required if an adequate hemostasis is not possible elsewhere. With this technique, fracture of the middle turbinate could be avoided in all cases. Only minimal damage, if any, occurred to the nasal mucosa. Mean surgical time was 111 minutes (range 57 to 220 minutes).
Figure 3.
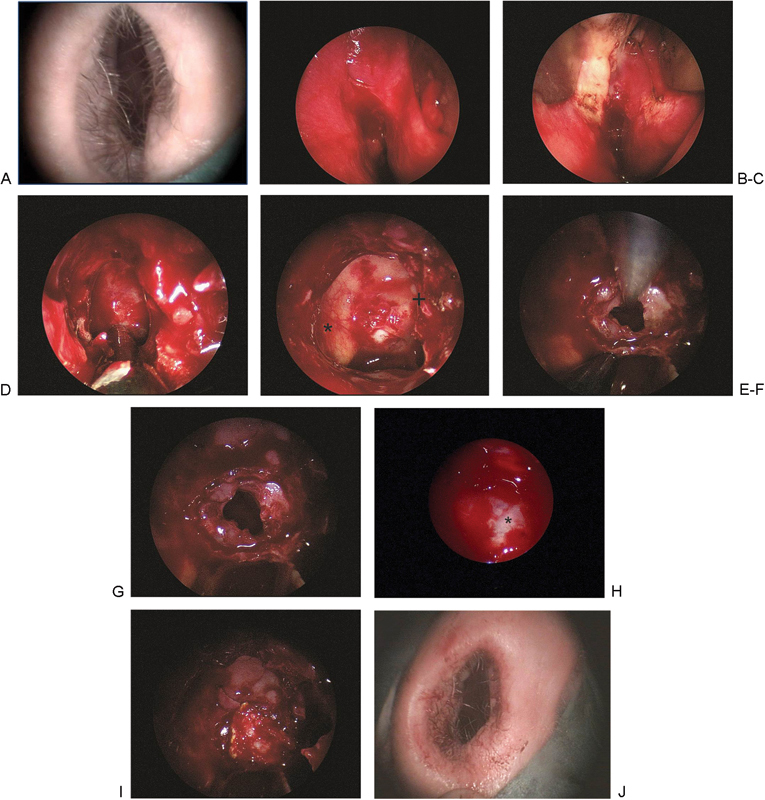
(A) Nasal inspection at the beginning of the procedure. (B) Localization of the sphenoid ostium at the recessus spheno-ethmoideus. (C) View at the floor of the sphenoid cavity after breaking the septum. (D) Removal of the sphenoid floor with preservation of a large bone flap. (E) View at the sphenoid cavity with a septum at the right (+), the carotid channel (*) at the left and the floor of the sella. (F) Tumor removal under endoscopic view. (G) Final endoscopic inspection. In the depth the diaphragm. (H) Inspection of the sellar region with 30 degree optic. At the right the carotid channel (*). No tumor remnants visible. (I) Closure of the sellar with fibrin glue and reconstruction of the sphenoid floor. (J) Postoperatively undamaged nose.
Patient Results
A total of 152 patients received 158 surgical procedures for endocrine inactive macroadenomas and 41 patients underwent surgery for hormone-secreting adenomas (28 growth hormone-secreting lesion, 8 prolactinomas, and 5 microadenomas causing Cushing disease). Among the 193 pituitary adenomas, radical tumor resection was intended at surgery in 175 cases (80%), including 2 microadenomas. In 43 cases, only a simple decompression of the optic chiasm was performed (20%). On follow-up (2 weeks to 2 years; mean 1.04 year), MRI revealed radical tumor resection in 125 of 138 adenoma cases when intended (91%) (Fig. 4A-D). Recurrent tumor growth was observed in five younger patients (2.2%) with adenomas, and subsequent transnasal surgery was performed via an identical approach. No particular scarring was observed in any of these procedures. There was a recurrent endonasal transsphenoidal surgery without any difficulties. In all 11 cases of Rathke cleft cysts, radical cyst excision was intended at surgery. No specific complications were noted. In the three patients with clivus chordomas, primarily a histologic diagnosis was obtained, and a decompression of the tumor was performed. All patients with clivus chordomas went to radiation therapy after surgery. Two patients had a frontolateral CSF fistula after trauma. These fistulas were closed with the aid of neuronavigation and dural substitute. However, after 6 months the CSF fistula recurred in one case and a transcranial revision was performed. In one case an osteolipoma was diagnosed by a neuropathologist. Finally, in one case, a sphenoid mucocele was diagnosed. Because of the patient's request, this mucocele was resected via an endonasal approach. For detailed presentation of our results in comparison to other studies, please refer to Table 1.
Figure 4.
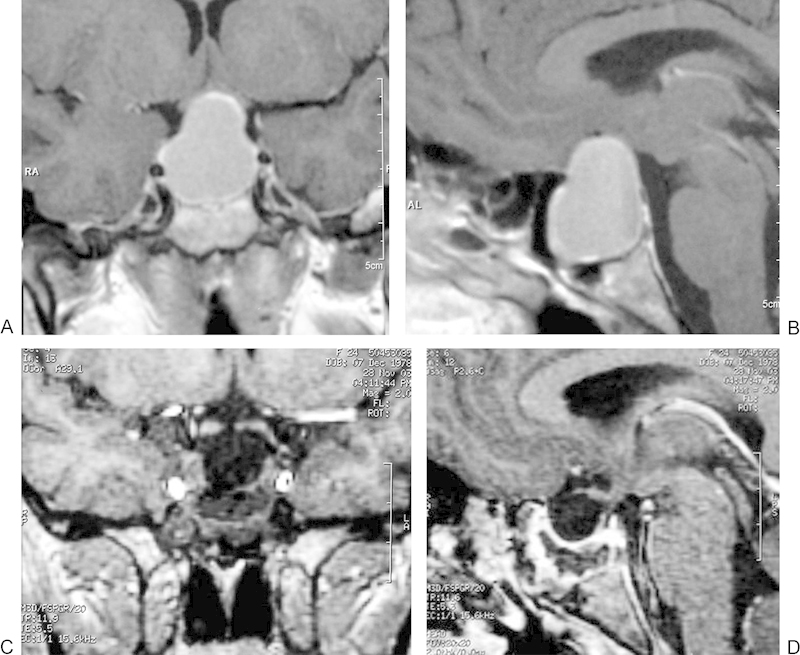
(A) Preoperative magnetic resonance imaging (MRI) of a large intrasellar and suprasellar pituitary adenoma. Coronal slice of a T1 image with gadolinium enhancement. (B) Preoperative MRI of the same tumor in sagittal plane. Sagittal slice of a T1 image with gadolinium enhancement. (C) MRI of the same patient 3 months postoperatively showing complete tumor removal. Coronal slice of a T1 image with gadolinium enhancement. (D) MRI of the same patient and time point in sagittal plane showing complete tumor removal. Sagittal slice of a T1 image with gadolinium enhancement.
Table 1. Surgical Results in Comparison with Other Studies.
| MRI no residual tumor | Zada27 n = 112 |
Jho24 n = 50 |
Cappabianca19 n = 146 |
Our data n = 192 |
|---|---|---|---|---|
| All zero cell adenomas | 70% | 84% | 56% | 88% |
| • noninvasive | 95% | 100% | - | 91% |
| • invasive and giant | 33-40% | 0/3 | - | 0% |
| Prolactinomas | 45% | - | 77% | 89% |
| Cushing adenoma | 60% | 75% | 77% | 50% |
| GH adenoma | 60% | - | 64% | 85% |
| Rathke cleft cyst | 80% | - | - | 83% |
Abbreviation: GH, growth hormone producing adenomas.
Note: Studies with endoscopic technique are marked in gray.
In all patients, hormonal disturbances were the leading symptom in 23 cases (10.8%). Visual deficits were the presenting symptom in 172 cases (79%). The five recurrent tumors were noted on routine follow-up MRI. Preoperative visual deficits improved in 151 of 172 cases (88%); a transient worsening was recorded in one 55-year-old woman (0.5%).
Complications
There was no mortality. No severe or hazardous permanent complications occurred. There were three cases of meningitis (1.4%) and seven cases of CSF leakage (3.2%). Three cases (1.4%) were effectively treated with spinal CSF drainage for 7 days. In one case (0.5%), an endoscopic revision with fat grafting was required. In one case (0.5%), transient worsening of the preoperative visual deficit occurred. In three cases (1.4%), conversion to microsurgery was required for recurrent bleeding from the cavernous sinus. In five cases (2.2%), a reoperation had to be performed for recurrent tumor growth of decompressed macroadenomas. Three patients (1.4%) complained postoperatively of nasal congestion or reduced nasal airflow; however, no complaints were considered to be severe. In one patient a septum perforation was detected by an ENT physician during follow-up examination conducted because of persistent nasal complaints postoperatively. For a detailed account of the complications, please refer to Tables 2 and 3.
Table 2. Complications in Comparison with Other Studies.
| Complications | Zada27 n = 112 |
Jho24 n = 50 |
Cappabianca19 n = 146 |
Our data n = 218 |
|---|---|---|---|---|
| Sellar hematoma | 1% | 0 | 1% | 1 (0.5%) |
| CSF fistula | 3% | 4% | 2% | 7 (3.2%) |
| Meningitis | 2% | 0 | 1% | 3(1.4%) |
| Worsening of visual deficit | 0 | 0 | 1% | 1 (0.5%) |
| Brain infarction | 1% | 0 | 0 | 0 |
| ICA injury | 1% | 0 | 1% | 0 |
| CN VI palsy | 0 | 0 | 1% | 0 |
| Periumbilical hematoma | 0 | 0 | 0 | 2 (1%) |
| Sinusitis | 0 | 0 | 2% | 0 |
| Conversion to microsurgery for bleeding | - | - | - | 3 (1.4%) |
| Reoperation (including 1 CSF fistula revision) | - | - | - | 8 (3.6%) |
Abbreviations: CN, cranial nerve; CSF, cerebrospinal fluid; ICA, internal carotid artery.
Note: Studies with endoscopic technique are marked in gray.
Table 3. Nasal Complications and Complaints.
| Nasal complications and complaints | Literature survey27 | Our data |
|---|---|---|
| Septum perforation | 1-13% | 1 (0.5%) |
| Par-/anesthesia upper lib (sublabial approach) | 5-28% | 0 |
| Anosmia | 5-6% | 0 |
| Nasal complications total | 28-35% | 3 (1.4%) |
| Complaints for nasal tamponade | 39% | - |
| Complaints for tamponade removal | 36% | - |
| Disturbed nasal breathing at 3 months postoperatively | 23% | 5 (2%) |
| Nasal congestion at 3 months postoperatively | 26% | 10 (4.5%) |
Discussion
For almost a century, the search for minimal invasiveness and the avoidance of potential damage to adjacent structures were among the main research topics in neurosurgery.1 Microsurgical transsphenoidal surgery for sellar lesions has been the gold standard for decades2,3,4,5,6,28,29,30,33,34 since Hardy and others modernized and improved the approach making it a safe and sufficient procedure.5 With this standard approach, very good results were obtained with a precise resection of pituitary lesions and low morbidity. However, the various approaches had rather significant differences. Among the various approaches, the sublabial and the transnasal approach has been most widely recommended. Still, at present, surgical strategies for transnasal approaches to the sellar region are diverging. Although some surgeons still consider nasolabial approaches,28,29,30 others use an endonasal microscopic approach,27 and a third group of clinical researchers approach the region via an endonasal route under endoscopic view.14,17,18,19,32,35,36,37 Particularly because of the great progress in intracranial endoscopy since the early 80s,8,9,31,38 the use of the endoscope has become more and more interesting for skull base microneurosurgeons.9,17,18,20,23,25,31,35,37,39,40,41,42,43 However, only recently the endonasal transsphenoidal approach to sellar lesions has become more and more popular.14,20,23,42,44 With a continuous increase in data, at present, the interest in endonasal transsphenoidal approaches to the perisellar skull base is overwhelming.
The increased interest in endoscopy in transsphenoidal surgery has encouraged the attempts of several neurosurgeons to make the transsphenoidal approach more minimally invasive. Many others—particularly Jho and coworkers and Cappabianca and coworkers—have presented a series of studies to further improve the minimally invasive approach of sellar lesions.17,18,19,23,25,43 Jho et al started to perform endoscopic endonasal endoscopic surgery for pituitary adenomas and other perisellar lesions in 1993. These authors presented excellent results, showing that their technique is very effective and less traumatic. Jho employs a one-nostril approach without use of a speculum and without packing of the nose after surgery. They published a series of reports about this technique over the years.23,25,43 Cappabianca (who was trained by Jho) and coworkers use a very similar technique without a speculum through one nostril. They think that the speculum creates a rigid tunnel that limits visibility and maneuvering of the instruments.18 They state that use of the endoscope without the use of the nasal speculum enables a widening of the working angle in all directions and greater angles of view for inspection.18 They also report that the treatment of recurrences after earlier transsphenoidal operation is much easier with the endonasal approach, particularly because of the avoidance of the submucosal nasal phase.18
The authors of this study started with the endonasal transsphenoidal technique in 1997. After several changes in the technique, the presented surgical technique has been applied in all cases of intrasellar or perisellar lesions if a transsphenoidal approach was feasible since October 2000. With the described technique, 218 procedures have been performed through September 2011. In summary, the authors consider their transnasal approach safe and effective. In comparison with other recently published studies, our results with respect to surgical radicality correspond to other data (Table 1). With respect to severe and permanent complications, our results also correspond—or are even superior to—other published series (Table 2). However, the low number of nasal complaints in our study is remarkable in contrast to other results (Table 3). Thus, the authors consider the approach particularly minimally invasive with regard of nasal complications.
Key steps of the approach are the use of a nasal speculum, breaking of the nasal septum just at the floor of the sphenoid sinus, adequate exposure of the lesion, and final inspection for radicality with various optics. Neither Jho and coworkers23,25,43 nor Cappabianca18,19,45 and colleagues use a speculum with their technique. They claim that the speculum might actually contribute to damage of the nasal mucosal and limits the exposure of the lesion. This stands in contrast with our results. In our experience, the in-and-out of the endoscope and other instruments during surgery causes injury to the nasal mucosa without any chance to avoid this if a speculum is not applied. We consider that the instrument is not controlled by the endoscope until it appears in front of the endoscope. With a speculum, the endoscope can be fixed in front of the sphenoid sinus/the sella, often even in the sella, and the instruments can be moved in and out without touching any mucosa. A fixed endoscope image increases precision, and the procedure is faster. In fact, the speculum is the instrument to secure the nasal mucosa, in our opinion. It gives the surgeon good guidance from the nostril deep into the sphenoid cavity. Also, in our 218 procedures, we did not have a case that could not be performed with the speculum because of limited exposure of the lesion. Thus, we advocate the use of a speculum. However, the use of the speculum requires breaking of the nasal septum to gain adequate exposure. This has not led to any complications in our patients so far; also, the surgeons who do not use a speculum induce usually a similar contralateral displacement of the septum after removal of the sphenoid floor together with the attached end of the nasal septum. Thus, because of the perfect guidance of the endoscope and surgical instruments, we prefer the septum breakage with final reposition, which has not shown any morbidity in our patients. In any case, the key step in endoscopy for sellar lesions is the final inspection for radicality with various angled optics. The authors are convinced that this technique, applied with or wothout the speculum, will result in a higher surgical radicality in the near future.
In all, the minimally invasive endonasal transsphenoidal approach allows safe tumor removal under direct visual control. Probably, this will lead to a higher surgical radicality in the long run. However, at present, evidence for a higher radicality with the endoscopic technique cannot be given, though our own data show that in almost 80% of cases, tumor remnants were detected with the angles optics that could not be seen with the straight 0-degree optics. The more radical surgery can avoid recurrences or delay recurrences with the subsequent need for radiation therapy for instance.
The authors are convinced that the combination of this minimally invasive approach with new instruments such as ultrasonic aspirators for endoscopy and other new techniques for tumor aspiration, such as waterjet dissection,21 will further improve the results and establish the endoscopic technique within the next 20 years as the therapy of choice for the approach of sellar lesions via the sphenoid cavity.
Acknowledgments/Disclosure
MR Gaab and MR Oertel are consultants to Karl Storz Company.
References
- 1.Kanter A S, Dumont A S, Asthagiri A R, Oskouian R J, Jane J A Jr, Laws E R Jr. The transsphenoidal approach. A historical perspective. Neurosurg Focus. 2005;18(4):e6. doi: 10.3171/foc.2005.18.4.7. [DOI] [PubMed] [Google Scholar]
- 2.Adams C B, Burke C W. Current modes of treatment of pituitary tumours. Br J Neurosurg. 1993;7(2):123–127. doi: 10.3109/02688699309103468. [DOI] [PubMed] [Google Scholar]
- 3.Ciric I Ragin A Baumgartner C Pierce D Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience Neurosurgery 1997402225–236., discussion 236-237 [DOI] [PubMed] [Google Scholar]
- 4.Fahlbusch R, Honegger J, Paulus W, Huk W, Buchfelder M. Surgical treatment of craniopharyngiomas: experience with 168 patients. J Neurosurg. 1999;90(2):237–250. doi: 10.3171/jns.1999.90.2.0237. [DOI] [PubMed] [Google Scholar]
- 5.Hardy J. Transphenoidal microsurgery of the normal and pathological pituitary. Clin Neurosurg. 1969;16:185–217. doi: 10.1093/neurosurgery/16.cn_suppl_1.185. [DOI] [PubMed] [Google Scholar]
- 6.Laws E J. Philadelphia: WB Saunders; 1995. Transsphenoidal approach to pituitary tumours; pp. 283–292. [Google Scholar]
- 7.Schroeder H W, Oertel J, Gaab M R. Endoscopic aqueductoplasty in the treatment of aqueductal stenosis. Childs Nerv Syst. 2004;20(11-12):821–827. doi: 10.1007/s00381-004-0937-z. [DOI] [PubMed] [Google Scholar]
- 8.Schroeder H W, Oertel J, Gaab M R. Incidence of complications in neuroendoscopic surgery. Childs Nerv Syst. 2004;20(11-12):878–883. doi: 10.1007/s00381-004-0946-y. [DOI] [PubMed] [Google Scholar]
- 9.Schroeder H W, Oertel J, Gaab M R. Endoscope-assisted microsurgical resection of epidermoid tumors of the cerebellopontine angle. J Neurosurg. 2004;101(2):227–232. doi: 10.3171/jns.2004.101.2.0227. [DOI] [PubMed] [Google Scholar]
- 10.Schroeder H W, Oertel J, Gaab M R. Endoscopic treatment of cerebrospinal fluid pathway obstructions. Neurosurgery. 2007;60(2) 01:44–51. doi: 10.1227/01.NEU.0000249242.17805.E3. [DOI] [PubMed] [Google Scholar]
- 11.Oertel J M, Mondorf Y, Baldauf J, Schroeder H W, Gaab M R. Endoscopic third ventriculostomy for obstructive hydrocephalus due to intracranial hemorrhage with intraventricular extension. J Neurosurg. 2009;111(6):1119–1126. doi: 10.3171/2009.4.JNS081149. [DOI] [PubMed] [Google Scholar]
- 12.Mortini P, Roberti F, Kalavakonda C, Nadel A, Sekhar L N. Endoscopic and Microscopic Extended Subfrontal Approach to the Clivus: A Comparative Anatomical Study. Skull Base. 2003;13(3):139–147. doi: 10.1055/s-2004-43324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fischer G Stadie A Reisch R et al. The keyhole concept in aneurysm surgery: results of the past 20 years Neurosurgery 201168(1, Suppl Operative):45–51., discussion 51 [DOI] [PubMed] [Google Scholar]
- 14.Cappabianca P, Cavallo L M, Esposito F, De Divitiis O, Messina A, De Divitiis E. Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery. Adv Tech Stand Neurosurg. 2008;33:151–199. doi: 10.1007/978-3-211-72283-1_4. [DOI] [PubMed] [Google Scholar]
- 15.Zada G, Cappabianca P. Raising the bar in transsphenoidal pituitary surgery. World Neurosurg. 2010;74(4-5):452–454. doi: 10.1016/j.wneu.2010.09.028. [DOI] [PubMed] [Google Scholar]
- 16.Naftel R P, Reed G T, Kulkarni A V, Wellons J C. Evaluating the Children's Hospital of Alabama endoscopic third ventriculostomy experience using the Endoscopic Third Ventriculostomy Success Score: an external validation study. J Neurosurg Pediatr. 2011;8(5):494–501. doi: 10.3171/2011.8.PEDS1145. [DOI] [PubMed] [Google Scholar]
- 17.Cappabianca P, Alfieri A, Colao A. et al. Endoscopic endonasal transsphenoidal surgery in recurrent and residual pituitary adenomas: technical note. Minim Invasive Neurosurg. 2000;43(1):38–43. doi: 10.1055/s-2000-8814. [DOI] [PubMed] [Google Scholar]
- 18.Cappabianca P, Cavallo L M, Colao A. et al. Endoscopic endonasal transsphenoidal approach: outcome analysis of 100 consecutive procedures. Minim Invasive Neurosurg. 2002;45(4):193–200. doi: 10.1055/s-2002-36197. [DOI] [PubMed] [Google Scholar]
- 19.Cappabianca P, Cavallo L M, Colao A, de Divitiis E. Surgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomas. J Neurosurg. 2002;97(2):293–298. doi: 10.3171/jns.2002.97.2.0293. [DOI] [PubMed] [Google Scholar]
- 20.Cappabianca P, Cavallo L M, de Divitiis O, Solari D, Esposito F, Colao A. Endoscopic pituitary surgery. Pituitary. 2008;11(4):385–390. doi: 10.1007/s11102-008-0087-5. [DOI] [PubMed] [Google Scholar]
- 21.Cappabianca P, Cavallo L M, Esposito F, de Divitiis E. Endoscopic endonasal transsphenoidal surgery: procedure, endoscopic equipment and instrumentation. Childs Nerv Syst. 2004;20(11-12):796–801. doi: 10.1007/s00381-004-0933-3. [DOI] [PubMed] [Google Scholar]
- 22.Conrad J, Philipps M, Oertel J. High-definition imaging in endoscopic transsphenoidal pituitary surgery. Am J Rhinol Allergy. 2011;25(1):e13–e17. doi: 10.2500/ajra.2010.25.3542. [DOI] [PubMed] [Google Scholar]
- 23.Jho H D. Endoscopic transsphenoidal surgery. J Neurooncol. 2001;54(2):187–195. doi: 10.1023/a:1012969719503. [DOI] [PubMed] [Google Scholar]
- 24.Jho H D, Carrau R L. Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg. 1997;87(1):44–51. doi: 10.3171/jns.1997.87.1.0044. [DOI] [PubMed] [Google Scholar]
- 25.Jho H D, Alfieri A. Endoscopic endonasal pituitary surgery: evolution of surgical technique and equipment in 150 operations. Minim Invasive Neurosurg. 2001;44(1):1–12. doi: 10.1055/s-2001-13590. [DOI] [PubMed] [Google Scholar]
- 26.Spencer W R, Levine J M, Couldwell W T, Brown-Wagner M, Moscatello A. Approaches to the sellar and parasellar region: a retrospective comparison of the endonasal-transsphenoidal and sublabial-transsphenoidal approaches. Otolaryngol Head Neck Surg. 2000;122(3):367–369. doi: 10.1016/S0194-5998(00)70050-7. [DOI] [PubMed] [Google Scholar]
- 27.Zada G, Kelly D F, Cohan P, Wang C, Swerdloff R. Endonasal transsphenoidal approach for pituitary adenomas and other sellar lesions: an assessment of efficacy, safety, and patient impressions. J Neurosurg. 2003;98(2):350–358. doi: 10.3171/jns.2003.98.2.0350. [DOI] [PubMed] [Google Scholar]
- 28.Sheehan M T, Atkinson J L, Kasperbauer J L, Erickson B J, Nippoldt T B. Preliminary comparison of the endoscopic transnasal vs the sublabial transseptal approach for clinically nonfunctioning pituitary macroadenomas. Mayo Clin Proc. 1999;74(7):661–670. doi: 10.4065/74.7.661. [DOI] [PubMed] [Google Scholar]
- 29.Sharma K, Tyagi I, Banerjee D, Chhabra D K, Kaur A, Taneja H K. Rhinological complications of sublabial transseptal transsphenoidal surgery for sellar and suprasellar lesions: prevention and management. Neurosurg Rev. 1996;19(3):163–167. doi: 10.1007/BF00512046. [DOI] [PubMed] [Google Scholar]
- 30.Shou X F Li S Q Wang Y F Zhao Y Jia P F Zhou L F Treatment of pituitary adenomas with a transsphenoidal approach Neurosurgery 2005562249–256., discussion 249-256 [DOI] [PubMed] [Google Scholar]
- 31.Cappabianca P de Divitiis E Endoscopy and transsphenoidal surgery Neurosurgery 20045451043–1048., 1048-1050 [DOI] [PubMed] [Google Scholar]
- 32.Oertel J GM Endoscopic endonasal transsphenoidal approach for pituitary lesions: results after 77 procedures with special reference to geriatric patients In, Klug N(ed) 2004:Abstract 55 [Google Scholar]
- 33.Fahlbusch R, Ganslandt O, Buchfelder M, Schott W, Nimsky C. Intraoperative magnetic resonance imaging during transsphenoidal surgery. J Neurosurg. 2001;95(3):381–390. doi: 10.3171/jns.2001.95.3.0381. [DOI] [PubMed] [Google Scholar]
- 34.Thomale U W Stover J F Unterberg A W The use of neuronavigation in transnasal transsphenoidal pituitary surgery Zentralbl Neurochir 2005663126–132., discussion 132 [DOI] [PubMed] [Google Scholar]
- 35.Cappabianca P Cavallo L M Esposito F Valente V De Divitiis E Sellar repair in endoscopic endonasal transsphenoidal surgery: results of 170 cases Neurosurgery 20025161365–1371., discussion 1371-1372 [PubMed] [Google Scholar]
- 36.Cavallo L M de Divitiis O Aydin S et al. Extended endoscopic endonasal transsphenoidal approach to the suprasellar area: anatomic considerations—part 1 Neurosurgery 200761(3, Suppl):24–33., discussion 33-34 [DOI] [PubMed] [Google Scholar]
- 37.Nasseri S S, Kasperbauer J L, Strome S E, McCaffrey T V, Atkinson J L, Meyer F B. Endoscopic transnasal pituitary surgery: report on 180 cases. Am J Rhinol. 2001;15(4):281–287. [PubMed] [Google Scholar]
- 38.Cappabianca P, Decq P, Schroeder H W. Future of endoscopy in neurosurgery. Surg Neurol. 2007;67(5):496–498. doi: 10.1016/j.surneu.2006.09.039. [DOI] [PubMed] [Google Scholar]
- 39.Cavallo L M Cappabianca P Galzio R Iaconetta G de Divitiis E Tschabitscher M Endoscopic transnasal approach to the cavernous sinus versus transcranial route: anatomic study Neurosurgery 200556(2, Suppl):379–389., discussion 379-389 [DOI] [PubMed] [Google Scholar]
- 40.Cavallo L M, Dal Fabbro M, Jalalod'din H. et al. Endoscopic endonasal transsphenoidal surgery. Before scrubbing in: tips and tricks. Surg Neurol. 2007;67(4):342–347. doi: 10.1016/j.surneu.2006.09.040. [DOI] [PubMed] [Google Scholar]
- 41.Cavallo L M, de Divitiis O, Aydin S. et al. Extended endoscopic endonasal transsphenoidal approach to the suprasellar area: anatomic considerations—part 1. Neurosurgery. 2008;62(6) 03:1202–1212. doi: 10.1227/01.neu.0000333786.98596.33. [DOI] [PubMed] [Google Scholar]
- 42.Das K, Spencer W, Nwagwu C I. et al. Approaches to the sellar and parasellar region: anatomic comparison of endonasal-transsphenoidal, sublabial-transsphenoidal, and transethmoidal approaches. Neurol Res. 2001;23(1):51–54. doi: 10.1179/016164101101198280. [DOI] [PubMed] [Google Scholar]
- 43.Jho H D. Endoscopic pituitary surgery. Pituitary. 1999;2(2):139–154. doi: 10.1023/a:1009991631761. [DOI] [PubMed] [Google Scholar]
- 44.Cappabianca P Cavallo L M Esposito F De Divitiis E Craniopharyngiomas J Neurosurg 200810911–3., reply 3-5 [DOI] [PubMed] [Google Scholar]
- 45.Cappabianca P Cavallo L M de Divitiis E Endoscopic endonasal transsphenoidal surgery Neurosurgery 2004554933–940., discussion 940-941 [DOI] [PubMed] [Google Scholar]