

Abstract
INTRODUCTION
Galeazzi fracture associated with ipsilateral posterior elbow dislocation and radial head fracture is a rare pattern of injury. Few reports exist that describes this injury pattern and its treatment. We describe a case report of simultaneous occurrence of Galeazzi fracture and ipsilateral dislocation of elbow.
PRESENTATION OF CASE
A 58 year-old female presented with Galeazzi fracture and posterior elbow dislocation associated with radial head fracture of left upper extremity. This was managed with closed reduction of the elbow, open reduction and internal fixation of the radial shaft fracture and K-wire stabilisation of the unstable distal radioulnar joint. Prophylactic fasciotomy was performed. At 10 months follow-up, the outcome was favourable with the American shoulder and elbow surgeon score of 92 and the disabilities of the arm, shoulder and hand score of 18.
DISCUSSION
The presumed mechanism of the injury was a forceful axial loading of a hyperpronated forearm and extended elbow. Our literature review shows that this pattern of injury occurs as a result of high energy trauma in young individuals, and successful outcome can be achieved by addressing each component of this complex injury individually.
CONCLUSION
Simultaneous occurrence of elbow dislocation and Galeazzi fracture seems to be the result of extreme axial force and unique position of upper extremity at the time of impact. Individualised approach to each component of this injury can result in favourable outcome.
Keywords: Galeazzi fracture, Elbow joint dislocation, Radial head, Closed
1. Introduction
A Galeazzi fracture is defined as a fracture of the radius associated with dislocation of the distal radioulnar joint (DRUJ).1,2 It occurs in 2.8–6.8% of forearm fractures in adults.1,2 The elbow dislocation rate is 6–13 cases per 100,000 people and accounts 11–28% of all in juries to the elbow.3
Very few cases of the combination of Galeazzi fracture and dislocation of the elbow joint in the same extremity have been reported in English language literature.4–9 The possible patho-mechanics and treatment approach are of interest in this rare injury.4,7,9
We present a case of the combination of Galeazzi fracture and posterolateral elbow dislocation associated with radial head fracture. The clinical and radiological findings, operative management and the outcome are discussed with review of literature.
2. Presentation of case
A 58-year-old female sustained a left elbow and forearm injuries following a fall whilst running. The initial clinical examination revealed deformity of the elbow and forearm. She also had decreased sensation in ulnar nerve distribution with no motor deficits. Initial radiographs showed left Galeazzi fracture (Fig. 1), left elbow postero-lateral dislocation and minimally displaced marginal radial head fracture (Fig. 2).
Fig. 1.

Anteroposterior and lateral radiographs demonstrating Galeazzi fracture. The radius is fractured at the junction of middle and distal third with associated widening of the distal radio-ulna joint.
Fig. 2.
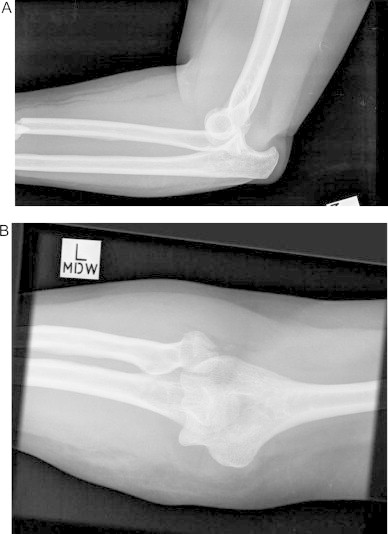
(A and B) Posterolateral dislocation of the elbow associated with mildly displaced radial head fracture.
Immediate manipulation and reduction of the elbow dislocation was performed in emergency department. The patient underwent open reduction internal fixation of the radial shaft fracture the following day using 3.5 mm six-hole locking compression plate (using standard cortical screws) through a standard volar approach of Henry. After internal fixation the stability of the DRUJ and elbow was examined. The stability of the DRUJ was examined under fluoroscopy. Distal radioulnar joint was found to be unstable and pinned using two percutaneous 1.6 mm K-wires in supination (Fig. 3). The elbow joint was stable. A prophylactic volar fasciotomy of forearm was also performed because of significant swelling of flexor compartment of the forearm at the end of procedure. Vacuum dressing was applied to the wound. There were no other clinical signs of compartment syndrome. The fasciotomy wound was primarily closed after two days. The flexor compartment muscles were clinically viable and contractile at the time of closure. The elbow was immobilised in the above elbow plaster slab with the elbow in 90° of flexion for 6 weeks. The K-wires were removed from the DRUJ after 8 weeks. At 10 months, she had no pain or instability of her elbow and wrist. She was able to carry out her normal day-to-day activities. The sensation in ulnar nerve distribution was gradually improving. The range of motion was 0–130° at the elbow, 70° extension and 80° flexion at wrist, 80° of supination and 70° pronation at the forearm (Fig. 4). The disabilities of the arm, shoulder and hand score and the American shoulder and elbow surgeons score were 18 and 92, respectively. Final radiographs demonstrated stable fixation and an enlocated elbow joint (Fig. 5).
Fig. 3.

Postoperative X-ray demonstrating fixation of radius using 6 hole locking compression plate. The DRUJ is enlocated and stabilised using 2 k-wires in supination.
Fig. 4.

Elbow and wrist range of motions at 10 months follow-up.
Fig. 5.

Follow-up X-ray 11 weeks post operatively showing united radial shaft fracture and enlocated elbow and DRUJ.
3. Discussion
Galeazzi fracture combined with dislocation of the elbow is rare.4–9 It has been suggested that this combination occurs when the magnitude of the deforming force is high or the position of the upper limb at the time of impact is unique.4,8 Observation of this injury led us to study the relevant mechanism and compare our findings with the ones reported in the literature.
Forceful axial loading of the hyperpronated forearm is the most probable mechanism of injury associated with Galeazzi fracture1,2; however, some authors believe that loading in supination also can cause Galeazzi injury.1,2 Hence, the fracture is further classified into two subtypes: Type I fracture is characterised by dorsal displacement of the distal fragment of the radius (apex volar) with volar dislocation of the distal ulna and type II fracture by volar displacement of the distal radial fragment (apex dorsal) with dorsal dislocation of the distal ulna. Typically, type I and type II fractures are caused by axial loading of hypersupinated and hyperpronated forearm, respectively.1,2 Posterior dislocation of the ulnohumeral joint can occur with a valgus distracting force and pathologic forced external rotation (posterolateral dislocation) or less commonly a varus distracting force (posteromedial dislocation).5,10,11
The exact mechanism of injury in this case could not be determined from the history. The patient landed heavily on outstretched hand whilst running, and had her arm caught under her body. We believe that our patient sustained a complex injury with similar mechanism described by Sarup and Bryant.9 The extreme axial loading from the impact of outstretched pronated hand with the body weight of patient acting as a driving force resulted in Galeazzi fracture and radial head fracture. Collapse of the radial column would result in transmission of the continuing force through the intact ulna and soft tissue. The transmitted axial force levers the ulna out of trochlear articulation causing dislocation of ulnohumeral joint.3,10
Our review of the English language literature showed only six cases of concomitant elbow dislocation and Galeazzi fracture (Table 1). There were five male and one female patient. The mean age of patients was 27 years old (range 16–32 years). The most common mechanism was road traffic accident (4 cases), suggesting high energy trauma the most likely contributing cause of this injury pattern. However, the mechanism of injury in the presented case is low velocity and the patient age is the eldest among other reported cases with similar injuries. Different variants of this injury are described. Sarup and Bryant reported a case of Galeazzi fracture combined with elbow dislocation and an additional ipsilateral humeral shaft fracture resulting from a fall down a flight of stairs.9 Recently Rajeev et al. reported a case of subacute posterior dislocation of elbow with ipsilateral Galeazzi fracture which was picked up five weeks after open reduction internal fixation of radial shaft fracture.8 Only one previously published case involved radial head fracture.5 In the report by Ng and Rose, the authors believed that posterior elbow subluxation associated with radial head and coronoid fracture (terrible triad variant) was a result of varus postero-medial rotation force. In this case the elbow was unstable intra-operatively requiring surgical stabilisation.5
Table 1.
Literature review of combined Galeazzi fracture and elbow dislocation.
| Author | Year | Case | Mechanism | Injury description | Treatment |
|
|---|---|---|---|---|---|---|
| Elbow dislocation | Galeazzi fracture | |||||
| Rajeev et al.8 | 2011 | 26 Ma | Motor bike accident | Galeazzi fracture and late posterior dislocation of the elbowb | Open reduction and collateral ligament repair | Radial plating |
| Nanno et al.6 | 2011 | 32 M | Motor bike accident | Bilateral Galeazzi fracture and dislocation of the elbow and scaphoid | Closed reduction | Radial plating and tension band wiring of the ulna styloid fracture |
| Ng and Rose5 | 2010 | 27 M | Motor car accident | Galeazzi fracture and posterior subluxation of the elbow associated with radial head and coronoid fracture | Open repair of coronoid and medial collateral ligament | Radial plating and pinning of DRUJ |
| Shiboi et al.4 | 2005 | 34 M | Fall off height (2 m) | Galeazzi fracture and posteromedial dislocation of the elbow | Closed reduction | Radial plating |
| Sarup and Bryant9 | 1997 | 35 F | Fall from flight of stairs | Galeazzi fracture and posteromedial dislocation of the elbow and ipsilateral humeral shaft fracture | Closed reduction | Radial plating |
| Mezzadra et al.7 | 1991 | 16 M | Motor bike accident | Posterolateral elbow dislocation, distal third radius and ulna fracture, dislocated DRUJc | Closed reduction | Radial plating |
M, male; F, female.
Posterior dislocation 5 weeks post operatively.
Not a true Galeazzi fracture.
Treatment options for individuals with combined elbow dislocation and Galeazzi fracture are not altered by their concurrent occurrence.5 In adults, anatomic open reduction internal fixation is the standard treatment for most patients with Galeazzi fracture. Further intraoperative interventions are based on the reducibility and post reduction stability of the DRUJ.1,2 Acute simple elbow dislocations can be treated with closed reduction alone. However, in most cases complex elbow fracture dislocations are best treated with internal fixation and closed reduction of the elbow.11 Our review of the literature shows that in all 6 cases the Galeazzi fracture were treated successfully with open reduction internal fixation. In 2 cases the elbow dislocation were treated surgically due to instability. In one case the dislocation was associated with radial head and coronoid fracture5 and in the other one the elbow dislocation was found after 5 weeks.8 In the latter case the authors acknowledged that the elbow was not examined under anaesthesia following open reduction internal fixation of Galeazzi fracture.8
4. Conclusion
Ipsilateral Galeazzi fracture and elbow dislocation is a rare injury. This pattern of injury is likely the result of significant amount of deforming force and unique position of the upper limb at the time of impact. Each injury could be treated individually regardless of simultaneous occurrence, expecting a favourable outcome.
Conflicts of interest statement
None.
Funding
None.
Ethical approval
Consent was obtained from the patient. The patient's details have been kept anonymous in the manuscript.
Author contributions
Saeed Asadollahi: Removal of K-wires, data collection, writing and drafting the article.
David Shepherd: Performing the surgery, writing and drafting the article, interpreting the findings.
Raphael Hau: Writing and drafting the article, interpreting the findings.
Contributor Information
Saeed Asadollahi, Email: saeedasadollahi@yahoo.com.
David Shepherd, Email: davidwickhamshepherd@gmail.com.
Raphael C. Hau, Email: raphaelhau@hotmail.com.
References
- 1.Atesok K.I., Jupiter J.B., Weiss A.P. Galeazzi fracture. Journal of the American Academy of Orthopaedic Surgeons. 2011;19:623–633. doi: 10.5435/00124635-201110000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Eberl R., Singer G., Schalamon J., Petnehazy T., Hoellwarth M.E. Galeazzi lesions in children and adolescents: treatment and outcome. Clinical Orthopaedics and Related Research. 2008;466:1705–1709. doi: 10.1007/s11999-008-0268-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hobgood E.R., Khan S.O., Field L.D. Acute dislocations of the adult elbow. Hand Clinics. 2008;24:1–7. doi: 10.1016/j.hcl.2007.11.012. [DOI] [PubMed] [Google Scholar]
- 4.Shiboi R., Kobayashi M., Watanabe Y., Matsushita T. Elbow dislocation combined with ipsilateral Galeazzi fracture. Journal of Orthopaedic Science. 2005;10:540–542. doi: 10.1007/s00776-005-0938-0. [DOI] [PubMed] [Google Scholar]
- 5.Ng V.Y., Rose S. Combined elbow fracture-dislocation and Galeazzi fracture in an adult: a case report and review of the literature. Current Orthopaedic Practice. 2010;21:330–333. [Google Scholar]
- 6.Nanno M., Sawaizumi T., Takai S. Case of bilateral Galeazzi fractures associated with dislocation of the right elbow. Journal of Nippon Medical School. 2011;78:384–387. doi: 10.1272/jnms.78.384. [DOI] [PubMed] [Google Scholar]
- 7.Mezzadra A., Gusmeroli E., Tettamanzi M., Prestianni B., Molinari D. A rare injury to the upper limb: elbow dislocation combined with Galeazzi fracture-dislocation. Italian Journal of Orthopaedics and Traumatology. 1991;17:567–572. [PubMed] [Google Scholar]
- 8.Rajeev A., Senevirathna S., Harrison J. Subacute dislocation of the elbow following Galeazzi fracture-dislocation of the radius: a case report. Journal of Medical Case Reports. 2011;5:589. doi: 10.1186/1752-1947-5-589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sarup S., Bryant P.A. Ipsilateral humeral shaft and Galeazzi fractures with a posterolateral dislocation of the elbow: a variant of the “floating dislocated elbow”. Journal of Trauma. 1997;43:349–352. doi: 10.1097/00005373-199708000-00024. [DOI] [PubMed] [Google Scholar]
- 10.Rhyou I.H., Kim Y.S. New mechanism of the posterior elbow dislocation. Knee Surgery, Sports Traumatology, Arthroscopy. 2012;7 doi: 10.1007/s00167-011-1872-7. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 11.O’Driscoll S.W., Jupiter J.B., King G.J., Hotchkiss R.N., Morrey B.F. The unstable elbow. Instructional Course Lectures. 2001;50:89–102. [PubMed] [Google Scholar]