

Abstract
INTRODUCTION
Laparoscopic cholecystectomy is considered to be the gold standard surgical procedure for cholelithiasis and is one of the commonest surgical procedures in the world today. However, in rare cases of previously undiagnosed situs inversus totalis (with dextrocardia), the presentation of the cholecystitis, its diagnosis and the operative procedure can pose problems. We present here one such case and discuss how the diagnosis was made and difficulties encountered during surgery and how they were coped with.
PRESENTATION OF CASE
A 35 year old female presented with left hypochondrium pain and dyspepsia, for 2 years. A diagnosis of cholelithiasis with situs inversus was confirmed after thorough clinical examination, abdominal and chest X-rays and ultrasonography of the abdomen. Laparoscopic cholecystectomy, which is the standard treatment, was performed with numerous modifications in the positioning of the monitor, insufflator, ports and the position of the members of the surgical team and the laparoscopic instruments. The patient had an uneventful recovery.
DISCUSSION
Situs inversus totalis is itself a rare condition and when associated with cholelithiasis poses a challenge in the management of the condition. We must appreciate the necessity of setting up the operating theatre, the positioning of the ports, the surgical team and the instruments.
CONCLUSION
Therefore, it becomes important for the right handed surgeons to modify their techniques and establish a proper hand eye coordination to adapt to the mirror image anatomy of the Calot's triangle in a patient of situs inversus totalis.
Keywords: Laparoscopic cholecystectomy, Dextrocardia, Situs inversus, Calot's triangle
1. Introduction
Situs inversus is a rare autosomal recessive disorder in which the organs are transposed from their normal location to the opposite side of the body. The known human case was reported by Fabricius in 1600.1 When involving both the abdominal and thoracic viscera including dextrocardia it is referred to as situs inversus totalis. When present, it may be associated with several other abnormalities including bronchiectasis, sinusitis, deficient tracheo-bronchial cilia, known as Kartagener's syndrome. In such patients, the clinical diagnosis of cholelithiasis becomes more difficult because the clinical presentation is confusing, especially because of the pain localized to the left hypochondrium.
The mirror image anatomy not only demands greater surgical skill but also requires careful pre-operative planning for setting up the operation theatre, the positioning of the surgical team, the ports and instruments. Difficulties are encountered by the right-handed surgeon who must show care not to cross arms to retract Hartmann's pouch for skeletonization of Calot's triangle.4
We report a case of a 35 year old female with situs inversus totalis with cholelithiasis with history suggestive of chronic cholecystitis managed by laparoscopic cholecystectomy.
2. Case description
A 35 year old female presented with recent intermittent pain in the left hypochondrium occasionally radiating to the back and dyspepsia often associated with episodes of vomiting. She reported similar episodes in the last 2 years relieved on intravenous antacids and analgesics. There was no history of fever, jaundice, altered bladder or bowel habits, abdominal distension or weight loss. She underwent open tubal ligation at the age of 27 years and had an uneventful recovery following that. She had no other ailments or symptoms.
On clinical examination, there was no jaundice or fever. The abdominal examination revealed mild tenderness in the left hypochondrium, a linear scar in the midline in the infra-umbilical region 8 cm below the umbilicus and the rest of the abdominal examination was unremarkable. The apex beat was present in the fifth intercostal space on the right mid clavicular line.
The patient's blood investigations revealed normal complete blood count, liver and kidney function tests, serum electrolytes, blood glucose. An ultrasonography of the abdomen [Fig. 1] was performed which showed the following:
-
1.
Liver and gall bladder on the left side [Fig. 1a], gall bladder lumen filled with multiple subcentimetric calculi with posterior acoustic shadowing.
-
2.
Common Bile Duct diameter 5 mm, portal vein normal.
-
3.
Spleen on the right side [Fig. 1b], Inferior vena cava on the left side and aorta on the right side [Fig. 1c].
Fig. 1.
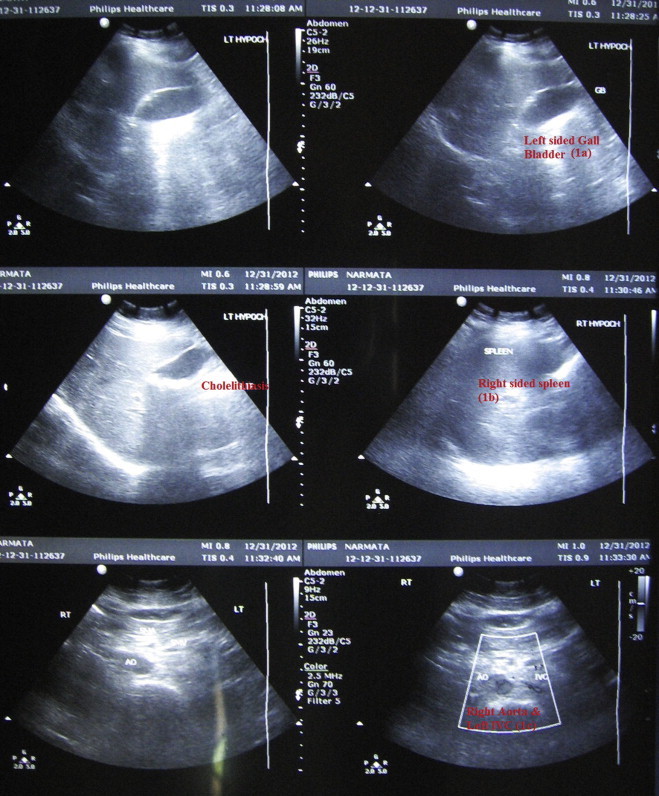
Ultrasonography abdomen-left sided liver & gall bladder (a), right sided spleen (b), left sided IVC and right sided aorta (c).
The chest radiograph of the patient showed heart shadow on the right side (dextrocardia) and the left hemi diaphragm to be raised as compared to the right side [Fig. 2].
Fig. 2.
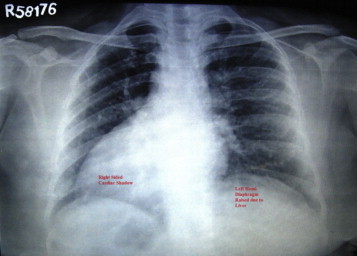
Chest radiograph showing dextrocardia.
The diagnosis of cholelithiasis with situs inversus totalis was established and decision to perform a laparoscopic cholecystectomy was taken after admitting the patient electively.
In order to conduct the surgery, the theatre equipment including the monitor, CO2 insufflator and diathermy were positioned in the mirror image of their normal position on the left side of the patient. The patient was positioned in the reverse Trendelenberg position with the right side slightly inclined up. The difficulty of even creating pneumoperitoneum from the right side by a right handed surgeon was experienced, so it was created comfortably from the left side as is done conventionally as the vision component was not involved. The first 10 mm port was inserted through the infra umbilical incision and confirmation of the diagnosis of situs inversus was done from the left side only [Fig. 3].
Fig. 3.
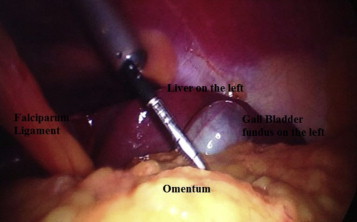
Liver and gall bladder in the left hypochondrium.
Subsequently the position of the surgical team was: the primary surgeon and the first assistant on the right side of the patient and the second assistant on the left side. Another 10 mm port was placed 5 cm below the xiphoid process just to the left of the midline. The other two 5 mm ports were inserted in the usual way but on the left side [Figs. 5 and 6]. A toothed grasper was inserted through the port 4 and was used to retract the fundus of the gall bladder. Being a right handed surgeon, the primary challenge was to retract the Hartmann's pouch while dissecting the Calot's triangle which led to crossing of the hands [Fig. 4].
Fig. 5.
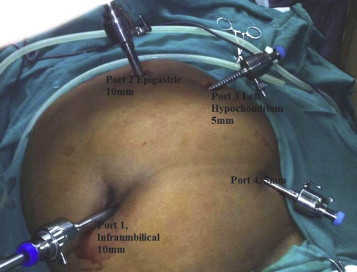
Port positions-mirror image.
Fig. 6.

Post operative sutured port sites.
Fig. 4.
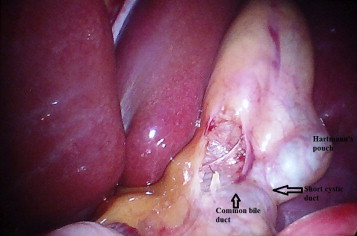
Calot's triangle.
This difficulty was overcome by allowing the first assistant to retract the Hartmann's pouch throughout the surgery while the main surgeon dissected the Calot's triangle using his right hand from the epigastric port with convenience. The cystic duct was noticed to be short and wide. It was dissected separately from the cystic artery and both separately clipped and divided via the epigastric port only. It was again found to be difficult to apply clips as the angle of the clip applicator did not fit along the direction of the cystic artery. The gall bladder was dissected out from the gall bladder fossa using the hook diathermy via the epigastric port with the first assistant maintaining traction on the gall bladder. At the time of retrieval of the gall bladder, the calculi were removed using the ovum forceps and the organ extracted out via the subxiphoid epigastric port.
The duration of the surgery was found to be 95 min which was longer than the conventional laparoscopic cholecystectomy which can be explained by the modification in the ergonomics made to adjust to the mirror image anatomy. The post operative period was uneventful and the patient was discharged the following day.
3. Discussion
Laparoscopic cholecystectomy is a technically difficult procedure in patients of situs inversus but situs inversus is not a contra-indication for the procedure. The incidence of cholelithiasis is same in situs inversus as in the general population.2 The presentation of the disease is, however, different as they can present with left upper quadrant or epigastric pain and in some cases, even right upper quadrant pain.2
It is the adaptation of the position of the surgeon, the assistants, ports for the dissection of the Calot's triangle, the direction of the clip applicator in the line of the cystic duct and artery that are important aspects in a case of situs inversus undergoing laparoscopic cholecystectomy. Most reports in the literature describe the mirror arrangement of the ports and the surgical team and the set up of the operating theatre.1,4,5 Batista et al. described the procedure with 4 ports-right pararectus (10 mm), umbilicus (10 mm), left pararectus (5 mm) and epigastric (5 mm).3 In our case, the epigastric port was used as the working or the dissecting port. Hall et al. used the epigastric port for grasping the gall bladder and the mid clavicular line port on the left side was used as the dissecting port.4
4. Conclusion
Most of the case reports in the literature have recommended laparoscopic cholecystectomy as the standard treatment for cholelithiasis in situs inversus. The procedure can be performed with utmost safety if the difficult orientation of the mirror image anatomy in this area is handled with careful planning both pre-operatively and intra-operatively and if performed by a experienced surgeon.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Informed consent obtained from the patient.
Author contributions
S.V.A. performed the surgery and was involved in the preoperative work up and postoperative care of the patient, helped in the preparation of the write up.
A.D. assisted in the surgery and was involved in the preoperative work up and postoperative care of the patient, conceived the write up.
S.S. assisted in the surgery, involved in the postoperative work up of the patient.
D.S.K. involved in the preoperative workup and postoperative care of the patient, performed the literature search.
A.S. involved in the preoperative workup and postoperative care of the patient.
B.B.T. involved in the radiological investigations and reporting of situs inversus in the patient.
Contributor Information
S.V. Arya, Email: svarya@yahoo.com.
Anupam Das, Email: dr.anupam@rediffmail.com, dranupamdas21@gmail.com.
Sunil Singh, Email: sunilkamal.singh@gmail.com.
Dheer Singh Kalwaniya, Email: dheersurgeon@gmail.com.
References
- 1.Pitiakoudis M., Tsaroucha A.K., Katotomichelakis M., Polychronidis A., Simopoulos C. Laparoscopic cholecystectomy in a patient with situs inversus using ultrasonically activated coagulating scissors. Report of a case and review of the literature. Acta Chirurgica Belgica. 2005;105:114–117. [PubMed] [Google Scholar]
- 2.Palte N.M., Tantia O., Sasmal P.K., Khanna S., Sen B. Laparoscopic cholecystectomy in situs inversus – our experience of 6 cases. Indian Journal of Surgery. 2010;72(5):391–394. doi: 10.1007/s12262-010-0159-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Augusto Ribeiro Batista Felipe, De Moricz Andre, De Campos Tercio, Monteiro Pacheco Adhemar, Jr., Altenfelder Silva Rodrigo. Technical aspects of laparoscopic cholecystectomy in a patient with situs inversus totalis – case report. Brazilian Journal of Video-Surgery. 2011;4(2):114–117. [Google Scholar]
- 4.Hall T.C., Barandiaran J., Perry E.P. Laparoscopic cholecystectomy in situs inversus totalis: is it safe. Annals of the Royal College of Surgeons of England. 2010;92(5):W30–W32. doi: 10.1308/147870810X12699662980277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.McKay D., Blake G. Laparoscopic cholecystectomy in situs inversus totalis: a case report. BMC Surgery. 2005;5:5. doi: 10.1186/1471-2482-5-5. [DOI] [PMC free article] [PubMed] [Google Scholar]