

Abstract
Objective
The initiation of teen driving, which occurs between ages 15 and 17, has generally been studied primarily in relation to crash injury reduction. However, it may be the most important period influencing development between puberty and emerging adulthood because, once the teens are driving on their own or riding with other teens, parental control over social behavior is greatly reduced and opportunities for risk taking are substantially increased. The noncrash risks and benefits of licensing during this critical transition period is the subject of this paper.
Methods
We identify “Transition Teens” as a subgroup of all 15- to 17-year-olds who reside in middle-class suburban and rural areas where families can afford a car and where a vehicle is needed for reasonable mobility. In this paper, we review recent studies on the effect of driving on non-traffic-related behaviors of teen drivers. Our analysis suggests that there are two environments that affect behavior and development: the home environment and the extended environment. Before driving age, the home environment influences are omnipresent in the life of the developing child. However, once teens can move more readily within the community and travel outside the home environment on their own or with a peer, they have access to locations where many or all the local controls on risky behavior may be absent.
Results and Conclusions
This article introduces the concept of “transitional teens” and provides a rough model that explains the possible risks encountered by this group when they begin to drive a vehicle or to ride with a peer. We offer this model to the research community with a challenge to hypothesize, test, and explore this proposed transitional period so that we can better understand and mitigate its associated risks.
Keywords: Traffic safety, teen driving, alcohol and drug use, underage driving laws, teen licensing
INTRODUCTION
Novice Teen Drivers
Learning to drive is a high-risk activity for youth. Traffic crashes are the leading cause of fatalities among teens (Figure 1). Further, crash risk is at a lifetime high during the first 2 years of driving (National Safety Council, 2005). Between 1995 and 2004, crashes involving 15- to 17-year-old drivers claimed the lives of 30,917 people nationwide. Of these, 11,177 were the teen drivers themselves, and 9,847 were passengers of teen drivers (The Auto Channel, 2006). Williams (1999) found that the crash-involvement rate for 16-year-olds was four times that of drivers in their twenties. Research has indicated that four factors play a prominent role in crashes involving teenagers: inexperience, immaturity, risk taking, and greater exposure to risk (Masten and Hagge, 2004; Senserrick and Haworth, 2004). The risk is increased by the failure to fasten safety belts (Womack et al., 1997), nighttime driving (Williams and Preusser, 1997), and distractions created by teen passengers (Farrow, 1987). These threats extend to the passengers of novice drivers who also are less likely buckle up and share the same risks as the driver.
Figure 1.

Leading Cause of Fatalities for Teens (Source: National Highway Traffic Administration 2003 DATA NSC Family Safety & Health, Summer 2004)
Countermeasures
The high-crash rate of youthful novice drivers has been recognized for some time. Initially, the official response to that problem was to require a driver education program for high-school sophomores as a prerequisite for obtaining a driver’s license. Experience demonstrated, however, that universal driver education in the public schools resulted in earlier licensing and increased exposure to crashes for novice drivers, many of whom would not have obtained a license until necessitated by employment or college attendance. Thus, many view driver education as counterproductive; consequently, support for it as a mandatory requirement for licensing has declined (Williams, 1996; Mayhew and Simpson, 2002; Mayhew et al., 1998; Williams and Ferguson, 2004). The response to this problem was to control the exposure of teenage novice drivers rather than depending on driver education programs (Williams, 1999). Most states have recently enacted graduated driver licensing (GDL) laws that require the novice driver to gain a year or more of experience before receiving a regular license. These laws vary substantially across the 50 states but generally contain four features: delay in application for licensing until age 16; an extended period of 3 to 6 months of driving on a learner’s permit with an adult in the car; an intermediate stage of solo driving during which teen passengers and nighttime driving (generally after midnight) is not permitted; and finally, strict observance of zero-tolerance (ZT) laws and safety belt laws is required with offenses sanctioned by extended delays in granting a full license (National Highway Traffic Safety Administration, 2006). Research has demonstrated the traffic injury benefits of GDL programs (Foss et al., 2001; Foss and Goodwin, 2003; Shope et al., 2001b; Shope and Molnar, 2004; Williams and Preusser, 1997; Chen et al., 2006) Research on graduated licensing, however, has revealed that it has the potentially negative feature of reducing the number of youths licensed to drive (McKnight et al., 1983; Frith and Perkins, 1992; Ferguson et al., 1996) and, therefore, their ability to meet their and their family’s transportation needs.
Benefits and Risks of Teen Licensing
The control of driving exposure raises a neglected issue regarding the benefits and potential risks of teen licensing related to nontraffic features of the teen lifestyle related to the availability of a vehicle. It is clear that families can benefit from teenage drivers who can transport themselves to jobs and school activities and run errands. The economic value of such activities by drivers in the 16- to 17-year age group has not been estimated, but it is clearly of substantial value to families and their teenagers. Similarly, the potential for the availability of a vehicle to increase the risk of undesirable behavior (such as alcohol and drug use, risky sexual behavior, or involvement in violence) has not been assessed. The age (15–17) when a teen begins to drive or travels in a vehicle driven by a peer initiates a period of increased opportunity for participation in adult activities. This also affords the opportunity to travel to an environment that is lacking in adult supervision. Before this age, parents controlled travel decisions and the vehicle-dependent activities of the teenager. Later, when a teen is licensed to drive, a substantial amount of control over personal activities passes to them. Positively, this provides an important opportunity for growth in maturity that will be required when the individual leaves home 2 to 3 years later. Negatively, it also exposes the teenager to two significant additional health-risks from increased access to alcohol and other drugs (AODs), sexual risk taking, and violence associated with high-risk environments and lack of parental supervision.
Effect of Driving on Noncrash Risks
To date, research on teen driving has focused on crash injury reduction. Although considerable attention has been given to the risks associated with highway crashes that result from youthful inexperience and risk taking, little attention has been given to the effect of being able to drive on the quality of life and on the nontraffic health risks of the teenager. Aside from traffic safety studies of such factors as driving skill, risk taking, training, and licensing, several developmental studies relating attitudes and behaviors, including alcohol and drug use, to teen crash involvement have been conducted (Bingham and Shope, 2004a; Bingham and Shope, 2004b; Bingham and Shope, 2004a, Shope et al., 2001a; Shope and Bingham, 2002). Less studied is the effect of access to a vehicle on the lifestyle and problem behavior of the teen.
Review of Studies of Noncrash Risks and Benefits
In our review of teen-driving studies, we found only a few reports relevant to the effect that the availability of a vehicle has on the lifestyle of young teens. The most directly relevant study was by McCarthy and Brown (2004). They collected responses to a questionnaire on alcohol and other drug consumption and driver licensing from a panel of high school students in San Diego in the fall of 2001 and again in the spring of 2002. They compared reported drinking behaviors of unlicensed students, newly licensed students, and longer term licensed students. They also studied the change between initial unlicensed and later licensed status. They found that obtaining a driver’s license was associated over the longer term with increases in the frequency of alcohol, cigarette, and marijuana use. The immediate effect of licensing on new drivers appeared to be associated with more negative attitudes toward drinking and driving and reduced alcohol consumption; however, reported instances of drinking-and-driving behavior increased with driving experience. The authors interpreted their results as indicating that teen drivers have more opportunities for substance use and decreased parental monitoring. They noted a not surprising tendency for teens to be less likely to ride with a drinking driver after obtaining a license.
Preusser et al. (2000) conducted a study in four states with varying laws that produced differing teen licensing rates. They surveyed high school students to obtain reports on their driving and their activities in Delaware, Connecticut, and New York, where learner’s permits and full licenses could be obtained before age 17, and in New Jersey, which at the time was the only state in the union that did not license teens before age 17. Their comparison of data from New Jersey with data from the other three states confirmed that there were large differences in the percentage of licensed high school sophomores and juniors and in the amount of their driving (by the senior year, the license status and driving was similar in all four states). The effect of these differences in driving on teen activities was somewhat less than might be expected. Students in New Jersey were less involved in doing family errands but were not significantly different in their weekday activities, such as holding a job, being involved in sports, or visiting friends. There were, however, some differences in weekend activities, such as going out on dates, but surprisingly, no differences in going to parties, participating in school clubs, and going shopping.
The Preusser et al. (2000) study clearly demonstrated that the teens in states with delayed licensing had to rely more on parents to provide transportation. They suggested that this “may have promoted additional opportunities for interaction between parents and teens and additional opportunities for parents to monitor the comings and goings of their adolescent children … thus, it is possible that crash reduction may not be the only benefit from delayed teenage licensure” (p.237). The lack of a strong effect of delayed licensure on the activities of teens may at first suggest that the role of the automobile in the transition-teens concept is not as central as suggested by the model we propose; however, the Preusser et al. study did not consider AOD use or other behavioral problems and did not relate individual driving status to teen problems. The authors did cite the study of teen vehicle ownership (Williams et al., 1987), which found that teen vehicle ownership was associated with lower academic performance. Thus, the Preusser et al. (2000) study paves the way for more intensive analysis of the role of driving and access to vehicles in the maturation and risk behavior of 15- to 17-year-olds.
Beck et al. (Beck et al., 2005) reported that disagreement on driving rules between parents and their teen resulted in, aside from more risky driving, travel to more “dangerous places.” One study (Poulin et al., 2007) that raised a potential downside to policies limiting teen licensing was a survey of high school students in the Canadian Maritime Provinces. Poulin et al. found that once such factors as social economic class and educational attainment were controlled, a lower licensure rate was associated with a higher rate of riding with an impaired driver.
Two economic analyses conducted by Carpenter (2004 and 2005) provide indirect evidence of the potential significance of teen driving to alcohol consumption and risky behavior. In his 2004 study, he examined the effect of the ZT law, which makes it an offense for anyone younger than age 20 to have any alcohol in his or her body while driving, on heavy episodic (binge) drinking by 18- to 20-year-olds (experimental group) compared to 22- to 24-year-olds (comparison group) using information on alcohol consumption from the Behavioral Risk Factor Surveillance System (BRFSS) from 1984 to 2001. He concluded that the presence of a ZT law reduced binge drinking by the underage group by 13 to 20%. Moreover, he bolstered this result by demonstrating that ZT laws reduced per capita beer sales by 15- to 19-year-olds and the proportion of public drunkenness arrest accounted for by youths aged 18 to 20. In 2005, Carpenter conducted a second panel study relating state ZT laws to state gonorrhea rates. He compared males and females separately in two age groups: 15 to19 years of age (affected group) and 20 to 24 years of age (control group). He controlled for the major impaired-driving laws, social economic factors, and ethnicity. He found that gonorrhea rates for 15- through 19-year-old White- non-Hispanic males were significantly lower (by 14%) in states with ZT laws, while the rates for 20- to 24-year-olds were not significantly lower. He interpreted the results of the two studies as indicating that ZT laws affect gonorrhea by reducing heavy drinking among the affected youth. Studies in which driving or driving laws are the independent variable and alcohol drug use or other problem behavior is the outcome measure are rare. Much more interest has been shown in the use of impaired driving or crash involvement as an outcome measure to study the significance of various characteristics of teen AOD users.
For the 15- to 17-year-olds, the transition from being transported by parents to driving or riding with a peer has the potential for modifying three important factors that have been shown to be important in determining alcohol and drug use: parental influence, peer influence, and the environment (availability). Teen driving or riding with a peer may transport the youth to an environment where parental influence is weakened, peer influence is strengthened, and alcohol and drug availability is increased. With these features, the “Transition Teen” period is analogous to the “Emerging Adult” transition period, which is initiated 2 years later with the transition to independent living. Kyprie et al. (2004) examined the transition to independent living by New Zealand youths that occurred at an average age of 17.7. They followed the substance use patterns of the teen sample for up to 6 years and compared drinking and drug use in the pre-transition with the post-transition period. They reported that regular drinkers who consumed 2.3 drinks per week in the period prior to the transition increased to 10.1 following the transition (p<.01). Both the exposure to an environment where alcohol was more available and peer alcohol use were found to be significant factors in the increase in post-transition drinking. Although the transition to independent living is clearly a more substantial transition than the transition to driving or riding with peers, the latter clearly contains some of the same factors inherent in independent living.
How Significant is Driving Status to Teens?
A report on a National Young Driver Survey of 5,665 16- to 19-year-olds by The Children’s Hospital of Philadelphia (The Center for Injury Research and Prevention at The Children’s Hospital of Philadelphia and State Farm Mutual Automobile Insurance Company, 2007) noted that “to teens, driving is considered an essential coming of age experience, and it has become an established aspect of teens’ maturation and socialization process.” The authors noted that while half of that age group drive to school and more than three-fourths use a car for errands, 60% say they drive to relax and 50% report driving without a destination in mind, suggesting substantial unsupervised recreational driving. And driving is a significant aspect to teens’ lives. McCarthy and Brown (2004) suggested “the acquisition of a driver’s license is one of several important developmental transitions for youth (p.289).” Yet, the implications of this transition have not been fully investigated. In a recent publication presenting the development sources of crash risk for young drivers, Arnett et al. (2002) argued that “the difference between 16–17 year olds and 18–19 year olds is so stark that they should be considered to be in two separate periods of life…” Yet, Arnett further continued, most driving patterns or trends are reported in one age category, 16 to 20 years. Teen driving, which occurs between ages 15 and 17, may be the most important developmental period between puberty and emerging adulthood. In a recent publication focused on the theory and science of emerging adulthood, Tanner (2006, p. 49) noted: “Prior to emerging adulthood, the individual is dependent on and regulated by parents, teachers, and the laws of society. During emerging adulthood, the individual accrues experience and prepares for self-governance with variable amounts of support still available from parents (i.e., financial gifts) and institutions (i.e., college).” The 15- to 17-year-old period, just prior to emerging adulthood, is where the developing person first experiences a reduction in parental control over social behavior and where the experiences and opportunities for risk taking are greatly increased. This critical transition period is the subject of this paper.
“Transition Teens” Concept
The studies and observations cited herein suggest that it may be useful to consider the period in which driving or riding with a teen becomes an important possible “stage” in adolescent development, at least for those teens living in the suburbs for whom access to a vehicle provides a broader horizon of activities than those without access to a car. Teens in central city areas would be expected to be less influenced by access to a vehicle because they have access to public transportation and a vehicle may have less economic value and involve greater expense to park and maintain. Although inner cities often have more unsafe neighborhoods than the suburbs, when a teenager living in the suburbs begins to drive, inner city hazards may become accessible. School and community events or parties in the local neighborhood benefit from formal and informal supervision by parents and other adults who can discourage AOD use, sexual risk taking, and violence. Driving a vehicle allows the teen to travel to locales where these adult influences may not be present.
The risks associated with the expanded horizons for transition teens (Figure 3) include riding with peers who are novice drivers, exposure to opportunities for AOD use, and peer support, if not pressure, for heavy consumption. Travel may transport teens into areas of greater traffic and crime risk, and the absence of supervision in the vehicle may expose transition teens to sexual risk taking. The principal responses to these risks have been high school education programs and statewide environmental efforts to promote the responsible service and sales of alcohol and the suppression of drug sales. Because of the influence of parents over the availability and the use of a vehicle by the teen driver (Hartos et al., 2004; Beck et al., 2005, 2006; Simons-Morton et al., 2004), programs that alert them to the risks beyond those of the highway would seem to be promising. It is at this point that the traditional highway safety field joins the wider field of public health in producing a common area for community prevention programs. Although parents support graduated licensing despite the potential inconvenience of having to drive their teens to many of their activities (Williams et al., 1998), not surprisingly their teens do not support the limits imposed on their driving by graduated licensing (Williams et al., 1984).
Figure 3.

Environmental Model for Transitional Teen Behavior
Whether the identification of a period such as “Transition Teens” covering the years from 15 to 17 when adolescents have the opportunity to begin driving or riding with peers is a development “stage” deserves further study. It does appear to have many features similar to those described in the “Emerging Adulthood” stage. Further, the utility of defining it a “stage” also depends on the extent that members of the same age group share common traits and are affected by similar environments. Developmental phases are traditionally associated with obvious physical changes in the body, such as puberty, or have been based on grade levels, in part because such definitions are relatively clear and precise. However, environment plays an important role in determining growth opportunities and health risks in all developmental phases. Over-reliance on formal definitions based on physical growth or academic stratifications may obscure important transitions that occur within a traditional developmental phase. Being the driver or the passenger in a vehicle driven by a teenager is an example of an environmental transition that has a potentially significant effect on teenage development
Application of Theory to Transition Teen Behavior
Researchers interested in alcohol as a factor in traffic safety have benefited from the availability of a relatively strong, broadly available and objective measure of problem behavior, like crash involvement. This measure has stimulated the implementation in all 50 states of three laws that potentially can strongly effect underage drinking: first, the minimum legal drinking age (MLDA) law; second, the ZT law, which makes it an offense for individuals younger than age 20 to operate a vehicle with any amount of alcohol in their bodies; and third, GDL laws, many of which limit nighttime diving and therefore potentially reduce drinking. This has tended to bring the developmental and traffic safety fields together. However, although developmental researchers most often use traffic safety statistics as outcome measures, most of the research in the two field areas is pursuing separate pathways. In this paper, we attempt to develop a model that integrates the research from both fields.
It should be noted that some research in traffic safety already encompasses elements from the developmental field. Shope and Bingham (2002) have presented a model for the study of teen crash involvement (Figure 2) that includes physical, psychosocial, and behavioral developmental factors. Typical of traffic safety studies, their model focuses on driving behavior with an important public health objective—crash injury reduction—as the outcome measure. But as our review suggests, driving has an important independent role in relation to other public health concerns including AOD use, sexual risk taking, and violence, which are of special interest to developmental researchers. Despite the potential importance of the mobility and privacy provided by a vehicle, its influence is rarely studied as a factor in those public health concerns. It is our objective in this paper to suggest a framework for integrating traffic safety and developmental science at the point at which the vehicle first becomes available to teenagers and may have the most profound effect on adolescent development.
Figure 2.

Model of Novice Crash Risk (Source: Shope and Bingham, 2002)
Model for Transition Teen Behavior
Towards this aim, we propose the conceptual model shown in Figure 3. It focuses on the 15- to 17-year-old age group, a period encompassing the first 3 years of high school and the point at which teenagers first become eligible to drive. The model suggests that there are four key elements that bear on the health risks of the youths in this age group: the developmental status of the individual, and three external factors; parental influence, social/environmental influences, and peer influences. The model contrasts the status of those influences before, compared to, and after the teen achieves the mobility that comes from driving or riding with peers. Before that point, the individual is limited to what we label as the “home environment” with relatively strong parental and other adult influences. Gaining the ability to drive grants the teen the option of entering the “extended environment” that lies outside the home community where adult and normative influences may be substantially weaker.
Home Environment
As in Shope and Bingham’s (2002) model, we identify three elements that significantly affect transition teen behavior: the community and its norms, parental (and significant other adult) influences, and peer influences. These three elements can become either risk or protective factors in influencing adolescent’s decisions to engage in risk behaviors. Bridging the extended environment, where additional risk behaviors exist, is the transition teen’s access to a vehicle.
Community
The community (schools, law enforcement, local ordinances) includes protective factors, such as those related to the regulation of alcohol and structured teen activities (school and after-school athletics and cultural programs). Although risk factors such as the availability of alcohol and drugs, crime, and traffic risks may be present within the home environment, the community is generally thought to be protective. However, the sensitivity of the interaction between community policies and driving risk was illustrated by Stone and Runyan (2005). They studied crashes involving 16- to 18-year-old high school students during lunch periods (12 PM to 2 PM) in counties that allowed students to drive off school grounds for lunch in comparison to counties where this was not allowed. The relative risk of crash involvement was three times higher during the lunch period where students could drive to lunch.
Ecological studies (LaScala et al., 2005) suggest that the community exercises an important influence on adolescent drug use through formal controls, such as economic conditions and law enforcement. For example, MLDA laws and ZT laws have been shown to effectively reduce underage alcohol-related traffic deaths (Grube and Nygaard, 2005; Shults et al., 2001; Voas et al., 2003). Statewide laws affect all communities; however, their influence on any specific locality is dependent on the level of enforcement (Ferguson et al., 2000). Similarly, local ordinances or zoning requirements can limit the number of alcohol outlets and the hours and conditions of sale in communities that establish such policies. Thus, formal controls vary considerably across communities but are more likely to be protective in the suburbs. Here, funding for enforcement is relatively available and citizens’ groups can have a substantial effect on zoning and other civic decision making.
Parents and Significant Adult Influences
Equally or more significant in minimizing substance abuse and risky behavior is the influence of parents and/significant adults—such as teachers, coaches, and neighbors—who enforce community norms. Parents, with whom transition teens live, are obviously in the best position to monitor their teen’s activities. However, teachers, coaches, and neighbors can exercise considerable formal and informal control within their specific contexts, limiting teen risk-taking behavior.
Peers
Social identity theory emphasizes the influence of the perceived group behavior on individual norms. Among teens, however, the expression of group behavior is generally limited by the restricted opportunities available in the neighborhood environments and the limits imposed by adult supervision. Intimate groups of teens who share risk-taking interests tend to seek environments where such activities can be pursued. Such efforts are generally frustrated as long as the teen is dependent on the adult for transportation away from the home environment. When peer transport is available, however, small affinity groups of teens can move to locations where high-risk activities are more possible (i.e., there is less supervision). In such extended environments, the behavior of the small reference group is relatively unrestrained, and individual group members may be influenced to join in group activities that they have not previously engaged in because of the limited opportunities in the home community.
Behavior in any context is hypothesized to be dependent on the perceived behavior of groups with which the individual feels closely associated. Although there are undoubtedly enduring underlying reference groups, the specific reference group may vary with the context. Specific behavior is further limited by the groups’ perception (and therefore the individual’s perception) of their ability to act within the context (perceived behavior control). The transition teen developmental phase is one that encourages the isolation of teens into small affinity groups (the number who can fit in a car), and the transportation of such groups away from home environment supervisory regulations to locales where they may have a greater perception of control over their own behavior. This perception of control may be faulty because they have less familiarity with the extended environment.
Peer influence within the home environment can probably be characterized as being protective because the large (macro) peer groups formed around community institutions, such as schools and athletic teams, are likely to reflect community norms. Authority figures and parents moderate the behavior of the individual teen and the intimate peer group with which the teen most closely identifies. These influences are particularly important when small (micro) peer groups involve members with deviant behavior. The extent to which larger (macro) groups of peers will influence the behaviors of the small affiliation units will vary. In addition to these social forces, micro-group risk taking may be suppressed by limited opportunities within the protective home environment.
These small groups (intimate peers) with deviant behavioral norms find their ability to take risks and avoid detection is limited as long as travel outside the home environment is generally provided by a supervising adult. The availability of a vehicle, which is generally provided by parents or a peer, allows the transition teen to escape supervision in the home environment and find another environment where normalizing factors are not present. Before reaching high school age, with few exceptions, supervising adults have been present in the vehicle when the teen has ridden in a car. The adults have controlled the trip destination and are likely to be present at the event or at the end of the event to ensure an immediate return. This prevents exposure to risk following the sanctioned activity. When the teen drives or rides with a peer, the parents’ control over destinations and behavior at those destinations is limited.
In summary, as Figure 3 suggests, health risks for 15- to 17-year-olds involving AOD use and sexual behavior are moderated by the community, parents (and other adults), and peers of the teenager. These influences are generally normative and militate against risky behaviors. Although peer influence on this behavior has generally been viewed as a risk factor, in situations (parties, athletic events) involving a relatively broad cross-section of the teens in the home environment (community peer groups), their influence is likely to be normative. It is the smaller affinity peer groups of more deviant peers that are likely to exert a negative influence.
Extended Environment
Before driving age, all these home environment influences are omnipresent in the life of the developing child. However, once teens can move more readily within the community and travel outside the home environment on their own or with their peers, they have access to locations where many or all the local controls on risky behavior may be absent. This is suggested by the diagram in Figure 3 where, in the Extended Environment, the normalizing influence of parents or significant adults and of macro peer groups is far removed, even absent. Additional risk may be present in the extended environment in the form of increased access to AODs and exposure to crime and traffic risks not typical of the home environment.
The opportunity to drive or ride with a peer leads to two new major categories of risk (Figure 3): (1) the “novice driving” element, which includes crash injuries related to the limited skills of inexperienced drivers; and (2) the “expanded horizons” element, which includes the increased exposure to AOD use, risky sex, and victimization due to the creation within the vehicle, or the travel into, higher-risk environments. For some risks, the vehicle itself becomes a high-risk environment without necessarily leaving the home community—it creates a private micro-environment away from adult supervision where risky behaviors, such as sexual experimentation and drug use, are possible. High school is a period of intense male-female relationships with couples pairing up regularly for short periods (Arnett, 2002). The car offers privacy for sexual exchanges. It also changes the power structure in such relationships, providing the driver (normally a male) with greater control over joint activities and location, which can lead to sexual experimentation, risk of unwanted sex, and exposure to sexually transmitted diseases. The vehicle also offers an isolated environment where a small group of peers can experiment with alcohol and/or other drugs. Evidence that the availability of a vehicle to teens is related to increased risk beyond those associated with novice driving was provided by Carpenter (2005). He conducted a study of the gonorrhea rate in states that enacted ZT laws for underage drivers. He documented significant reductions in the gonorrhea rates for 15- to 19-year-olds in states that enacted such laws relative to the gonorrhea rates for 20- to 24-year-olds in those states not affected by the ZT laws. The final aspects of the model include the health risk behaviors related to separation from the protections of the home environment due to expanded horizons. A list of the major risk and protective factors faced by transition teens is provided in Figure 4.
Figure 4.
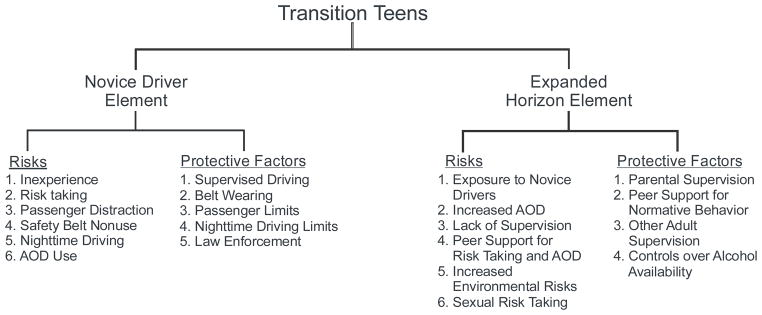
Transition Teen Problem Areas
CONCLUSION
This article introduces the concept of transitional teens and provides a rough model that explains the possible risks encountered by this group when they begin to drive a vehicle or to ride with a peer. We offer this model to the research community with a challenge to hypothesize, test, and explore it as a proposed addition to the stages of life so that we can better understand and mitigate its associated risks. The value of any theory lies in its ability to generate hypotheses that can be tested. The transition teens model presents several immediate questions that appear worthy of investigation: (1) Are youths (aged 15–17) who have access to cars more likely to use alcohol and/or other drugs? (2) Are they more likely to have early sexual experiences? (3) Are they exposed to greater environmental risks such as crime?
The model predicts that 15- to 17-year-olds whose parents manage or monitor vehicle access will be at lower risk for both crash involvement and involvement in nondriving problems related to AOD use, such as risky sex and violence. To date, driving researchers have primarily investigated the effect of parental monitoring on driving behaviors (Simons-Morton et al., 2004, 2005; Hartos et al., 2004). Initial evidence suggests that, as would be expected, where parents devote more time to supervising and enforcing clear rules, the driving behavior of their teen drivers is improved. There is evidence that a brief intervention implemented through the motor vehicle department can increase parental supervision and rule enforcement and overall driving limits (Simons-Morton et al., 2004). The Transition Teens concept suggests that such studies should be extended to see if increased parental supervision of novice drivers results in reduced AOD use. The recent passage of GDL laws by most states empowers parents by extending the learning period during which teens must have an adult in the car and, once they do begin solo driving, requiring a period during which teen passengers and nighttime driving is prohibited. These rules give parents the opportunity to exert more control over their teen’s driving (Williams and Ferguson, 2002). There is strong evidence that graduated licensing laws are effective in reducing novice driver crash involvements (Baker et al., 2006). The transition-teens concept suggests that the effect of such laws on problems related to AOD use should be determined, perhaps by the method Carpenter (2004 and 2005) used in his studies of the relationship of the ZT law to binge drinking and gonorrhea rates mentioned earlier.
A substantial number of youths entering the transition-teens period have had experience with alcohol and some with drugs. Early onset of drinking at age 14 or earlier has been shown to be associated not only with alcohol impaired driving (Hingson et al., 2002), but also with other alcohol problems (Grant and Dawson, 1998; Hingson et al., 2001, 2003). The transition teens model, which holds that availability of a vehicle raises the risk of AOD problems beyond those associated with driving itself, suggests that 15- to 17-year-olds who reported early drinking (particularly heavy episodic drinking; van Beurden et al., 2005) will show greater evidence of nonhighway, alcohol problems if they have access to a car.
In many European countries (e.g., Germany, France, and Britain), vehicles are much less available to teens and the laws governing the issuance of driver’s licenses are more restrictive, with some countries not allowing learner’s permits until age 17 or 18 years. In other countries (e.g., Nova Scotia and Ontario, Canada; Victoria, Australia; and New Zealand), a license at age 16 comes only at a substantial cost and with extensive driver training. Since in the United States adolescents may obtain a learner’s permit at age 15 years and 9 months (in most states) and become fully licensed well before age 18, an opportunity exists to compare AOD problems not directly related to crash involvement across national boundaries.
Thus, the transition-teens concept can generate a number of interesting possibilities for testing the basic assumption that the availability of a vehicle is a risk factor for AOD problems outside of those that are the direct consequences of highway crashes. It must be recognized, however, that an important limitation to the transition-teen concept is that it is almost exclusive to rural and suburban areas. In general, youth residing in urban areas, due to the proximity of resources, have less need for a vehicle and thus less access to one. Urban environments provide their own specific risks to which most suburban and rural areas are not exposed. This environmental limitation should not, however, diminish the transition-teen concept as research often targets specific populations, genders, ages, residences, and circumstances. Significant and growing percentages of youth in this age group reside in suburban and rural areas and, thus, are immediately affected by these issues. The national trend is for middle-class families, if affordable, to support the driving of their teens. Further, the move to suburban living is increasing during the transition-teen development period. The problem for these relatively affluent Americans is whether they can provide their teenagers with the opportunities for cultural and intellectual growth that access to a vehicle provides, while also protecting them from the hazards that the access to a vehicle provides. There exists a critical period when teens begin to drive or to ride with teens that deserves to be more fully examined—one that cannot be categorized as middle teen or emerging adulthood. Today’s transition teens are mobile and, thus, faced both with greater opportunities and greater risk.
References
- Arnett J. Developmental Sources of Crash Risk in Young Drivers. Inj Prev. 2002;8 :ii17–ii23. doi: 10.1136/ip.8.suppl_2.ii17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baker SP, Chen LH, Li G. National Evaluation of Graduated Driver Licensing Programs (DOT HS 810 614) for the U.S. Department of Transportation, National Highway Traffic Safety Administration; Washington, DC: 2006. [Google Scholar]
- Beck KH, Hartos JL, Simons-Morton BG. Parent-Teen Disagreement of Parent-Imposed Restrictions on Teen Driving after One Month of Licensure: Is Discordance Related to Risky Teen Driving. Prevention Science. 2005;6(3):177–185. doi: 10.1007/s11121-005-0001-6. [DOI] [PubMed] [Google Scholar]
- Beck KH, Hartos JL, Simons-Morton BG. Relation of Parent-Teen Agreement of Restrictions to Teen Risky Driving over 9 Months. American Journal of Health Behavior. 2006;30(5):533–543. doi: 10.5555/ajhb.2006.30.5.533. [DOI] [PubMed] [Google Scholar]
- Bingham CR, Shope JT. Adolescent Developmental Antecedents of Risky Driving among Young Adults. J Stud Alcohol. 2004a;65(1):84–94. doi: 10.15288/jsa.2004.65.84. [DOI] [PubMed] [Google Scholar]
- Bingham CR, Shope JT. Adolescent Problem Behavior and Problem Driving in Young Adulthood. J Adolesc Res. 2004b;19(2):205–223. [Google Scholar]
- Carpenter C. How Do Zero Tolerance Drunk Driving Laws Work. J Health Econ. 2004;23(1):61–83. doi: 10.1016/j.jhealeco.2003.08.005. [DOI] [PubMed] [Google Scholar]
- Carpenter C. Youth Alcohol Use and Risky Sexual Behavior: Evidence from Underage Drunk Driving Laws. J Health Econ. 2005;24:613–628. doi: 10.1016/j.jhealeco.2004.09.014. [DOI] [PubMed] [Google Scholar]
- Chen LH, Baker SP, Li G. Graduated Driver Licensing Programs and Fatal Crashes of 16 Year Old Drivers: A National Evaluation. Pediatrics. 2006;118:56–62. doi: 10.1542/peds.2005-2281. [DOI] [PubMed] [Google Scholar]
- Farrow JA. Young Driver Risk-Taking: A Description of Dangerous Driving Situations among Sixteen to Nineteen-Year-Old Drivers. International Journal of the Addictions. 1987;22(12):1255–1267. doi: 10.3109/10826088709027485. [DOI] [PubMed] [Google Scholar]
- Ferguson SA, Fields M, Voas RB. Enforcement of Zero Tolerance Laws in the Us – Prevention Section. In: Laurell H, Schlyter F, editors. Alcohol, Drugs and Traffic Safety – T 2000; Proceedings of the 15th International Conference on Alcohol, Drugs and Traffic Safety; May 22–26, 2000; Stockholm, Sweden: ICADTS; 2000. pp. 713–718. [Google Scholar]
- Ferguson SA, Leaf WA, Williams AF, Preusser DF. Differences in Young Driver Crash Involvement in States with Varying Licensure Practices. Accid Anal Prev. 1996;28:171–180. doi: 10.1016/0001-4575(95)00051-8. [DOI] [PubMed] [Google Scholar]
- Foss R, Goodwin A. Enhancing the Effectiveness of Graduate Driver Licensing Legislation. J Safety Res. 2003;34:79–84. doi: 10.1016/s0022-4375(02)00083-x. [DOI] [PubMed] [Google Scholar]
- Foss RD, Feaganes JR, Roggman LA. Initial Effects of Graduated Driver Licensing on 16-Year-Old Driver Crashes in North Carolina. JAMA. 2001;286(13):1631–1632. doi: 10.1001/jama.286.13.1588. [DOI] [PubMed] [Google Scholar]
- Frith WJ, Perkins WA. The New Zealand Graduated Licensing System. Paper presented at: National Road Safety Seminar; Wellington, New Zealand. 1992. [Google Scholar]
- Grant BF, Dawson DA. Age of Onset of Drug Use and Its Association with DSM-IV Drug Abuse and Dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse. 1998;10(2):163–173. doi: 10.1016/s0899-3289(99)80131-x. [DOI] [PubMed] [Google Scholar]
- Grube JW, Nygaard P. Alcohol Policy and Youth Drinking: Overview of Effective Interventions for Young People. In: Stockwell T, Gruenewald PJ, Tournbourou J, Loxley W, editors. Preventing Harmful Substance Use: The Evidence Base for Policy and Practice. Wiley; New York: 2005. pp. 113–127. [Google Scholar]
- Hartos JL, Shattuck T, Simons-Morton BG, Beck KH. An in-Depth Look at Parent-Imposed Driving Rules: Their Strengths and Weaknesses. J Safety Res. 2004;35:547–555. doi: 10.1016/j.jsr.2004.09.001. [DOI] [PubMed] [Google Scholar]
- Hingson R, Heeren T, Levenson S, Jamanka A, Voas RB. Age of Drinking Onset, Driving after Drinking, and Involvement in Alcohol-Related Motor Vehicle Crashes. Accid Anal Prev. 2002;34(1):85–92. doi: 10.1016/s0001-4575(01)00002-1. [DOI] [PubMed] [Google Scholar]
- Hingson R, Heeren T, Zakocs R. Age of Drinking Onset and Involvement in Physical Fights after Drinking. Pediatrics. 2001;108(4):872–877. doi: 10.1542/peds.108.4.872. [DOI] [PubMed] [Google Scholar]
- Hingson R, Heeren T, Zakocs R, Winter M, Wechsler H. Age of First Intoxication, Heavy Drinking, Driving after Drinking and Risk of Unintentional Injury among U.S. College Students. J Stud Alcohol. 2003;64(1):23–31. doi: 10.15288/jsa.2003.64.23. [DOI] [PubMed] [Google Scholar]
- Kypri K, McCarthy DM, Coe MT, Brown SA. Transition to Independent Living and Substance Involvement of Treated and High Risk Youth. Journal of Child and Adolescent Substance Abuse. 2004;13(3):85–100. [Google Scholar]
- LaScala E, Freisthler B, Gruenewald PJ. Population Ecologies of Drug Use, Drinking and Related Problems. In: Stockwell T, Gruenewald PJ, Toumbourou JW, Loxley W, editors. Preventing Harmful Substance Use: The Evidence Base for Policy and Practice. John Wiley & Sons, Ltd; Chichester, West Sussex, England: 2005. pp. 67–78. [Google Scholar]
- Masten SV, Hagge RH. Evaluation of California’s Graduated Driver Licensing Program. J Safety Res. 2004;35:523–535. doi: 10.1016/j.jsr.2004.08.006. [DOI] [PubMed] [Google Scholar]
- Mayhew DR, Simpson HM. The Safety Value of Driver Education and Training. Journal of the International Society for Child and Adolescent Injury Prevention. 2002;8(Suppl II):ii3–8. doi: 10.1136/ip.8.suppl_2.ii3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayhew DR, Simpson HM, Williams AF, Ferguson SA. Effectiveness and Role of Driver Education and Training in a Graduated Licensing System. J Public Health Policy. 1998;19(1):51–67. [PubMed] [Google Scholar]
- McCarthy DM, Brown SA. Changes in Alcohol Involvement, Cognitions and Drinking and Driving Behavior for Youth after They Obtain a Driver’s License. J Stud Alcohol. 2004;65(3):289–296. doi: 10.15288/jsa.2004.65.289. [DOI] [PubMed] [Google Scholar]
- McKnight AJ, Hyle P, Albrecht L. Youth License Control Demonstration Project (DOT HS 7 01765) for the National Highway Traffic Safety Administration; Washington, DC: 1983. [Google Scholar]
- National Highway Traffic Safety Administration. Graduated Driver Licensing System. Traffic Safety Facts: Laws. National Highway Traffic Safety Administration; [Accessed September, 2006.]. Available at: www.nhtsa.gov. [Google Scholar]
- National Safety Council. Teen Driver: A Family Guide to Teen Driver Safety. for the National Safety Council; Washington, DC: 2005. [Google Scholar]
- Poulin C, Boudreau B, Asbridge M. Adolescent Passengers of Drunk Drivers: A Multi-Level Exploration into the Inequities of Risk and Safety. Addiction. 2007;102(1):51–61. doi: 10.1111/j.1360-0443.2006.01654.x. [DOI] [PubMed] [Google Scholar]
- Preusser DF, Leaf WA, Ferguson SA, Williams AF. Variations in Teenage Activities with and without a Drivers License. J Public Health Policy. 2000;21(2):224–239. [PubMed] [Google Scholar]
- Senserrick T, Haworth N. Young Driver Research: Where Are We Now? What Do We Still Need to Know?. Paper presented at: Road Safety Research, Education, and Policing Conference; Perth, Australia/Clayton, Victoria, Australia. 2004. [Google Scholar]
- Shope JT, Bingham CR. Drinking-Driving as a Component of Problem Driving and Problem Behavior in Young Adults. J Stud Alcohol. 2002;63(1):24–33. [PubMed] [Google Scholar]
- Shope JT, Elliott MR, Raghunathan TE, Waller PF. Long-Term Follow-up of a High School Alcohol Misuse Prevention Program’s Effect on Students’ Subsequent Driving. Alcoholism, Clinical and Experimental Research. 2001a;25(3):403–410. [PubMed] [Google Scholar]
- Shope JT, Molnar LJ. Michigan’s Graduated Driver Licensing Program: Evaluation of the First Four Years. J Safety Res. 2004;35(3):337–344. doi: 10.1016/j.jsr.2004.04.001. [DOI] [PubMed] [Google Scholar]
- Shope JT, Molnar LJ, Elliott MR, Waller PF. Graduated Driver Licensing in Michigan: Early Impact on Motor Vehicle Crashes among 16 Year-Old Drivers. JAMA. 2001b;286(13):1593–1598. doi: 10.1001/jama.286.13.1593. [DOI] [PubMed] [Google Scholar]
- Shults RA, Elder RW, Sleet DA, et al. Reviews of Evidence Regarding Interventions to Reduce Alcohol-Impaired Driving. Am J Prev Med. 2001;21(4 Suppl):66–88. doi: 10.1016/s0749-3797(01)00381-6. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Hartos JL, Beck KH. Increased Parent Limits on Teen Driving: Positive Effects from a Brief Intervention Administered at the Motor Vehicle Administration. Prev Sci. 2004;5(2):101–111. doi: 10.1023/b:prev.0000023080.76550.ab. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Hartos JL, Leaf WA, Preusser DF. Persistence of Effects of the Checkpoints Program on Parental Restrictions of Teen Driving Privileges. Am J Public Health. 2005;95(3):447–452. doi: 10.2105/AJPH.2003.023127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanner JL. Recentering During Emerging Adulthood: A Critical Turning Point in Life Span Human Development. In: Arnett JJ, Tanner JL, editors. Emerging Adults in America: Coming of Age in the 21st Century. American Psychological Association; Washington, DC: 2006. [Google Scholar]
- The Auto Channel. Majority Killed in Teen Driver Crashes Are Passengers, Other Drivers; Aaa to Focus Advocacy Efforts on Strengthening Teen Driver Safety Laws. [Accessed March 09, 2006];The Auto Channel. Available at: http://www.theautochannel.com/news/2006/01/18/207699.html.
- The Center for Injury Research and Prevention at The Children’s Hospital of Philadelphia and State Farm Mutual Automobile Insurance Company. Driving through the Eyes of Teens: A Research Report of the Children’s Hospital of Philadelphia and State Farm. The Children’s Hospital of Philadelphia; Philadelphia, PA: 2007. [Google Scholar]
- van Beurden E, Zask A, Brooks L, Dight R. Heavy Episodic Drinking and Sensation Seeking in Adolescents as Predictors of Harmful Driving and Celebrating Behaviors : Implications for Prevention. J Adolesc Health. 2005;27(1):37–43. doi: 10.1016/j.jadohealth.2004.11.132. [DOI] [PubMed] [Google Scholar]
- Voas RB, Tippetts AS, Fell J. Assessing the Effectiveness of Minimum Legal Drinking Age and Zero Tolerance Laws in the United States. Accid Anal Prev. 2003;35(4):579–587. doi: 10.1016/s0001-4575(02)00038-6. [DOI] [PubMed] [Google Scholar]
- Williams AF. Magnitude and Characteristics of the Young Driver Crash Problem in the United States. In: Simpson HM, editor. New to the Road: Reducing the Risks for Young Motorists. Youth Enhancement Service, Brain Information Service, UCLA School of Medicine; 1996. pp. 19–25. [Google Scholar]
- Williams AF. Graduated Licensing Comes to the United States. Inj Prev. 1999;5(2):133–135. doi: 10.1136/ip.5.2.133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams AF, Ferguson SA. Rationale for Graduated Licensing and the Risks It Should Address. Inj Prev. 2002;8(suppl II):ii9–ii13. doi: 10.1136/ip.8.suppl_2.ii9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams AF, Ferguson SA. Driver Education Renaissance? Inj Prev. 2004;10(1):4–7. doi: 10.1136/ip.2003.004358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams AF, Ferguson SA, Leaf WA, Preusser DF. Views of Parents of Teenagers About Graduated Licensing Systems. J Safety Res. 1998;29(1):1–7. [Google Scholar]
- Williams AF, Preusser DF. Night Driving Restrictions for Youthful Drivers: A Literature Review and Commentary. J Public Health Policy. 1997;18(3):334–345. [PubMed] [Google Scholar]
- Williams AF, Preusser DF, Lund AK. High School Students’ Views of Laws Restricting Teenage Driving. J Public Health Policy. 1984;5(3):387–395. [PubMed] [Google Scholar]
- Williams AF, Preusser DF, Lund AK, Rasmussen SJ. Cars Owned and Driven by Teenagers. Transportation Quarterly. 1987;41:177–188. [Google Scholar]
- Womack KN, Trout NH, Davies BJ. Characteristics and Conditions of Teenage Safety Belt Use (DOT HS 808 676) U.S. Department of Transportation, National Highway Traffic Safety Administration; College Station, TX: 1997. [Google Scholar]