

Abstract
Local, state, and national policies that limit the hours that alcoholic beverages may be available for sale might be a means of reducing excessive alcohol consumption and related harms. The methods of the Guide to Community Preventive Services were used to synthesize scientific evidence on the effectiveness of such policies. All of the studies included in this review assessed the effects of increasing hours of sale in on-premises settings (in which alcoholic beverages are consumed where purchased) in high-income nations. None of the studies was conducted in the U.S. The review team’s initial assessment of this evidence suggested that changes of less than 2 hours were unlikely to significantly affect excessive alcohol consumption and related harms; to explore this hypothesis, studies assessing the effects of changing hours of sale by less than 2 hours and by 2 or more hours were assessed separately.
There was sufficient evidence in ten qualifying studies to conclude that increasing hours of sale by 2 or more hours increases alcohol-related harms. Thus, disallowing extensions of hours of alcohol sales by 2 or more should be expected to prevent alcohol-related harms, while policies decreasing hours of sale by 2 hours or more at on-premises alcohol outlets may be an effective strategy for preventing alcohol-related harms. The evidence from six qualifying studies was insufficient to determine whether increasing hours of sale by less than 2 hours increases excessive alcohol consumption and related harms.
Introduction
Excessive alcohol consumption is responsible for approximately 79,000 deaths per year in the U.S., making it the third-leading cause of preventable death.1 Binge drinking (consuming five or more drinks per occasion for men and four or more drinks per occasion for women) is reported by approximately 15% of U.S. adults aged ≥18 years and by approximately 29% of high school students in the U.S.2,3 The direct and indirect economic costs of excessive drinking in 1998 were $184.6 billion.4 The reduction of excessive alcohol consumption in general and binge drinking in particular are thus matters of major public health and economic interest. Reducing binge drinking among U.S. adults has been a public health objective in Healthy People 2010.5
In the U.S., local control of the total or specific hours during which alcoholic beverages may be sold (hereafter referred to as “hours of sale”) varies from one state to another. Some states allow cities, counties, and other local jurisdictions to enact their own alcohol control policies, and in these states, restrictions on hours of sale can vary from one location to another. In other states, local control may be pre-empted by state regulations that prohibit local authorities from enacting alcohol control regulations stricter than those that apply to the rest of the state.6,7 As of 1953, American Indian reservations have the authority to establish their own alcohol-related policies, prior to which alcohol was formally prohibited.8
There is also wide variation among states in the specific restrictions they place on the hours of sale by retail setting (i.e., on- or off-premises) and by the day of the week.9 For on-premises alcohol outlets, states allow facilities to serve alcohol for a median of 19 hours a day on weekdays and Saturdays. Nine states (Alabama, Florida, Georgia, Illinois, Louisiana, Maryland, Nevada, New Jersey, and South Carolina) have no limits on hours of sale for on-premises alcohol outlets.9 On Sundays, alcohol may be served for a median of 17 hours at on-premises facilities, with seven states placing no restrictions on Sunday on-premises sales; four states allow no sales of alcohol at on-premises facilities on Sundays. In off-premises settings, hours of sale are limited to a median of 18 hours on weekdays and Saturdays. Restrictions range from no limits on hours of sale in Alabama, Florida, Georgia, Illinois, Louisiana, Maryland, and Nevada to 8 hours of sale allowed in Idaho. On Sundays, states allow a median of 13 hours of alcohol sales at off-premises facilities, with five states having no restrictions; 18 states with “blue laws” allow no off-premises sales.
This review uses the methods of the Guide to Community Preventive Services (Community Guide)10 to assess the effects of changes in the hours during which alcohol is served on excessive alcohol consumption and related harms. A separate review published in this issue assesses the effects of changing days of sale on excessive alcohol consumption and related harms and concludes that increasing days of sale leads to increased consumption and related harms. The focal question of the present review is how, within allowable days of sale, the number of hours available for acquisition and service of alcohol affects excessive alcohol consumption and related harms.
Findings and Recommendations from Other Reviews and Advisory Groups
Several scientific reviews11–14 have concluded that restricting the hours when alcohol may be sold is an effective strategy for reducing excessive alcohol consumption and related harms. One review,11 funded by the Center for Substance Abuse Prevention (CSAP), found substantial evidence of harms associated with expanding the hours and days of alcohol sales. This conclusion was based on previous empirical research indicating that the expansion of the hours and days of sale increased prevalence of excessive alcohol consumption and alcohol-related problems. Most prior reviews have combined findings on days and hours and none have examined a threshold effect. The CSAP review included studies prior to 1999; a recent review14 includes studies published between 2000 and 2008. The present review covers both periods using the systematic methods of the Community Guide described below.
Several international bodies have also recommended the control of hours or days of sale, or both as means of reducing excessive alcohol consumption and related harms.15 For example, a recent review16 of alcohol control strategies by the WHO found that limiting of hours of sale was an effective method for reducing alcohol-related harms. In Ireland, the Department of Health and Children’s Strategic Task Force on Alcohol17 concluded (p. 30) that “restricting any further increases in the physical availability of alcohol (number of outlets and times of sales)” is among the most effective policy measures for influencing alcohol consumption and related harms.
Methods
The methods of the Community Guide were used to systematically review scientific studies that have evaluated the effectiveness of limiting or maintaining existing limits on the hours of sale for preventing excessive alcohol consumption and related harms.10 In brief, the Community Guide process involves forming a systematic review development team (review team), consisting of subject matter and methodology experts from other parts of the CDC, other federal agencies, and academia, and the Task Force on Community Preventive Services (Task Force); developing a conceptual approach for organizing, grouping, and selecting interventions; selecting interventions to evaluate; searching for and retrieving available research evidence on the effects of those interventions; assessing the quality of and abstracting information from each study that meets inclusion criteria; assessing the quality of and drawing conclusions about the body of evidence on intervention effectiveness; and translating the evidence on effectiveness into recommendations. Evidence is collected and summarized on (1) the effectiveness of reviewed interventions in altering selected health-related outcomes and (2) positive or negative effects of the intervention on other health and nonhealth outcomes. When an intervention is shown to be effective, information is also included about (3) the applicability of evidence (i.e., the extent to which available effectiveness data might generalize to diverse population segments and settings); (4) barriers to implementation; and (5) the economic impact of the intervention. To help ensure objectivity, the review process is typically led by scientists who are not employed by a program that might be responsible for overseeing the implementation of the intervention being evaluated.
The results of this review process are then presented to the Task Force, an independent scientific review board that objectively considers the scientific evidence on intervention effectiveness presented to them and then determines, with the guidance of a translation table, whether the evidence is sufficient to warrant a recommendation on intervention effectiveness.10 Evidence can be found to be strong, sufficient, or insufficient. Sufficient or strong evidence may indicate benefit, harm, or ineffectiveness of the intervention whereas insufficient evidence indicates more research is needed.
Conceptual Approach and Analytic Framework
The premise of this review is that increased availability of alcoholic beverages through any mechanism facilitates increases in excessive consumption and related harms, and that limiting hours of sale of alcoholic beverages is one way to reduce availability. The limitation of hours of sale of alcoholic beverages was defined as “applying regulatory authority to limit the hours that alcoholic beverages may be sold at on- and off-premises alcoholic beverage outlets.” Limiting may refer to either maintaining existing limits in response to efforts to expand hours of sale or reducing current limits on hours of sale. Hours of sale may be regulated at the national, state, or local level or some combination of these. Off-premises retailing refers to the sale of contained alcoholic beverages, for instance, at package stores, liquor stores, grocery stores, or convenience stores, for consumption elsewhere. On-premises retailing refers to the sale of alcoholic beverages for consumption at the point of sale, for example, at bars, restaurants, or clubs.
Policies that regulate the hours of sale may be influenced by various characteristics of the affected population, including the demand for alcoholic beverages, the age distribution of the population, the religious affiliation and involvement of residents, and the amount of tourism the area attracts. Policies reducing or expanding hours of sale are hypothesized to affect alcohol consumption and alcohol-related harms through the following means (Figure 1). First, increases or decreases in the hours of sale affect consumers’ ability to purchase alcohol by changing its availability. Second, when access to alcoholic beverages changes, consumers may alter their purchasing habits in several ways, including changing their purchase volume, rescheduling their purchases, relocating their purchases, or obtaining alcoholic beverages illegally. Changes in their purchasing habits may then affect their drinking patterns or overall levels of alcohol use, resulting in changes in alcohol-related problems.
Figure 1.
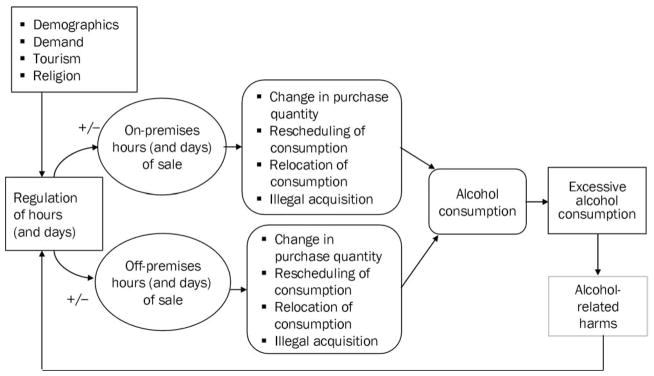
Effects of regulation of hours (and days) of alcohol sales on excessive alcohol consumption and related harms
Changes in the hours of sale may also affect alcohol-related health outcomes by other means. For example, increases in the hours that alcohol is available at on-premises outlets may be associated with increased social aggregation, which, in turn, may increase aggressive behaviors that are exacerbated by alcohol consumption.18 Increases or decreases in the hours that alcohol is available in one jurisdiction may also increase or decrease alcohol consumption in adjacent jurisdictions if consumers travel from a jurisdiction with fewer hours to one with greater hours. This may also affect the number of miles traveled to purchase alcohol, and therefore the probability of alcohol-related motor vehicle crashes.
The present review addresses the following research question: what are the effects on excessive alcohol consumption and related harms of changing the hours of sale at on- or off-premises outlets? It was hypothesized that there would be a dose–response relationship related to the magnitude of the change in hours (i.e., the amount by which hours of sale are increased or decreased). Based on this hypothesis, the body of evidence for this review was stratified into studies examining changes of ≥2 hours and <2 hours per day. This cut point was chosen by the judgment of the review team that 2 hours might be a reasonable threshold for a substantial effect and on the distribution of available studies.
The process by which hours of alcohol sale are changed in different settings may also be an important variable to consider in evaluating the effects of such changes. In some settings in which the allowable hours of sale are increased, any licensed facility may extend hours. In others, facilities must apply for an extension and meet certain criteria, such as demonstrating a lack of facility crowding in a neighborhood. It was hypothesized that the additional level of regulation required to apply for extended opening hours might reduce the potential harm from greater access by restricting the implementation and extent of added hours.
Inclusion and Exclusion Criteria
To be included as evidence in this review, studies had to meet certain criteria. First, studies that assessed short-term changes in alcohol availability (e.g., alcohol sales related to a special event such as a sports competition) were not included. Second, eligible studies needed to assess the specific impact of changes in the hours of sale on excessive alcohol consumption, related harms, or both, as opposed to evaluating the effect of change in combination with other interventions. Studies of combined interventions may obscure the effects attributable specifically to changes in hours. Third, because the current focus was on the effects of changes in hours of sale in jurisdictions where these changes occurred, no review was made of studies that examined the effects of changes in hours in one jurisdiction on consumption elsewhere, for example, in neighboring jurisdictions or across a border. Fourth, to increase the applicability of the findings to the U.S., studies had to be conducted in countries with high-income economiesa according to the World Bank.19 Fifth, studies had to present primary research findings, not just review other research findings. Sixth, studies had to be published in English. Seventh, studies had to have a comparison group or, at a minimum, compare outcomes of interest before and after a change in the policy related to hours of sale.
Specific types of alcohol-related harms of interest were alcohol-related diseases (e.g., liver cirrhosis), alcohol-impaired driving, alcohol-related crashes, unintentional or intentional injuries, and violent crime. When studies assessed multiple outcomes of interest, those outcomes with the strongest known association with excessive alcohol consumption were selected. Outcome measures that had the strongest known association with excessive alcohol consumption included binge drinking, heavy drinking, liver cirrhosis mortality, alcohol-related medical admissions, and alcohol-related motor vehicle crashes, including single-vehicle night-time crashes (which are widely used to indicate the involvement of excessive drinking).20 Less-direct measures included per capita ethanol consumption, a recognized proxy for estimating the number of heavy drinkers in a population21; unintentional injuries; suicide; and crime, such as homicide and aggravated assault.
Search for Evidence
The following databases were searched: Econlit, PsycINFO, Sociology Abstracts, MEDLINE, Embase, and EtOH. All years of records available on the databases were searched up to February 2008. Although the systematic search ended at this date, the review team is not aware of additional hours of sale research published since this time. (The search strategy will be available on the Community Guide website.) The reference lists of articles reviewed were also searched as well as reference lists from other systematic reviews. Government reports were considered for inclusion, but unpublished papers were not. Subject matter experts were also consulted to identify studies that might have been missed.
Assessing the Quality and Summarizing the Body of Evidence on Effectiveness
Each study that met the inclusion criteria was read by two reviewers who used standardized criteria to assess the suitability of the study design and threats to validity.10 Uncertainties and disagreements between the reviewers were reconciled by consensus among the review team members. Classification of the study designs accords with the standards of the Community Guide review process and may differ from the classification reported in the original studies.
Studies were evaluated based on their design and execution. Those that collected data on exposed and control populations prospectively were classified as having the greatest design suitability. Those that collected data retrospectively or lacked a comparison group, but that conducted multiple pre- and post-measurements on their study population(s), were rated as having moderate design suitability. Finally, cross-sectional studies, those without a comparison group, and those that involved only a single pre- or post-measurement in the intervention population were considered to have the least suitable design. Quality of execution was assessed by examining potential threats to study validity, including an inadequate description of the intervention or of the study population(s), poor measurement of the exposure or outcome, failure to control for potential confounders, and a high attrition rate among study participants. Based on these criteria, studies were characterized as having good quality of execution if they had at most one threat to validity; fair execution if they had two to four threats to validity, and limited quality of execution if they had five or more threats to validity. For example, studies that used only proxy outcome measures were assigned a penalty for this threat to validity. Only studies with good or fair quality of execution were included in the body of evidence; studies with any level of design suitability were included, other than those with cross-sectional design.
Effect estimates were calculated as relative percentage change in the intervention population compared with the control population using the following formulas:
-
For studies with pre- and post-measurements and concurrent comparison groups:
Effect estimate=(Ipost/Ipre)/(Cpost/Cpre)−1,
where:
Ipost=last reported outcome rate or count in the intervention group after the intervention;
Ipre=reported outcome rate or count in the intervention group before the intervention;
Cpost=last reported outcome rate or count in the comparison group after the intervention;
Cpre=reported outcome rate or count in the comparison group before the intervention.
-
For studies with pre- and post-measurements but no concurrent comparison:
Effect estimate=(Ipost−Ipre)/Ipre
All studies included in this review assessed the effects of increasing hours of sale, and the control condition was not increasing hours of sale. Although the analysis here accordingly assesses the effects of increasing hours, the public health intervention of interest is the control condition, (i.e., limiting or not increasing hours of sale). This approach rests on the assumption that increasing availability by increasing hours is likely to increase excessive consumption and related harms, and thus not increasing hours when proposed is the public health intervention. For each body of evidence, the review reports a number of events of policy changes in hours in a given jurisdiction, each of which may have been the subject of more than one study (a research investigation carried out by a single researcher or research group), each of which, in turn, may have been reported in more than one paper or report.
Results on Intervention Effectiveness
Studies of Changes of >2 Hours in Hours of Sale
Ten studies22–31 of six events that resulted in a change of ≥2 hours in the hours of alcohol sales met the inclusion criteria. Only one study22 was of greatest design suitability; however, the principal analysis in this study was presented graphically and did not allow the estimation of a numeric effect size. One study23 was of moderate design suitability and eight24–31 were of least suitable design. All studies had fair quality of execution. (A summary evidence table [Table 1]22–40 accompanies this review.)
Table 1.
Evidence of the effects of limits of alcohol hours of sale on excessive alcohol consumption and related harm
| Study/design/execution | Population/study time period | Intervention/comparison | Analysis/outcome | Reported findings | Review/effect size |
|---|---|---|---|---|---|
| Policies allowing a change of ≥2 hours—Increasing hours | |||||
| El-Maaytah (2008)29 Design suitability: Least Pre/post, no control Quality of execution: Fair (4 limitations) |
Location: University College Hospital, London, England, and Wales Dates: Intervention: November 24, 2005 Pre-intervention: November 24, 2004–April 30, 2005 Post-intervention: November 24, 2005–April 30, 2006 |
Intervention: Flexible opening hours: Potentially 24-hour opening, 7 days a week, dependent on special license Note: Granting of licenses subject to consideration of impact on local residents, businesses, and expert opinion Control: None |
Analysis: Chi-square Outcome: ARMT (6 months before compared to 6 months after) |
ARMT Pre: 1102 Post: 730 |
Relative % change (95% CI): −33.8% (−39.7, −27.3) |
| Newton (2007)27 Design suitability: Least Pre/post, no comparison Quality of execution: Fair (3 limitations) |
Location: London Dates: Intervention: November 2005 Pre-intervention: March 2005 (9:00PM–9:00AM) Post-intervention: March 2006 (9:00PM–9:00AM) |
Intervention: Experimental unrestricted hours Control: None |
Analysis: Mann–Whitney U test for differences in proportions Outcomes: Numbers and percentages of “alcohol-related” ER admissions, injuries, and hospital referrals |
Significant increases in number of alcohol-related admissions, alcohol-related assault, alcohol-related injury, and alcohol-related hospital admissions | Relative % change (95% CI): Alcohol-related assault: 129.6 (46.1, 260.8) Alcohol-related injury: 193.2 (108.2, 312.8) |
| Babb (2007)28 Design suitability: Least Pre/post, no comparison Quality of execution: Fair (3 limitations) |
Location: London Dates: Intervention: November 2005 Pre-intervention: December 2004–November 2005 (9:00PM–9:00AM) Post-intervention: December 2005– November 2006 (9:00PM –9:00AM) |
Intervention: Experimental unrestricted hours, along with fines/ penalties for service to drunk clients and children Control: None |
Analysis: 30 of 43 home office police forces provide data on arrests for serious and less-serious violent crimes. Offenses not specified as alcohol- related |
Moving averages calculated for nighttime arrests, 6:00PM to 5:59 AM | Relative % change: Serious offenses (including homicide and manslaughter): −9.5% Less-serious offenses (with wounding): −5.4% Less-serious offenses (with wounding) in city centers and near licensed premises: −4.3% Assault without injury: −2.7% Assault without injury in city centers and near licensed premises: 3.1% |
| Ragnarsdottir (2002)26 Design suitability: Least Pre/post, no comparison Quality of execution: Fair (3 limitations) |
Location: “relatively small” city center, Reykjavik Dates: Intervention: July 1999–July 2000 Pre-intervention: March 1999–April 1999 (8 weekend nights) Post-intervention: March 2000–April 2000 (8 weekend nights) *Weekend nights defined as Saturday or Sunday from 12:00 MN to 7:00AM |
Intervention: Experimental unrestricted hours Control: Unchanged hours |
Analysis: Percentages; no tests of significance Outcomes:
|
For all outcomes, location not specified as city center (the location of intervention) or outside city center. Emergency ward admissions: Weekend nights: 31% increase All-day: 3% increase Weekends (all day): 20% increase Weekdays: 2% decrease Reasons for admission include incidents often related to drinking: Accidents and other mishaps: 23% increase Fighting: 34% increase Non–alcohol-related admission types: No change Suspected drunk driving: 1999: 29 2000: 52 |
Relative % change: Weekend emergency ward admissions: 20%* Accidents and other mishaps: 23%* Fighting: 34%* Suspected drunk driving: 79.3% (13.8, 182.4) |
| Smith (1988)25 Design suitability: Least Pre/post, no comparison group Quality of execution: Fair (3 limitations) |
Location: Tasmania, Australia Dates: Intervention: August 10, 1977 Pre-intervention: July 1, 1971–June 30, 1977 Follow-up: October 1, 1977–September 30, 1978 |
Intervention: Unrestricted hours allowed throughout week. Smith reports numbers of actual hours did not change, but hours shifted to later times. Exceptions (mandatory closing): Sundays 5:00 AM–12:00NOON Sundays 8:00PM–12:00MN Good Friday Prior hotel opening hours: Monday–Saturday: 10:00 AM–10:00PM Sunday: 12:00NOON–8:00PM Control: Number of injury crash from 6:00 PM to 10:00PM |
Analysis: Chi-square Outcome: Crash injury between 10:00PM and 6:00AM |
Traffic injury crash: Increased between 10:00PM and 6:00AM. Although the number occurring directly after the former closing time decreased, both the proportion and the absolute number of traffic injury crash from 12:00MN to 6:00AM increased, for a total overall increase. |
Relative % change (95% CI): Traffic injury crash: 10.8% (−1.5, 21.2) |
| Raymond (1969)22 Design suitability: Greatest Pre/post, no comparison. Quality of execution: Fair (3 limitations) |
Location: Melbourne, Victoria (Australia) Dates: Intervention: February 1, 1966 Pre-intervention: 1964–1965 Follow-up: 1966–1967 after period Note: data collection begins January 1, 1966 |
Intervention: Closing time extended from 6:00PM to 10:00PM Control: Sundays |
Analysis: Outcomes:
|
Summary of major findings: Total accidents: No change Hourly distribution of accidents occurring from 6:00PM to 11:00PM changed significantly: Sharp decrease from 6:00PM to 7:00PM and an increase from 10:00PM to 11:00PM. |
Graphical comparison of weekdays and Saturday with hours change vs Sunday without change: No effect |
| Williams (1972)23 Design suitability: Moderate Interrupted time series Quality of execution: Fair (2 limitations) |
Location: Victoria, Australia Dates: Intervention: January 2, 1966 Pre-intervention: 1958–1966 Follow-up: 1966–1969 |
Intervention: Closing time extended from 6:00PM to 10:00PM Control: None |
Analysis: Maximum likelihood estimates Outcome: Consumption of alcohol in Aus$ sales per capita controlled for price of beer and consumer price index |
Sales increase $1.9 per quarter due to 10:00PM closing Equivalent to 12% increase Note: Author reports no significant effect because SEs are large |
Consumption change: 12% (ns)* * CIs not calculable because of lack of data |
| Smith (1988)24 | Location: Victoria, Australia Dates: Intervention: January 2, 1966 |
Intervention: Closing time extended from 6:00 PM to 10:00PM Control: None |
Injury crash change: Yearly vehicle crashes 3 years before and 1 year after the change in hours. No assessment of alcohol- relatedness of crashes | An increase of 11.5% in automobile crash injuries associated with the change in hours (not taking entire day into account) | Relative % change (95% CI): 3.6% (−16.6, 28.8) |
| Smith (1990)30 Design suitability: Least Pre/post, no comparison Quality of execution: Fair (3 limitations) |
Location: Victoria, Australia Dates: Intervention:
Pre-intervention: January 1, 1980–December 31, 1983 Follow-up (1): January 1, 1984–December 31, 1984 Follow-up (2): January 1, 1985–December 31, 1985 |
Intervention:
Control: None |
Analysis: Chi-squares Outcome: Traffic crash injury |
Injury crash during the 4 hours after 8-hour Sunday session | Relative % change (95% CI): 8.5 (2.2, 15.2) |
| Briscoe (2003)31 Design suitability: Least Cross-sectional Quality of execution: Fair (3 limitations) |
Location: Victoria, Australia Dates: Intervention: July 1998–June 2000 |
Intervention: 24-hour permit granted to some on- premises alcohol outlets | Analysis: descriptive statistics Outcomes: Number of assaults within outlets during study period |
Summary of major findings: Authors claim that there is an association between 24-hour permits and high rates of assaults. However, findings appear contradictory and do not allow re-evaluation. |
Inconclusive |
| Policies allowing a change of <2 hours | |||||
| Chikritzhs (1997)32–35 Design suitability: Greatest Before and after design with comparison Quality of execution: Fair (3 penalties) |
Location: Perth, Western Australia (WA) Dates: Data collected from July 1, 1991 to June 30, 1995 for:
Data collected from July 1, 1990 to June 30, 1996 for:
|
Intervention (1988): ETPs only (until 1:00AM instead of 12MN) Control: Hotels that served in standard hours (until 12: 00MN) throughout study period (non-ETPs) |
Analysis to test for ETP association:
Outcomes:
|
Monthly assaults per hotel: ETP hotels: Pre: 0.121; Post: 1.87 Non-ETP hotels: Pre: 0.112; Post: 0.133 * Adjusting for alcohol sales eliminated effect of ETPs (e.g., increased consumption accounted for increased harm) ETP hotels: Pre: 670,403; Post: 881,048 Non-ETP hotels: Pre: 686,094; Post: 815,822 Alcohol-related road crashes: ETP hotels: Pre: 0.0781; Post: 0.0808 Non-ETP hotels: Pre: 0.0731; Post: 0.0503 |
Relative % change: Monthly assaults per hotel: 30.1% Wholesale alcohol purchases: 10.5% Alcohol-related road crashes: 51.3% |
| Smith (1987)36 Design suitability: Least Before and after design, no comparison Quality of execution: Fair (3 penalties) |
Location: New South Wales, Australia Dates: Intervention: Weekday/Saturday closing hours: changed from 10:00PM to 11:00PM Pre-intervention: 1976–1979 Follow-up: 1980–1981 |
Intervention: Hours: Weekday/Saturday evening closing hours extended from 10:00PM to 11:00PM December 1979 Sunday hours and outlet types also expanded December 1980 BAC levels lowered from 0.08% to 0.05% Control: No comparison group |
Analysis: Percentage change Outcomes: Motor vehicle fatalities |
Summary of major findings: Findings on this outcome not considered |
Relative % change in motor vehicle fatalities: −2.7% |
| Knight (1980)37 Design suitability: Least Before and after study without comparison Quality of execution: Fair (4 limitations) |
Location: 4 major cities and central belt of Scotland Dates: Intervention: Hours: December 13, 1976 Pre-intervention: October–November 1976 Follow-up: March 1977 |
Intervention: Hours: Evening closing hours extended from 10:00PM to 11:00PM in December 1977 (Sunday licenses issued October 1977) Control: No comparison group |
Analysis: Percentage changes Outcomes: Consumption and patterns of consumption |
Change in consumption (in standard units) from before to after the time change: Men: −0.9 units/week Women: 0.2 units/week |
Relative % change in consumption following extended hour: Men: −4.9% Women: 3.8% |
| Bruce (1980)38 Design suitability: Least Before and after study with no comparison Quality of execution: Fair (2 limitations) |
Location: 4 major cities and central belt of Scotland Dates: Intervention: Hours: December 13, 1976 Pre-intervention: October–November 1976 Follow-up: March 1977 |
Intervention: Hours: Evening closing hours extended from 10:00PM to 11:00PM in December 1977 (Sunday licenses issued October 1977) Control: No comparison group |
Analysis: Percentage changes Outcomes: Beer sales in bulk barrels |
Beer sales in bulk barrels Mean 1970–1976/1977 3,7856,143/40,262,000 3,264,000/366,800 |
Relative % change: Beer sales in bulk barrels 5.7% |
| De Moira (1995)39 Duffy (1996)40 Design suitability: Greatest Prospective data collection with intervention and control populations Quality of execution: Fair (2 limitations) |
Location: England/Wales Dates: Intervention: August 1988 Pre-intervention: 1980–1988 Follow-up: 1988–1991 |
Intervention: Extension of opening and Sunday hours
Control: Scotland (positive control, having already extended hours several years previously) |
Analysis: Logistic linear regression, analysis of deviance Outcomes:
|
Summary of major findings: Mortality: No increase in:
Workplace: No increase in:
Increase in:
RR Scotland: 1.34 RR E and E: 1.01 Motor vehicle: No increase in:
Increase in:
Relative % change: 3.5% Public order: No increase in:
|
Relative % changes (95% CI): Mortality from diverse alcohol-related diseases: no effect Convictions for sales to underage patrons: 64.1% (21.2%, 99.0%) Purchases by minors: −62.4% (72.9%, 46.5%) Recorded violent crime: 15.5% (14.0%, 17.0%) |
| Vingilis (2005)41 Design suitability: Greatest Prospective data collection with intervention and control populations Quality of execution: Fair (3 limitations) |
Intervention: May 1996 Pre-intervention: 1992–1996 Follow-up: 1996–1999 |
Intervention: On May 1, 1996, Ontario, Canada, amended the Liquor License Act to extended closing hours for alcohol sales and service in licensed establishments from 1:00AM to 2:00AM Control: Michigan and New York states, in which similar changes did not occur |
Analysis: Supposedly interrupted time series, but results not given. Graphical analyses. Outcomes: Motor vehicle fatalities, alcohol-related and all Consumption |
Summary of major findings: No significant change relative to controls Declines in consumption reported |
Findings: No significant change relative to controls |
Cls not calculable due to the lack of data.
ARMT, alcohol-related maxillofacial trauma; ETP, extended trading permit
Four of the six events studied occurred in Australia (in 1966, 1977, 1984, and 1998–2000); one in London, England (in 2005); and one in Reykjavik, Iceland (in 2005). All of the events led to increased hours of sale at on-premises alcohol outlets.
In Victoria, Australia, weekday and Saturday hours were extended from 6:00 PM to 10:00 PM in 1966. Hours allowed prior to this change were not reported. One study22 compared trends in motor vehicle–related outcomes on weekdays and Saturdays before and after the hours of alcohol sales at on-premises alcohol outlets in Victoria, Australia, were extended, to the same outcomes on Sundays, when there was no change in hours. The author found that the increase in hours of sales on weekdays and Saturday did not significantly affect the number of crashes that occurred on these days. However, she observed a change in the timing of crashes corresponding to the change in the closing time of the on-premises alcohol outlets. Thus, in this study, it appeared that although the number of events may not have been affected by the change in the closing time of alcohol outlets, their timing was affected. In contrast to this study’s findings, two subsequent analyses of the same event concluded that the increase in hours was associated with increases in consumption23 and motor vehicle crash injuries.24
In 1984, hours available for alcohol service in Victoria were extended from 10:00PM until 12:00MN on weekdays and Saturdays and in length of time open from 4 hours to 8 hours on Sundays (a day on which alcohol sales had been previously allowed). Information on hours prior to the weekday and Saturday extension is not given. A study of this event30 found an increase in motor vehicle crash injuries associated with these increases in hours.
Between July 1998 and June 2000, Victoria granted 24-hour permits to some on-premises alcohol outlets. A cross-sectional study comparing rates of assaults in outlets granted and not granted 24-hour permits is inconclusive.31 Although authors claim that higher rates of assault are associated with 24-hour facilities, their statements describing results are inconsistent, and the authors do not provide data to allow re-evaluation.
In Tasmania (Australia), licensed premises were allowed to stay open until any hour in 1977. Prior Monday–Saturday opening hours were 10:00AM–10:00PM; Sunday hours, 12NOON–8:00PM. The assumption by policymakers underlying unrestricted closing times was that possibly intoxicated clients would not be exiting the facilities at the same time, potentially decreasing risks, because different outlets would choose different closing hours. A study of this event25 found an increase in motor vehicle crash injuries associated with these increases in hours.
In Reykjavik, licensed premises were allowed to stay open until any hour in the year 1999 on an experimental basis. Prior closing requirements were 11:30 PM on weekdays and 2:00 AM on weekends. Researchers found increases in emergency room admissions, injuries, fighting, and suspected driving while intoxicated.26
Finally, the United Kingdom’s Licensing Act of 2003 allowed sales of alcoholic beverages 24 hours a day in England and Wales, beginning in November 2005, subject to local licensing requirements. Three studies assessing the impact of this increase in hours of sale produced mixed results.27–29 Two studies28,29 found a relative decrease in harms (violent criminal offenses and alcohol-related maxillofacial trauma, respectively), whereas a third study27 found a relative increase in harms (alcohol-related assault and injury) subsequent to this increase in hours of sale.
Among the ten studies in this body of evidence,22–31 two studies28,29 found that an increase of ≥2 hours in the hours of sale led to decreased alcohol-related harms (i.e., injury and serious violent crime), and six studies23–27,30 found an increase in alcohol-related harms relative to the period before the increase in hours of sale took place (Figure 2). The study by Raymond22 found no effect. One study23 found a nonsignificant increase in alcohol consumption associated with the increase in hours in Victoria, Australia, in 1966.
Figure 2.

Relative percentage change in diverse outcomes associated with increases of ≥2 hours
DUI, driving under the influence
Information on the requirement that premises seek permits prior to expanding hours may not have been complete in the studies reviewed. To the extent that stated permit requirements accurately reflect the expansion process, there appears to be no systematic effect of permitting. Although the harmful effects of permitted expansions appear to be larger than those in which permits were not required (Figure 2) there were also effects in the opposite direction for studies of permitted settings.
Studies of Changes of <2 Hours in Hours of Sale
Six studies of five events (reported in ten papers32–41) that resulted in a change of <2 hours of sale met the inclusion criteria. All studies were of on-premises alcohol outlets. Three studies (seven papers32–35,39–41) were of greatest design suitability, three36–38 were of least suitable design; all were of fair quality of execution. One study (two papers39,40) of the extension of opening hours in England and Wales in 1988 did not allow the calculation of effects for several outcomes, but it reported small and inconsistent results on multiple alcohol-related outcomes. One41 provides graphics and report using interrupted time series but does not report numeric results.
In 1993, Perth, Australia allowed on-premises outlets to extend their closing time from 12:00MN to 1:00AM.32–35 Findings were inconsistent, with a reported increase of alcohol wholesale but a decline in drunk driving and an increase in assaults and in alcohol-related crashes. None of these findings was significant.
In December 1979, the state of New South Wales in Australia expanded on-premises alcohol outlet closing hours from 10:00PM to 11:00PM, at the same time expanding Sunday hours and outlet settings. A study of these events36 proposed using the weekdays as the control in an assessment of the effects of increased Sunday sales on motor vehicle fatalities. However, this comparison is biased toward a null effect, given the change in weekday hours. A comparison of weekday fatalities before and after the weekday expansion indicates a reduction of 2.7% in motor vehicle fatalities over the study period associated with the weekday increase of 1 hour in closing time. However, this outcome may be confounded by a reduction from 0.08% to 0.05% in maximum legal blood alcohol levels in December 1980, which would have been expected to deter drunk driving and reduce motor vehicle injuries.
In 1976, Scotland allowed on-premises outlets to extend their closing time from 10:00PM to 11:00PM.37,38 Reported changes were small and not consistent in direction. Knight found increased consumption for women and decreased consumption for men, and Bruce reported a small increase in the per capita consumption of beer.
In 1988, England and Wales extended the closing hours at on-premises outlets from 10:30PM to11:00PM and moved the opening time from 11:00AM to 10:00AM.39,40 The outcomes, including mortality from liver disease and cirrhosis, pancreatitis, alcohol poisoning, “alcohol-dependent syndrome,” alcohol psychosis, workplace absenteeism and injury, and various motor vehicle–related outcomes) assessed in these studies were heterogeneous and included the seemingly contradictory findings that in comparison with changes in the control setting (Scotland), convictions for sales to underage patrons increased by 64.1% (95% CI=21.2%, 99.0%), whereas sales to minors fell substantially. Another finding was an increase in recorded violent crime of 15.5% (95% CI= 14.0%, 17.0%). (See Table 1.)
Finally, in 1996, Ontario Province extended closing hours in on-premises alcohol outlets from 1:00AM to 2:00AM. A study41 of this event used graphics and interrupted time series to assess the effects of this change on all and alcohol-related fatal motor vehicle crashes. Changes in Ontario were compared with changes in Michigan and New York, neither of which changed hours of sale during the same period. The study also assessed changes in the sales of beer, wine, and spirits in Ontario from the period before to the period following the policy change. Numeric results are not reported. Beer consumption declined over the study period, whereas the consumption of wine and spirits declined in the early 1990s and then increased in the later 1990s. The authors conclude that changes in motor vehicle outcomes are “minimal.” Their graphics suggest a shift of the timing of alcohol-related fatalities to later hours following the extension of hours of sale.
This small body of evidence indicates no consistent effects of changes of <2 hours on alcohol-related outcomes. Four events of increases in hours of sale were studied. Only one study of increased hours of sale in Perth, Australia, reported substantial increases in wholesale alcohol purchases, assaults, and motor vehicle crashes. Two studies (of events in England and Wales and in Ontario, Canada) did not provide numeric results but reported small and inconsistent changes in alcohol-related outcomes including alcohol consumption, multiple alcohol-related causes of mortality, and motor vehicle crashes. Two studies of increased hours of sale in Scotland also reported small and inconsistent changes in alcohol sales and consumption.
Again, information on the requirement that premises seek permits prior to expanding hours may not have been complete in the studies reviewed. To the extent that stated permit requirements accurately reflect the expansion process, there appears to be no systematic effect of permitting (Figure 3).
Figure 3.

Relative percentage change in diverse outcomes associated with increases of <2 hours
NSW, New South Wales
Applicability
The studies in this review were conducted in a variety of settings outside the U.S. and during a wide range of time periods. None-theless, the association between restrictions on the hours when alcohol may be sold and alcohol-related harms was consistent across most geographic locations (all in high-income countries) and time periods, and the findings of this review are likely to be relevant for considering the potential impact of modifying the number of hours when alcohol may be sold in the U.S.
Other Harms and Benefits
Maintaining hours of sale may sustain quality of life in communities by controlling alcohol availability, excessive alcohol consumption, and health and social harms resulting from excessive alcohol use (e.g., public drunkenness); evidence of effects on quality of life were not provided by the studies reviewed. Although it is possible that crimes such as illicit alcohol sales may increase in localities where the hours of sale are limited, no evidence of such effects was found in any of the studies evaluated. One study26 noted increased workload among law enforcement personnel associated with expanded hours of sale.
Barriers
The maintenance and reduction in the number of hours when alcohol may be sold may affect overall alcohol sales and may thus be opposed by commercial interests involved in manufacture, distribution, and sale of alcoholic beverages. The alcohol industry has generally supported policies that remove restrictions on the access to alcohol.42
State pre-emption laws (i.e., state laws that prevent the implementation and enforcement of local policies more restrictive than statewide regulations) can also undermine efforts by local governments to regulate hours of sale.6 Indeed, the elimination of pre-emption laws related to the sale of tobacco products is one of the health promotion objectives in Healthy People 2010.5 However, there is no similar objective in Healthy People 2010 related to the local sale of alcoholic beverages.
Economics
No studies were identified that assessed the economic impact of reducing the number of hours when alcohol may be sold. No study was found that specifically estimated the magnitude of commercial losses in sales and tax revenues because of a policy of restricting hours of alcohol sales.
Summary
This review found that increasing the hours when alcohol may be sold by ≥2 hours increased alcohol-related harms. Evidence supporting this conclusion was based on studies conducted in on-premises settings outside the U.S. According to Community Guide rules of evidence, these findings provided sufficient evidence for the effectiveness of maintaining limits on hours of sale for the reduction of alcohol-related harms when efforts are made to increase hours by ≥2.10 Because no qualifying study assessed the effects of reducing hours of sale, the only direct inference that can be made is that reducing hours of sale by ≥2 is likely to avert alcohol-related harms. However, it may also be reasonable to expect that reducing hours of sale would also reduce alcohol-related harms.
Because there was no consistent effect on excessive alcohol consumption or related harms of increasing hours of sales by <2 hours, according to Community Guide rules of evidence, there was insufficient evidence that this intervention had a meaningful effect.10 Insufficient evidence means that it is not possible to determine from the available evidence whether this policy change had a meaningful effect.
Research Gaps
All existing research on hours of sale to date has been conducted in nations other than the U.S. It would be useful to have studies of changes in hours of sale in U.S. settings to confirm results from other settings. In addition, all research thus far has assessed the effects of increasing hours of sale. Although it may be a less-frequent event, evaluating the effects of reducing hours of sale for preventing excessive alcohol consumption and related harms would be useful. Evidence on changes in hours of sale of <2 hours is currently insufficient because of inconsistent findings. Thus, when such changes occur, it may be worthwhile to assess the effects of smaller changes in hours of sale on excessive alcohol consumption and related harms to improve our understanding of the “dose–response” and “threshold” relationships between changes in hours of sale and public health outcomes.
Additional research is also needed to more fully assess the costs and benefits of restricting the number of hours when alcohol is sold. From a societal perspective, economic elements should include intervention costs; loss in sales, tax revenues, and employment; reductions in fatal and nonfatal injuries, crime, and violence; gains in safety and public order; and averted loss of household and workplace productivity.
Finally, no studies were found that assessed the effects of changes in hours of sale in off-premises settings. Although consumers at off-premises settings are less likely to be directly affected by the effects of excessive consumption at the place of purchase, it is nevertheless possible that changes in availability in these settings may also affect alcohol-related harms. This issue merits investigation.
Discussion
Based on a systematic review of qualifying studies, this review confirms the findings of previous reviews and adds details regarding a possible dose or threshold effect. Evidence of the effects of changes in hours of sale of <2 hours was insufficient to determine effectiveness because of inconsistency among findings in the body of evidence, leaving unanswered the question of the effects of small increases in hours of sale. Data are not sufficient to allow systematic assessment of the relative percentage increase in hours (over a baseline) or the placement of the hours within the day.
All of the studies included in this review assessed the effects of increasing hours of sale at on-premises outlets, consistent with the international trend toward expanding the availability of alcoholic beverages. Further scientific evidence is needed to fully assess the symmetry between the effects of maintaining existing limits on the hours of sale compared with reducing hours of sale.
The only available evidence of the effects of reducing hours of sale was from a study in Brazil,43 which did not qualify for inclusion in the review because Brazil is not a high-income nation, and, in general, studies of alcohol consumption from middle- and lower-income nations are thought not to be directly applicable to the contemporary U.S. context. In 1999, the city of Diadema had very high homicide rates; 65% of these were alcohol-related. Most of the homicides occurred between 11:00PM and 6:00AM. Diadema law allowed 24-hour opening of alcohol outlets. In July 2002, a new city law required bars to close at 11:00PM. From 2002 to 2005, homicide rates in the city declined by 44% (95% CI=27%, 61%), controlling for mortality trends. During this time period, there was also a 17% decline in assaults against women (the only additional outcome assessed); this finding, however, was not significant.
In addition to the lack of studies that assessed the effect of stricter limits on the hours when alcohol may be sold, the body of qualifying studies in this review had several other limitations. First, some studies did not directly assess the impact of relaxing restrictions on the hours of sales on excessive alcohol consumption and alcohol-related harms, but rather relied on proxy measures of these effect outcomes (e.g., criminal arrest rates). Second, nearly all of the studies relied on population-based data from public health surveillance systems that did not capture information on alcohol control policies. As a result, many of these studies were unable to control for some potential confounding factors. However, these studies generally assessed changes in the same geographic area before and after the implementation of changes in hours of sale over a fairly short time period. Other contextual factors that could also influence alcohol sales and consumption (e.g., changes in alcohol excise taxes) at the country, state, or community levels were likely to have remained fairly constant during the study periods, allowing for a valid assessment of the impact of changing hours of sale, independent of other factors, on alcohol-related harms.
The findings in this review support the potential value of allowing local communities to maintain restrictions on hours of sale. If further research supports the effectiveness of local restrictions on hours of sale, it would also argue for eliminating state pre-emption laws that prohibit local governments from enacting alcohol control policies more restrictive than those that exist statewide.
Acknowledgments
We acknowledge the support and contributions of Steven Wing of the Substance Abuse and Mental Health Services Administration (SAMHSA) in discussions of this and other reviews.
Footnotes
World Bank High-Income Economies (as of May 5, 2009): Andorra, Antigua and Barbuda, Aruba, Australia, Austria, The Bahamas, Bahrain, Barbados, Belgium, Bermuda, Brunei Darussalam, Canada, Cayman Islands, Channel Islands, Cyprus, Czech Republic, Denmark, Equatorial Guinea, Estonia, Faeroe Islands, Finland, France, French Polynesia, Germany, Greece, Greenland, Guam, Hong Kong (China), Hungary, Iceland, Ireland, Isle of Man, Israel, Italy, Japan, Republic of Korea, Kuwait, Liechtenstein, Luxembourg, Macao (China), Malta, Monaco, Netherlands, Netherlands Antilles, New Caledonia, New Zealand, Northern Mariana Islands, Norway, Oman, Portugal, Puerto Rico, Qatar, San Marino, Saudi Arabia, Singapore, Slovak Republic, Slovenia, Spain, Sweden, Switzerland, Trinidad and Tobago, United Arab Emirates, United Kingdom, U.S., Virgin Islands (U.S.).
The names and affiliations of the Task Force members are listed at www.thecommunityguide.org/about/task-force-members.html.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
No financial disclosures were reported by the authors of this paper.
References
- 1.CDC. Alcohol-attributable deaths and years of potential life lost—U.S. 2001. MMWR Morb Mortal Wkly Rep. 2004;53(37):866–70. [PubMed] [Google Scholar]
- 2.National Center for Health Statistics. Health, U.S., 2005 with chart-book on trends in the health of America. Hyattsville MD: NCHS; 2005. Report No.: 1232. [Google Scholar]
- 3.Miller JW, Naimi TS, Brewer RD, Jones SE. Binge drinking and associated health risk behaviors among high school students. Pediatrics. 2007;119(1):76–85. doi: 10.1542/peds.2006-1517. [DOI] [PubMed] [Google Scholar]
- 4.Harwood H. Report prepared by The Lewin Group for the National Institute on Alcohol Abuse and Alcoholism. Rockville MD: NIAAA; 2000. Updating estimates of the economic costs of alcohol abuse in the U.S.: estimates, update methods, and data. Report No.: 98-4327. [Google Scholar]
- 5.USDHHS. Healthy People. 2010 www.healthypeople.gov/
- 6.Mosher J. Alcohol issues policy briefing paper: the perils of preemption. Chicago: American Medical Association; 2001. [Google Scholar]
- 7.Gorovitz E, Mosher J, Pertschuk M. Preemption or prevention? Lessons from efforts to control firearms, alcohol, and tobacco. J Public Health Policy. 1998;19(1):36–50. [PubMed] [Google Scholar]
- 8.Pub. L. No. 83-277, 67 Stat. 586 (1983).1983.
- 9.Wikipedia.org. Alcohol laws of the U.S. by state. en.wikipedia.org/wiki/Alcohol_laws_of_the_United_States_by_state.
- 10.Briss PA, Zaza S, Pappaioanou M, et al. Developing an evidence-based Guide to Community Preventive Service—methods. Am J Prev Med. 2000;18(1S):35–43. doi: 10.1016/s0749-3797(99)00119-1. [DOI] [PubMed] [Google Scholar]
- 11.Grover PL, Bozzo R. Preventing problems related to alcohol availability: environmental approaches. DHHS, SAMHSA, CSAP; 1999. [Google Scholar]
- 12.Stockwell T, Gruenewald P. Controls on the physical availability of alcohol. In: Heather N, Peters TJ, Stockwell T, editors. International handbook of alcohol dependence and problems. Chichester, UK: Wiley; 2004. pp. 699–719. [Google Scholar]
- 13.Smith DI. Effectiveness of restrictions on availability as a means of preventing alcohol-related problems. Contemp Drug Prob. 1988:627–84. [Google Scholar]
- 14.Popova S, Giesbrect N, Bekmuradov D, Patra J. Hours and days of sale and density of alcohol outlets: impacts on alcohol consumption and damage: a systematic review. Alcohol Alcohol. 2009;44:500–16. doi: 10.1093/alcalc/agp054. [DOI] [PubMed] [Google Scholar]
- 15.Babor TF, Caetano R, Casswell S, et al. Alcohol: no ordinary commodity-research and public policy, 2nd edition. Oxford, UK: Oxford University Press; 2010. [Google Scholar]
- 16.WHO. Evidence for the effectiveness and cost-effectiveness of interventions to reduce alcohol-related harm. Copenhagen, Denmark: WHO Regional Office for Europe; 2009. www.euro.who.int/__data/assets/pdf_file/0020/43319/E92823.pdf. [Google Scholar]
- 17.Strategic Task Force on Alcohol. Strategic Task Force on Alcohol—second report. Ireland: Health Promotion Unit, Department of Health and Children; 2004. [Google Scholar]
- 18.Lipsey MW, Wilson DB, Cohen MA, Derzon JH. Is there a causal relationship between alcohol use and violence? In: Galanter M, editor. Recent developments in alcoholism: volume 13, alcohol and violence. New York: Plenum Press; 1997. pp. 245–82. [DOI] [PubMed] [Google Scholar]
- 19.World Bank. World development indicators 2006. 2006 devdata.worldbank.org/wdi2006/contents/cover.htm.
- 20.Gruenewald PJ, Millar AB, Treno AJ, Yang Z, Ponicki WR, Roeper P. The geography of availability and driving after drinking. Addiction. 1996;91(7):967–83. doi: 10.1046/j.1360-0443.1996.9179674.x. [DOI] [PubMed] [Google Scholar]
- 21.Cook PJ, Skog OJ. Alcool, alcoolisme, alcoolisation—comment. Alcohol Health Res World. 1995;19(1):30–1. [PMC free article] [PubMed] [Google Scholar]
- 22.Raymond A. Ten o’clock closing—the effect of the change in hotel bar closing time on road accidents in the metropolitan area of Victoria. Aust Road Res. 1969;3(10):3–17. [Google Scholar]
- 23.Williams RA. Changes in trading hours: ten o’clock closing and consumption of alcohol in Victoria. Econ Record. 1972;48:123–7. [Google Scholar]
- 24.Smith DI. Effect on casualty traffic accidents of the introduction of 10 p.m. Monday to Saturday hotel closing in Victoria. Aust Drug Alcohol Rev. 1988;7:163–6. [Google Scholar]
- 25.Smith DI. Effect on traffic accidents of introducing flexible hotel trading hours in Tasmania, Australia. Br J Addict. 1988;83:219–22. doi: 10.1111/j.1360-0443.1988.tb03984.x. [DOI] [PubMed] [Google Scholar]
- 26.Ragnarsdottir T, Kjartansdottir A, Davidsdottier S. Effect of extended alcohol serving hours in Reykjavik, Iceland. In: Room R, editor. The effects of Nordic alcohol policies. Helsinki, Finland: Nordic Council for Alcohol and Drug Research; 2002. pp. 145–54. [Google Scholar]
- 27.Newton A, Sarker SJ, Pahal GS, van den Bergh E, Young C. Impact of the new UK licensing law on emergency hospital attendances: a cohort study. Emerg Med J. 2007;24:532–4. doi: 10.1136/emj.2007.046094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Babb P. Home Office Online Report 16/07. 2007. Violent crime, disorder and criminal damage since the introduction of the Licensing Act 2003. [Google Scholar]
- 29.El-Maaytah M, Smith S, Jerjes W, et al. The effect of the new “24 hour alcohol licensing law” on the incidence of facial trauma in London. Br J Oral Maxillofac Surg. 2008;46(6):460–3. doi: 10.1016/j.bjoms.2008.01.018. [DOI] [PubMed] [Google Scholar]
- 30.Smith DI. Effect on casualty traffic accidents of changing Sunday alcohol sales legislation in Victoria, Australia. J Drug Issues. 1990;20(3):417–26. [Google Scholar]
- 31.Briscoe S, Donnelly N. Problematic licensed premises for assault in inner Sydney, Newcastle and Wollongong. Aust N Z J Criminol. 2003;36(1):18–33. [Google Scholar]
- 32.Chikritzhs T, Stockwell T, Masters L. Evaluation of the public health and safety impact of extended trading permits for Perth hotels and nightclubs. Perth: National Drug Institute; 1997. [Google Scholar]
- 33.Chikritzhs T, Stockwell T. The impact of later trading hours for Australian public houses (hotels) on levels of violence. J Stud Alcohol. 2002;63(5):591–9. doi: 10.15288/jsa.2002.63.591. [DOI] [PubMed] [Google Scholar]
- 34.Chikritzhs T, Stockwell T. The impact of later trading hours for hotels on levels of impaired driver road crashes and driver breath alcohol levels. Addiction. 2006;101(9):1254–64. doi: 10.1111/j.1360-0443.2006.01487.x. [DOI] [PubMed] [Google Scholar]
- 35.Chikritzhs T, Stockwell T. The impact of later trading hours for hotels (public houses) on breath alcohol levels of apprehended impaired drivers. Addiction. 2007;102(10):1609–17. doi: 10.1111/j.1360-0443.2007.01981.x. [DOI] [PubMed] [Google Scholar]
- 36.Smith DI. Effect on traffic accidents of introducing Sunday hotel sales in New South Wales, Australia. Contemp Drug Prob. 1987;14:279–94. [Google Scholar]
- 37.Knight I, Wilson P. Scottish licensing laws. London: Office of Population Censuses and Surveys, Social Survey Division; 1980. [Google Scholar]
- 38.Bruce D. Changes in Scottish drinking habits and behaviour following the extension of permitted evening opening hours. Health Bull. 1980;38(3):133–7. [PubMed] [Google Scholar]
- 39.De Moira ACP, Duffy JC. Changes in licensing law in England and Wales and alcohol-related mortality. Addiction Res. 1995;3(2):151–64. [Google Scholar]
- 40.Duffy JC, De Moira ACP. Changes in licensing law in England and Wales and indicators of alcohol-related problems. Addiction Res. 1996;4(3):245–71. [Google Scholar]
- 41.Vingilis E, McLeod AI, Seeley J, Mann RE, Beirness D, Compton CP. Road safety impact of extended drinking hours in Ontario. Accid Anal Prev. 2005;37(3):549–56. doi: 10.1016/j.aap.2004.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Giesbrecht N. Roles of commercial interests in alcohol policies: recent developments in North America. Addiction. 2000;95(4):S581–95. doi: 10.1080/09652140020013791. [DOI] [PubMed] [Google Scholar]
- 43.Duailibi S, Ponicki W, Grube J, Pinsky I, Laranjeira R, Raw M. The effect of restricting opening hours on alcohol-related violence. Am J Public Health. 2007;97(12):2276–80. doi: 10.2105/AJPH.2006.092684. [DOI] [PMC free article] [PubMed] [Google Scholar]