

Abstract
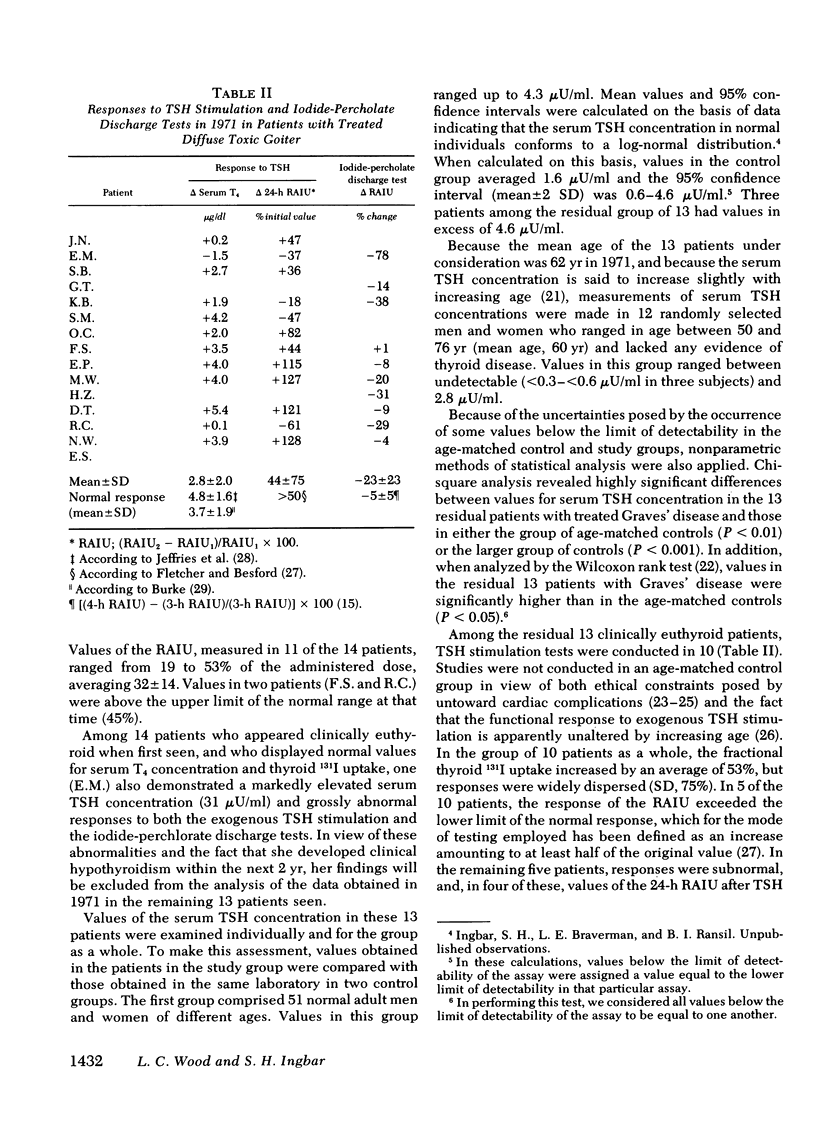
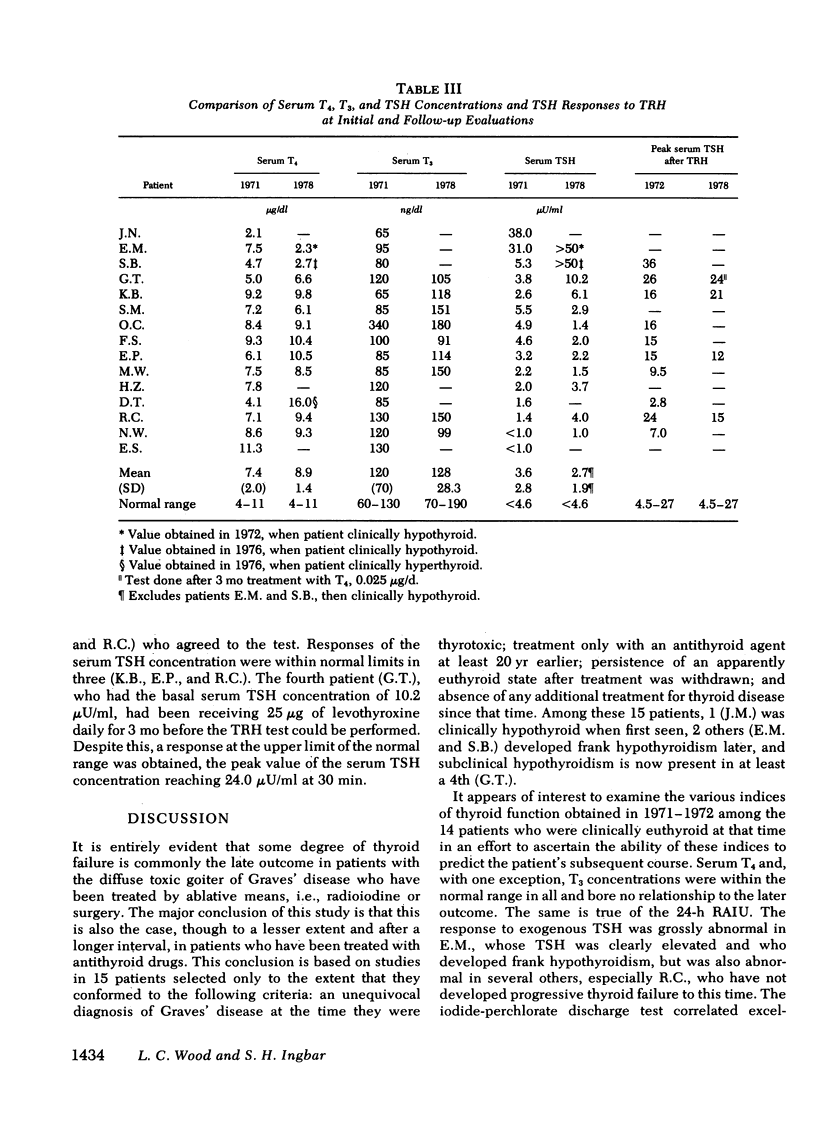
In 1971, thyroid function was evaluated in 15 unselected patients whose only therapy for diffuse toxic goiter was a course of thionamide drug treatment completed 20-27 yr earlier. One patient was frankly hypothyroid by clinical and laboratory criteria. The remaining 14 patients appeared clinically euthyroid and had a normal serum thyroxine (T4) concentration and thyroid radioiodine uptake (RAIU). Nevertheless, only 6 of 14 appeared to be entirely normal according to more refined criteria. The serum thyrotropin (TSH) concentration was markedly elevated in one patient and above the normal range (1.6±2.0; mean±2 SD) in five others. Thyroid stimulation with exogenous TSH revealed subnormal responses of the serum T4I, RAIU, or both, in 7 of 11 patients tested. An abnormal iodideperchlorate discharge test was found in 5 of 10 patients and appeared most abnormal in patients with abnormal RAIU responses to TSH. Fluorescent antimicrosomal antibody was found in the serum of 12 of the 15 patients, in contrast to an expected frequency of 7% in normal individuals of the same age.
By the time a second major follow-up study was completed in 1978, two additional patients had become frankly hypothyroid. A third subject met accepted criteria for subclinical hypothyroidism. One of these subjects had had a clearly elevated serum TSH concentration in 1972, and the remaining two had exhibited the highest responses of serum TSH (36, 26 μU/ml) to thyrotropin-releasing hormone among 10 patients tested in 1972.
One patient developed recurrent thyrotoxicosis in 1978, 25 yr after the onset of his first and only other apparent episode of hyperthyroidism. This patient was the only one who demonstrated a subnormal response to thyrotropin-releasing hormone in 1972. The remaining nine subjects that could be studied in 1978 exhibited varying combinations of abnormalities of thyroid function.
It is concluded that progressive failure of thyroid function is a common occurence in long-standing Graves' disease, and it is suggested that this results from concomitant chronic thyroiditis. We postulate that this inherent tendency toward thyroid failure is exaggerated by surgery or radioactive iodine, explaining the progressive increase in, and inordinate frequency of, hypothyroidism after ablative modes of therapy in diffuse toxic goiter.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ASPENSTROM G. Late results with propylthiouracil treatment of hyperthyroidism in a goiter region. Acta Med Scand. 1953;147(1):63–70. [PubMed] [Google Scholar]
- BAKER S. P., GAFFNEY G. W., SHOCK N. W., LANDOWNE M. Physiological responses of five middle-aged and elderly men to repeated administration of thyroid stimulating hormone (thyrotropin; TSH). J Gerontol. 1959 Jan;14(1):37–47. doi: 10.1093/geronj/14.1.37. [DOI] [PubMed] [Google Scholar]
- BAKER S. P., LANDOWNE M., GAFFNEY G. W. Electrocardiographic changes following the administration of thyroid stimulating hormone (thyrotropin). Am J Cardiol. 1960 Nov;6:905–914. doi: 10.1016/0002-9149(60)90290-3. [DOI] [PubMed] [Google Scholar]
- Bode H. H., Danon M., Weintraub B. D., Maloof F., Crawford J. D. Partial target organ resistance to thyroid hormone. J Clin Invest. 1973 Apr;52(4):776–782. doi: 10.1172/JCI107240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braverman L. E., Vagenakis A. G., Foster A. E., Ingbar S. H. Evaluation of a simplified technique for the specific measurement of serum thyroxine concentration. J Clin Endocrinol Metab. 1971 Apr;32(4):497–502. doi: 10.1210/jcem-32-4-497. [DOI] [PubMed] [Google Scholar]
- Braverman L. E., Vagenakis A. G., Wang C. A., Maloof F., Ingbar S. H. Studies on the pathogenesis of iodide myxedema. Trans Assoc Am Physicians. 1971;84:130–138. [PubMed] [Google Scholar]
- Burke G. The thyrotrophin stimulation test. Ann Intern Med. 1968 Dec;69(6):1127–1139. doi: 10.7326/0003-4819-69-6-1127. [DOI] [PubMed] [Google Scholar]
- COOPER G. W., JEFFERIES W. M., KELLY L. W., Jr, LEVY R. P., PROUTY R. L. The significance of low thyroid reserve. J Clin Endocrinol Metab. 1956 Nov;16(11):1438–1455. doi: 10.1210/jcem-16-11-1438. [DOI] [PubMed] [Google Scholar]
- Cuttelod S., Lemarchand-Béraud T., Magnenat P., Perret C., Poli S., Vannotti A. Effect of age and role of kidneys and liver on thyrotropin turnover in man. Metabolism. 1974 Feb;23(2):101–113. doi: 10.1016/0026-0495(74)90107-3. [DOI] [PubMed] [Google Scholar]
- DOUGLAS D., KENNIE A. T. Thiouracil in toxic goitre; late results in a personal series. Br Med J. 1952 Dec 27;2(4799):1387–1391. doi: 10.1136/bmj.2.4799.1387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DUNN J. T., CHAPMAN E. M. RISING INCIDENCE OF HYPOTHYROIDISM AFTER RADIOACTIVE-IODINE THERAPY IN THYROTOXICOSIS. N Engl J Med. 1964 Nov 12;271:1037–1042. doi: 10.1056/NEJM196411122712004. [DOI] [PubMed] [Google Scholar]
- Dickson J. A., Fraser G. C. "Swallowed" endotracheal tube: a new neonatal emergency. Br Med J. 1967 Jun 24;2(5555):811–812. doi: 10.1136/bmj.2.5555.811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FLETCHER R. F., BESFORD H. A test of thyroid and pituitary function using thyrotrophin. Clin Sci. 1958 Feb;17(1):113–120. [PubMed] [Google Scholar]
- Furth E. D., Rathbun M., Posillico J. A modified bioassay for the long-acting thyroid stimulator (LATS). Endocrinology. 1969 Sep;85(3):592–593. doi: 10.1210/endo-85-3-592. [DOI] [PubMed] [Google Scholar]
- GOODWIN J. F., STEINBERG H., WILSON A. Long-term therapy of thyrotoxicosis with thiouracil compounds. Br Med J. 1954 Feb 20;1(4859):422–425. doi: 10.1136/bmj.1.4859.422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gautvik K. M., Tashjian A. H., Jr, Kourides I. A., Weintraub B. D., Graeber C. T., Maloof F., Suzuki K., Zuckerman J. E. Thyrotropin-releasing hormone is not the sole physiologic mediator of prolactin release during suckling. N Engl J Med. 1974 May 23;290(21):1162–1165. doi: 10.1056/NEJM197405232902103. [DOI] [PubMed] [Google Scholar]
- Hershman J. M., Givens J. R., Cassidy C. E., Astwood E. B. Long-term outcome of hyperthyroidism treated with antithyroid drugs. J Clin Endocrinol Metab. 1966 Aug;26(8):803–807. doi: 10.1210/jcem-26-8-803. [DOI] [PubMed] [Google Scholar]
- MANSON D. I. Late results of treatment of thyrotoxicosis with thiouracil compounds. Edinb Med J. 1953 Jul;60(7):321–330. [PMC free article] [PubMed] [Google Scholar]
- McCULLAGH E. P., CASSIDY C. E. Propylthiouracil: 4-6 year follow-up of selected patients with Graves' disease. J Clin Endocrinol Metab. 1953 Dec;13(12):1507–1512. doi: 10.1210/jcem-13-12-1507. [DOI] [PubMed] [Google Scholar]
- Nofal M. M., Beierwaltes W. H., Patno M. E. Treatment of hyperthyroidism with sodium iodide I-131. JAMA. 1966 Aug 22;197(8):605–610. [PubMed] [Google Scholar]
- Palmer K. T. A prospective study into thyroid disease in a geriatric unit. N Z Med J. 1977 Oct 12;86(597):323–324. [PubMed] [Google Scholar]
- SOLOMON D. H., BECK J. C., VANDERLAAN W. P. Prognosis of hyperthyroidism treated by antithyroid drugs. J Am Med Assoc. 1953 May 16;152(3):201–205. doi: 10.1001/jama.1953.03690030001001. [DOI] [PubMed] [Google Scholar]
- Snyder P. J., Utiger R. D. Response to thyrotropin releasing hormone (TRH) in normal man. J Clin Endocrinol Metab. 1972 Feb;34(2):380–385. doi: 10.1210/jcem-34-2-380. [DOI] [PubMed] [Google Scholar]
- TAUNTON O. D., MCDANIEL H. G., PITTMAN J. A., Jr STANDARDIZATION OF TSH TESTING. J Clin Endocrinol Metab. 1965 Feb;25:266–277. doi: 10.1210/jcem-25-2-266. [DOI] [PubMed] [Google Scholar]
- TROTTER W. R. Nonsurgical treatment of thyrotoxicosis. Proc R Soc Med. 1961 Oct;54:869–871. [PubMed] [Google Scholar]
- Vallotton M. B., Pretell J. Y., Forbes A. P. Distinction between idiopathic primary myxedema and secondary pituitary hypothyroidism by the presence of circulating thyroid antibodies. J Clin Endocrinol Metab. 1967 Jan;27(1):1–10. doi: 10.1210/jcem-27-1-1. [DOI] [PubMed] [Google Scholar]
- Van Welsum M., Feltkamp T. E., De Vries M. J., Doctor R., Van Zijl J., Hennemann G. Hypothyroidism after thyroidectomy for Graves's disease: a search for an explanation. Br Med J. 1974 Dec 28;4(5947):755–756. doi: 10.1136/bmj.4.5947.755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WILLCOX P. H. Twelve years' experience of antithyroid treatment. Postgrad Med J. 1962 May;38:275–280. doi: 10.1136/pgmj.38.439.275. [DOI] [PMC free article] [PubMed] [Google Scholar]