

Abstract
Objective
There are increasing global concerns about improving the dietary intakes of children and adolescents. In the United States (U.S.) the focus is on reducing energy from foods and beverages that provide empty calories from solid fats and added sugars (SoFAS). We examine trends in intakes and sources of solid fat and added sugars among U.S. 2- to 18- year olds from 1994-2010.
Methods
Data from five nationally representative surveys, the Continuing Survey of Food Intakes by Individuals Surveys (1994-1996) and the What We Eat In America, National Health and Nutrition Examination Surveys (2003-2004, 2005-2006, 2007-2008 and 2009-2010) were used to examine key food sources and energy from solid fats and added sugars. Sample sizes ranged from 2,594 to 8,259 per survey period, for a total of 17,268 observations across the five surveys. Food files were linked over time to create comparable food groups and nutrient values. Differences were examined by age, race/ethnicity and family income.
Results
Daily intake of energy from SoFAS among U.S. 2-18 year olds decreased from 1994-2010, with declines primarily detected in the recent time periods. Solid fats accounted for a greater proportion of total energy intake than did added sugars.
Conclusions
Although the consumption of solid fats and added sugars among children and adolescents in the United States decreased between 1994–1998 and 2009–2010, mean intakes continue to exceed recommended limits.
Keywords: Child, adolescent, nutrition, dietary intake United States, cross-sectional surveys
INTRODUCTION
There are increasing global concerns about improving the dietary intakes of children and adolescents. The World Health Organization Global Strategy on Diet, Physical Activity and Health recommends limiting intakes of free (added) sugars, saturated fat and sodium, increasing consumption of fruits and vegetables, and legumes, whole grains and nuts and eliminating trans-fatty acids 1. In the United States (U.S.), diet quality has been linked with concern not only for pediatric overweight and obesity but also for increasing pediatric nutrition-related cardiometabolic problems.2-5 Reducing excessive energy intake has thus become a major goal in the U.S., highlighted by the Dietary Guidelines for Americans.6 While slightly different from global recommendations, the Dietary Guidelines for Americans emphasize the need to reduce energy from foods and beverages that provide empty calories from solid fats and added sugars (SoFAS). There is general agreement among nutrition scholars that unhealthy fats and added sugars are key sources of surplus energy intake and overall indicators of unhealthy dietary patterns.1, 7, 8
Although the percent of daily calories consumed from added sugars has declined between 1999–2000 and 2007–2008,9 scholars have shown that U.S. children and adolescents still consumed excessive added sugars in 2005-2008.10 Reported intakes of solid fats among U.S. children and adolescents in 2003-2004 also exceeded allowance levels,11 though analyses on trends in solid fat intakes over the previous decade do not exist. The present study incorporates the most recent nationally representative dietary intake data from 2009-2010 to expand our understanding of the trends in both solid fats and added sugars consumption among U.S. children and adolescents.
This study highlights 15 year trends in SoFAS consumption among U.S. children age 2-18. Using five nationally representative surveys of food intake in the U.S. we report average daily intakes of solid fat and added sugars as well as the percentage of total energy intake from solid fat and added sugars and examine differential trends among age, race/ethnic and income subpopulations.
METHODS
Data Sources and Samples
We used cross-sectional data on children and adolescents ages 2-18 years from five nationally representative surveys of food intake in the United States: the Continuing Survey of Food Intakes by Individuals Surveys (CSFII) 1994 to 1996 (CSFII 96, n=8,259) and the National Health and Nutrition Examination Surveys (NHANES) 2003 to 2004 (NHANES 04, n=3,435), 2005 to 2006 (NHANES 06, n=3,652), 2007 to 2008 (NHANES 08, n=2,594) and 2009 to 2010 (NHANES 10, n=2,763). Detailed information about the operation of each survey and its sampling design has been published elsewhere.12-16 The results were weighted using the NHANES examination sample weights to provide nationally representative information on American’s food and nutrient intakes at the time of the survey and to adjust for the complex sample design of NHANES.
Dietary Intake
Data from two 24-hour recalls were collected using the United States Department of Agriculture (USDA) Automated Multiple-Pass Method (AMPM).17 This 5-step dietary interview process includes multiple passes through the 24 h of the previous day, during which respondents receive cues to help them remember and describe foods they consumed. The Day 1 interview was conducted in person in a Mobile Examination Center and was used for this study. For the CSFII 1994-1996 and 1998, the main meal planner/preparer within a household reported for children less than 12 years of age. For the What We Eat in America (WWEIA), NHANES 2003-2004, 2005-2006, 2007-2008 and 2009-2010 survey participants aged 12 years and older completed the dietary interview on their own, proxy-assisted interviews were conducted with children aged 6 to 11 years, and proxy respondents reported for children younger than age 5 years. Details of each dietary data collection method are published elsewhere.18-22
Food composition information
Total energy intake
Dietary intake data from each survey period were linked to a food composition database developed by the USDA with nutrient values corresponding to the diets of individuals at the time of processing. For CSFII 1994-98, data was used from the Survey Nutrient Database which was maintained for use with nationwide food surveys. For WWEIA, NHANES 2003-2004, 2005-2006, 2007-2008 and 2009-2010, data was used from the USDA’s Food and Nutrient Database for Dietary Studies (FNDDS) which is used to code, process and analyze the data assessed in the course of the WWEIA survey.23-27 Each nutrient data base was derived from the USDA Nutrient Data Base for Standard Reference (SR), versions 11, 18, 20 and 22.28
Energy from solid fats and added sugars
We used the USDA’s MyPyramid Equivalents Database (MPED) to examine consumption of energy from solid fat and added sugars. Multi-ingredient foods are disaggregated into their basic ingredients and the solid fat and added sugars present in each ingredient are classified. MPED values for grams of solid fat and teaspoons of added sugars were converted based on 9 kcal/g and 16 kcal/tsp, respectively. MPED version 1.0 was used for CSFII 1994-98; MPED version 2.0 was used for WWEIA, NHANES 2003-2004 and MPED version 2.0 addendum was used for WWEIA, NHANES 2005-2006, 2007-2008 and 2009-2010.29-31
Food and beverage groupings
The food grouping system used for this study originated with the nine USDA food groupings and then groupings were systematically disaggregated based on nutrient composition, critical dietary behaviors and similarities in consumption patterns (e.g., ready-to-eat cereals and savory snacks). In addition, select popular foods (e.g., pizza and hamburgers/cheeseburgers) were classified as their own group. A total of 41 mutually exclusive food groups and 12 beverages groups were created. Eight-digit food/beverage codes assigned by the USDA to each item were linked to a designated food group to ensure that foods and beverages were consistently placed in the same group across the six times periods used in this study. Figure 1 provides a complete list of food and beverage groups.
Figure 1.

List of food and beverage groupings
With advances in dietary data collection and coding methods, the flexibility and specificity of intake data has improved over time. During the collection and coding of dietary recall data, individual food codes may be linked together using “combination” codes which allow combining the nutritional information of individual foods that are consumed together at an eating occasion. For example, sugar in coffee or food mixtures, such as a homemade burrito, that is reported as separate ingredients: beans, cheese, lettuce and salsa, can be combined into single food items. It is important to note that not all aggregated foods are captured by this coding scheme. In order to describe consumption trends in comparable food and beverage groupings over time, select combination codes relevant to the current research question (specifically, beverages, corn and tortilla products, soups, and ice cream with additions) were incorporated. For each of these examples, the nutrient content of every individual item was summed into one combined food or beverage.
Statistical analysis
Dietary recalls (Day 1 only) for all 2-18 year olds with data on dietary intake variables of interest were included in this analysis. Appropriate weighting factors were applied to adjust for differential probabilities of selection and various sources of nonresponse.32 Mean intakes of total energy, solid fat and added sugars from each food category were estimated as was the contribution of solid fat and added sugars to total energy intakes. Trends are presented as calories per capita per day. Differences were examined by age (2-5 years, 6-11 years and 12-18 years), race/ethnicity (Non-Hispanic White, Non-Hispanic Black and Mexican-American) and family income (<130% of poverty income ratio, 130-350% of poverty income ratio, ≥350% of poverty income ratio). To test for statistical differences between years, we used independent 2-sample t tests. Differences were considered statistically significant at the p <0.05 level with Bonferroni correction.33Data analyses were conducting using Stata (version 11.0, 2009, StataCorp, College Station, TX).
RESULTS
Sociodemographic characteristics of the analytic sample are reported in Table 1. There were minor differences in the distributions of race/ethnicity and income over the surveys, the greatest of which were an 8% decrease in the proportion of non-Hispanic Whites and 8% increases in both the proportion of Mexican Americans and children from lower income households between 1989-1991 and 2009-2010.
Table 1.
Percentages of the US population age 2-18 by sociodemographic characteristics from National Nutrition Surveys, 1989 to 2010*
| Continuing Survey of Food Intakes by Individuals and 1994-96 Diet and Health Knowledge Survey (CSFII) 1994-1998 (n=8,259) | What We Eat in America, National Health and Nutrition Examination Survey (WWEIA, NHANES) 2003-2004 (n=3,435) | What We Eat in America, National Health and Nutrition Examination Survey (WWEIA, NHANES) 2005-2006 (n=3,652) | What We Eat in America, National Health and Nutrition Examination Survey (WWEIA, NHANES) 2007-2008 (n=2,594) | What We Eat in America, National Health and Nutrition Examination Survey (WWEIA, NHANES) 2009-2010 (n=2,763) | |
|---|---|---|---|---|---|
| Age group | |||||
| 2-5 y | 0.24 | 0.22 | 0.22 | 0.23 | 0.23 |
| 6-11 y | 0.36 | 0.35 | 0.34 | 0.34 | 0.34 |
| 12-18 y | 0.40 | 0.43 | 0.43 | 0.42 | 0.42 |
| % Female Income as a % of poverty | 0.49 | 0.49 | 0.49 | 0.50 | 0.50 |
| ≤130% | 0.24 | 0.33 | 0.27 | 0.32 | 0.33 |
| 131-185% | 0.13 | 0.11 | 0.10 | 0.10 | 0.12 |
| >185% | 0.62 | 0.56 | 0.63 | 0.58 | 0.55 |
| Race-ethnic status | |||||
| % non-Hispanic White | 0.70 | 0.65 | 0.63 | 0.64 | 0.62 |
| % non-Hispanic Black | 0.17 | 0.16 | 0.15 | 0.16 | 0.14 |
| Mexican-Americans† | 0.07 | 0.13 | 0.14 | 0.14 | 0.15 |
| Other | 0.05 | 0.06 | 0.08 | 0.06 | 0.08 |
Weighted percentages have been adjusted to be nationally representative.
Analyses are limited to Mexican Americans because of sampling constraints in WWEIA.
Total Energy Intake
The average daily intake of energy among all U.S. 2-18 year olds declined from 2003-2010, decreasing from 2115 calories per day in 2003-2004 to 1914 calories per day in 2009-2010 (p< 0.05) (Table 2). In contrast, over the same time period average daily energy intakes among 12-18 year olds, non-Hispanic Blacks and children from middle income households did not decrease significantly.
Table 2.
Mean intakes of energy from solid fats and added sugars among children and adolescents in the United States (2-18 years), by age, race/ethnicity and family income from 1994-2010*.
| CSFII 1994-1998 (n=8,259) | WWEIA, NHANES 2003-2004 (n=3,435) | WWEIA, NHANES 2005-2006 (n=3,652) | WWEIA, NHANES 2007-2008 (n=2,594) | WWEIA, NHANES 2009-2010 (n=2,763) | |
|---|---|---|---|---|---|
| All | |||||
| Total energy, Mean kcal ± SE | 2016 ± 26 | 2115 ± 22 | 2035 ± 33 | 1906 ± 261,2,3 | 1914 ± 272 |
| % energy from SoFAS | 39% | 37% | 36%1 | 35%1,2 | 33%1,2,3 |
| % energy from solid fat | 21% | 20% | 20% | 20%1 | 19%1,3 |
| % energy from added sugar | 18% | 17% | 16%1 | 15%1,2 | 14%1,2,3 |
| 2-5 y | |||||
| Total energy, Mean kcal ± SE | 1587 ± 13 | 1721 ± 251 | 1566 ± 232 | 1510 ± 252 | 1543 ± 262 |
| % energy from SoFAS | 36% | 35% | 33%1 | 33%1,2 | 32%1,2 |
| % energy from solid fat | 21% | 21% | 19%1 | 20%2 | 20% |
| % energy from added sugar | 15% | 14% | 14%1 | 13%1 | 12%1,2,3 |
| 6-11 y | |||||
| Total energy, Mean kcal ± SE | 1934 ± 22 | 2120 ± 491 | 1981 ± 37 | 1931 ± 272 | 1865 ± 202 |
| % energy from SoFAS | 39% | 38% | 37%1 | 36%1 | 33%1,2,3,4 |
| % energy from solid fat | 21% | 20% | 21% | 20%1 | 19%1,3 |
| % energy from added sugar | 18% | 17% | 16%1 | 16%1 | 14%1,2,4 |
| 12-18 y | |||||
| Total energy, Mean kcal ± SE | 2352 ± 49 | 2317 ± 48 | 2315 ± 51 | 2106 ± 441,2,3 | 2157 ± 58 |
| % energy from SoFAS | 40% | 38%1 | 37%1 | 35%1 | 34%1,2,3 |
| % energy from solid fat | 20% | 19%1 | 20% | 19% | 18%1 |
| % energy from added sugar | 19% | 19% | 17%1 | 16%1 | 15%1,2 |
| Male | |||||
| Total energy, Mean kcal ± SE | 2242 ± 34 | 2295 ± 42 | 2258 ± 50 | 2065 ± 361,2 | 2066 ± 392 |
| % energy from SoFAS | 39% | 37% | 37% | 35%1,2 | 33%1,2,3,4 |
| % energy from solid fat | 21% | 20% | 20% | 19%1,3 | 19%1,2,3 |
| % energy from added sugar | 18% | 18% | 16% | 16%1,2 | 14%1,2,3 |
| Female | |||||
| Total energy, Mean kcal ± SE | 1777 ± 26 | 1924 ± 261 | 1798 ± 212 | 1747 ± 332 | 1761 ± 282 |
| % energy from SoFAS | 38% | 37% | 36%2 | 35%1,2 | 33%1,2 |
| % energy from solid fat | 20% | 20% | 20% | 20% | 19%2 |
| % energy from added sugar | 18% | 17% | 16%1 | 15%1,2 | 14%1,2 |
| Non-Hispanic White | |||||
| Total energy, Mean kcal ± SE | 2059 ± 32 | 2133 ± 32 | 2101 ± 41 | 1956 ± 412 | 1921 ± 361,2,3 |
| % energy from SoFAS | 39% | 38% | 37%1 | 36%1 | 34%1,2,3,4 |
| % energy from solid fat | 21% | 20% | 20% | 20% | 19%1,2 |
| % energy from added sugar | 18% | 18% | 16%1 | 16%1 | 15%1,2 |
| Non-Hispanic Black | |||||
| Total energy, Mean kcal ± SE | 1975 ± 41 | 2093 ± 48 | 1941 ± 40 | 1847 ± 442 | 1937 ± 57 |
| % energy from SoFAS | 40% | 37% | 36%1 | 35%1,2 | 33%1,2,3 |
| % energy from solid fat | 22% | 20%1 | 20%1 | 19%1 | 19%1,3 |
| % energy from added sugar | 17% | 17% | 16% | 15%1,2 | 14%1,2 |
| Mex-Americans | |||||
| Total energy, Mean kcal ± SE | 1846 ± 75 | 2131 ± 451 | 1930 ± 332 | 1810 ± 392 | 1849 ± 402 |
| % energy from SoFAS | 36% | 36% | 33%1 | 33%1,2 | 31%1,2 |
| % energy from solid fat | 20% | 20% | 19% | 19% | 18%1 |
| % energy from added sugar | 16% | 16% | 14% | 14%1,2 | 13%1,2 |
| ≤ 130% PIR | |||||
| Total energy, Mean kcal ± SE | 1976 ± 39 | 2154 ± 61 | 1928 ± 462 | 1924 ± 422 | 1905 ± 362 |
| % energy from SoFAS | 38% | 37% | 35%1 | 35%1 | 33%1,2,3 |
| % energy from solid fat | 22% | 20% | 20%1 | 19%1 | 19%1 |
| % energy from added sugar | 16% | 17% | 15% | 16% | 14%1,2 |
| 131-185% PIR | |||||
| Total energy, Mean kcal ± SE | 1938 ± 47 | 2000 ± 97 | 2047 ± 122 | 1931 ± 75 | 1819 ± 73 |
| % energy from SoFAS | 40% | 37% | 36%1 | 35%1 | 35%1 |
| % energy from solid fat | 22% | 20% | 20% | 20% | 19%1 |
| % energy from added sugar | 18% | 17% | 15% | 15%1 | 16% |
| > 185% PIR | |||||
| Total energy, Mean kcal ± SE | 2049 ± 34 | 2108 ± 30 | 2087 ± 42 | 1882 ± 461,2,3 | 1916 ± 422,3 |
| % energy from SoFAS | 38% | 37% | 37%1 | 35%1 | 33%1,2,3,4 |
| % energy from solid fat | 20% | 20% | 20% | 20% | 19%1,3 |
| % energy from added sugar | 18% | 18% | 16%1 | 15%1,2 | 14%1,2,3 |
SE (Standard Error); SoFAS (solid fats and added sugars); PIR (poverty income ratio)
Data sources: Data from the Continuing Survey of Food Intakes by Individuals (CSFII) of 1994-1998 (n=7,758), What We Eat in America (WWEIA) National Health and Nutrition Examination Survey (NHANES) 2003-2004 (n=3,272), WWEIA, NHANES 2005-2006 (n=3,432), WWEIA, NHANES 2007-2008 (n=2,450), WWEIA, NHANES 2009-2010 (n=2,763).
Significantly different from 1994-98 at p<0.05
Significantly different from 2003-04 at p<0.05
Significantly different from 2005-06 at p<0.05
Significantly different from 2007-08 at p<0.05
Total Solid Fats and Added Sugars (SoFAS)
The intake of SoFAS as a percentage of total energy intake among U.S. children age 2-18 declined from 1994-2010, decreasing from 39% in 1994-1998 to 33% in 2009-2010 (p<0.05) (Table 2). The average daily intake of energy from SoFAS among U.S. 2-18 year olds also declined over the same time period, decreasing from 797 calories per day in 1994-1998 to 646 calories per day in 2009-2010 (p< 0.05) (Appendix 1).
For most age, sex, race/ethnic and income groups, intakes of SoFAS remained stable from 1994-2006 and were significantly lower only in the 2007-2008 and 2009-2010 time periods. Among select age (2-5y), sex (female), race/ethnic (Mexican-Americans) and income (low income) groups the decrease in SoFAS intake began earlier such that SoFAS were significantly lower in the 2005-2006 period as compared to the 1994-2004 period. The only decrease in daily intake of SoFAS from 2007-2008 to the most recent period (2009-2010) was among 6-11 year olds and males.
Solid Fats
Among all age, sex, race/ethnic and income groups solid fats accounted for a greater proportion of total energy intake than did added sugars (Table 2). The intake of solid fat as a percentage of total energy intake among U.S. children age 2-18 declined slightly from 21% in 1994-1998 to 19% in 2009-2010 (p<0.05) (Table 2), however among 2-5 year olds no change was observed.
The average daily intake of energy from solid fats among U.S. 2-18 year olds declined from 1994-2010, decreasing from 426 calories per day in 1994-1998 to 368 calories per day in 2009-2010 (Appendix 1). For most age, race and income groups intakes of solid fats were significantly lower in the 2007-2010 periods as compared to the 1994-2006 periods. Among select age (2-5y and 12-18y), and race/ethnic (Mexican-Americans) groups the decrease in solid fat intake began earlier such that SoFAS were significantly lower in the 2005-2006 period as compared to the previous period. The only decrease in solid fat intake from 2007-2008 to the most recent period (2009-2010) was among 6-11 year olds. Little change in solid fat intake was observed among females, with only the difference being lower reported solid fat intakes in 2009-2010 as compared to 2003-2004.
The main sources of solid fat intake (food groups with the highest mean intakes at each survey period) among U.S. children age 2-18 were milk (including whole and reduced-fat versions), grain-based desserts, pizza, cheese, processed meats and fried potatoes (Figure 2a and Appendix 2). These sources varied by income and race/ethnic subgroups (Appendices 3, 4 and 5). Additional major contributors included dairy-based desserts among non-Hispanic Whites, children from middle and higher income households and 6-11 year olds, tortilla- and corn-based dishes among Mexican Americans, children from low-income households and 6-11 and 12-18 year olds and pasta dishes among 2-5 year olds and children from middle income households.
Figure 2.
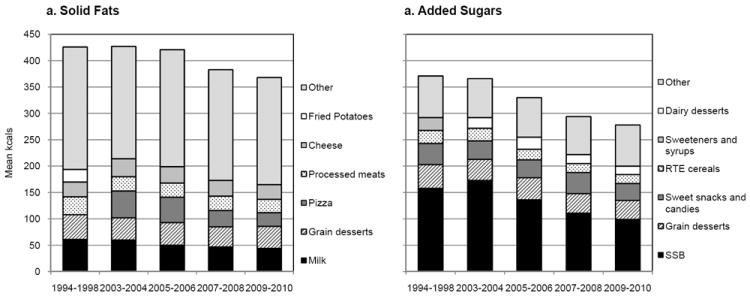
Major sources of solid fats and added sugars among children and adolescents in the United States (2-18 years) from 1994-2010a
a Data sources: Data from the Continuing Survey of Food Intakes by Individuals (CSFII) of 1994-1998 (n=8,259), What We Eat in America (WWEIA) National Health and Nutrition Examination Survey (NHANES) 2003-2004 (n=3,435), WWEIA, NHANES 2005-2006 (n=3,652), WWEIA, NHANES 2007-2008 (n=2,594), WWEIA, NHANES 2009-2010 (n=2,763).
Added Sugars
The intake of added sugars as a percentage of total energy intake among U.S. children age 2-18 declined considerably from 18% in 1994-1998 to 14% in 2009-2010 (p<0.05) (Table 2). The average daily intake of energy from added sugars among U.S. 2-18 year olds also declined from 1994-2010, decreasing from 371 calories per day in 1994-1998 to 278 calories per day in 2009-2010 (Appendix 1). For most age, race/ethnic and income groups intakes of added sugars were significantly lower in the 2005-2008 periods as compared to the 1994-2004 periods. The only decrease in added sugars from 2007-2008 to the most recent period (2009-2010) was among 6-11 year olds.
The main sources of added sugar intake (food groups with the highest mean intakes at each survey period) among U.S. children age 2-18 were sugar-sweetened beverages (SSB), grain-based desserts, candy and other sweet snacks, ready-to-eat cereals, dairy-based desserts and sweeteners and syrups (Figure 2b and Appendix 2). In general these sources were consistent across all income and race/ethnic subgroups. The few exceptions included flavored/sweetened milk among children from low income families, Mexican Americans and 2-5 and 6-11 year old children as well as flavored/sweetened coffees and teas among children from middle income families and 12-18 year olds (Appendices 3, 4 and 5).
DISCUSSION
Increasing global concerns regardingchild and adolescent diets have resulted in recommendations to limit intakes of free (added) sugars and saturated fat.1 The US Dietary Guidelines for Americans reflect these recommendations using solid fat in lieu of saturated fat. The 2010 guidelines recommend that total SoFAS intake be limited to 5-15% of total energy intake depending on energy needs.6 Despite recent declines in the percentage of total daily energy intake from SoFAS (from 39% in 1994-1998 to 33% in 2009-2010), intakes among U.S. children and adolescents still far exceed recommended levels. Of particular importance, among 2-5 year olds the percent of energy intake from solid fats did not decrease over the 15 year period.
To the authors’ knowledge this is the first report of trends in solid fat intakes among U.S. children and adolescents. Intakes of solid fats only slightly decreased from 1994-2010 and accounted for a greater proportion of total energy intake than did added sugars at all time points. The observed decreases in added sugars intakes are supported by similar findings from Welsh and colleagues of decreases in added sugars consumption in the U.S. between 1999-2000 and 2007-2008 among all U.S. children and adults (≥2 years). The current study expands our understanding of added sugars, demonstrating that intakes have not decreased in the most recent time period (from 2007-2008 to 2009-2010). Taken together, these results suggest that the decreases in SoFAS intakes observed through 2007-2008 have leveled off and that decreases have primarily been due to reductions in added sugars intakes.
The main sources of SoFAS intakes over the 16-year period were SSBs, grain-based desserts, candy, ready-to-eat cereals, dairy-based desserts, milk, pizza, cheese, processed meats and fried potatoes. Other investigators have examined key food and beverage sources of SoFAS in the U.S. diet. Bachman and colleagues assessed the key sources of SoFAS among all persons aged 2 years and older using data from NHANES 2001-200234 and Reedy and Krebs-Smith examined the key sources of solid fats and added sugars among children and adolescents using data from NHANES 2003-2004.11 Although the food groupings were slightly different, our analysis identified similar sources of SoFAS among U.S. children and adolescents from 1994-2010.
More research is needed to understand why the observed declines in SoFAS intake among U.S. children and adolescents may be occurring. Increased public dialog over the course of the time periods under study heightened awareness of childhood obesity and healthy eating across the U.S. Numerous initiatives focused attention on limiting the consumption of foods and beverages high in unhealthy fats and added sugars. Several efforts sought to improve the dietary quality of school feeding programs and to remove food and beverage sources of SoFAS from U.S. child care settings, school cafeterias and school vending machines.35 There were also increases in U.S. state-level taxes on snack foods, soda, and other sweetened beverages during the time periods under study.36 Finally, the role of private sector efforts to reformulate food and beverage products37, 38 has not yet been seriously evaluated; however a recent case study of the two largest and most influential sweetened beverage producers suggest a shift toward water and reduced calorie beverage purchases.39
Whether the observed declines in SoFAS intake among U.S. children and adolescents reflect a true downward trend (due to heightened awareness of pediatric overweight and initiatives to improve diet) or recent economic shifts (including increases in global food prices and the Great Recession), cannot be inferred from this study. In ongoing but as yet unpublished research, our team is examining sales and purchases of consumer packaged goods foods and beverages from 2000-2011. Unreported results suggest that declines in purchases of important sources of SoFAS in the U.S. began prior to the Great Recession of 2007-2010.40
While the current analysis captures the past 15 years, it misses the major shifts that occurred in American diets prior to 1994. Previous work from our research group with earlier dietary data showed that national consumption rates of caloric sweeteners increased from 13% of total energy in 1977–1978 to 16% of total energy in 1994–199641 and again to 18% by 1999-2000.42 Combined with findings from Welsh and colleagues national added sugars consumption subsequently decreased to a low of 14% of total energy in 2009–2010. These data demonstrate that the consumption of added sugars peaked in the early part of the decade, declined steadily through 2007-2008 and has remained relatively stable from 2007-2008 through 2009-2010. Previous literature also documents increases in total energy intakes, portion sizes and snacking from the 1970’s to the 1990’s among U.S. children and adolescents as well as increases in energy intake from specific sources such as pizza and SSBs.43-45
Recent research from Brazil reveals even greater SoFAS intakes among Brazilian adolescents (saturated and trans fats were assessed as a proxy for solid fats).46 Using a nationally representative survey and methods comparable to those used in this study, Pereira and colleagues observed that 54% of total energy intake reported by Brazilian adolescents was from SoFAS. Meats were the main contributor of saturated and trans fats and beverages were the main contributor of added sugar in the Brazilian adolescent population. Studies on SoFAS intakes from other countries could not be found though there is an extensive literature demonstrating increases in added sugar and sugar-sweetened beverage intakes across the globe.39, 47-50
The current results, while highlighting a recent decline in added sugar intake among US children, show that the average US child still consumes approximately 268 kcal/d of added sugar, with SSB’s being the primary source. Evidence suggests that SSB consumption is associated with risk of diabetes.51 Reduced consumption of SSBs has been shown to be associated with reduced weight gain and fat accumulation in normal weight children 52 and reduced BMI gain in overweight and obese children.53
There is less literature and understanding of the role of excessive solid or saturated fat intake during childhood. The long-term STRIP study compared children fed low-fat and high fat milk from 6 months of age onwards and found increased risk of many cardiometabolic problems linked with the high fat milk.54, 55 We can assume that saturated fat in any food source would have a comparable effect.
Several cautions are noted to aid in the interpretation of our findings. The definition of added sugars in the MPED database does not include fruit juice concentrate as an added sweetener. We have previously shown that 7% of food and beverage products purchased by U.S. households in 2005-2009 contained fruit juice concentrate.56 Consequently, estimates of added sugars intakes based on the MPED definition are likely an underestimate of the true intake of added sugars. Because respondents are different from one set of survey years to another, identification of trends can be inferred but not confirmed.
Dietary intake assessment methods and food composition information have improved significantly over time. Although data presented are based on the first day 24-h recall from all surveys, the recall methodology was modified to include the USDA’s AMPM in WWEIA-NHANES surveys. While validation studies of the AMPM have not been conducted in children validation studies in adults have shown the AMPM improved completeness of the recall.17 As such, it is possible that the observed increases in SoFAS intake from 1994-2004 are an artifact of the more complete capture of the data.
Despite improvements in dietary assessments methods, research suggests that collecting reliable and accurate dietary data from children and adolescents remains difficult.57, 58 Underreporting of intake has been associated with factors such as age, race/ethnicity and body weight status,57-61 and underreporting appears to be greatest among unhealthy foods or foods perceived to be related to obesity.61-63 While we note that available dietary intake methods are considered to be capable of providing unbiased estimates of energy intake at the population level, it remains possible that with heightened awareness of pediatric overweight and obesity, the observed decreases are a result of the population’s differential underreporting of dietary intakes of SoFAS that may be perceived negatively. This may especially be a concern among the younger age groups where intake data are collected by proxy report (2-5 year olds) or through proxy-assisted interviews (6-11 year olds). It is also possible that those providing proxy reports unintentionally underreport because they do not observe meals and snacks consumed outside of the home (e.g., in child care settings). Participation in organized child care, day care centers, nurseries and preschools has increased slightly from 41% of preschool-aged children in 1999 to 43% of pre-school aged children in 2010.64, 65 We have no reason to believe that this increase would result in sufficient changes in unintentional underreporting to explain the observed decreases in SoFAS intakes among young children. Further, while methods for critically examining mis-reporting of nutrient intake data have been advocated,66, 67 these methods were developed for adults. Because of the complexities related to development and growth there is not yet a standard approach to examine mis-reporting in children and adolescents though research in this area is growing.68, 69 Finally, we acknowledge that the methods used in this analysis to estimate the mean of the population distribution of usual dietary intakes from 24-hour recalls assume lack of bias in reporting.
CONCLUSIONS
Although the consumption of solid fats and added sugars among children and adolescents in the United States decreased between 1994–1998 and 2009–2010, mean intakes continue to exceed recommended limits by 18 to 28% of total energy intake.
Supplementary Material
Acknowledgments
We thank the Robert Wood Johnson Foundation (Grant 67506) and the National Institutes of Health (R01 HL104580 and CPC 5 R24 HD050924) for financial support. We also wish to thank Dr. Phil Bardsley for exception assistance with the data management and programming and Ms. Frances L. Dancy for administrative assistance.
Footnotes
None of the authors have conflict of interests of any type with respect to this manuscript.
References
- 1.WHO. Global strategy on diet, physical activity and health. Geneva, Switzerland: 2004. [Google Scholar]
- 2.Li C, Ford ES, Zhao G, Mokdad AH. Prevalence of pre-diabetes and its association with clustering of cardiometabolic risk factors and hyperinsulinemia among U.S. adolescents: National Health and Nutrition Examination Survey 2005-2006. Diabetes Car. 2009;32:342–347. doi: 10.2337/dc08-1128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pinhas-Hamiel O, Zeitler P. The global spread of type 2 diabetes mellitus in children and adolescents. J Pediatr. 2005;146:693–700. doi: 10.1016/j.jpeds.2004.12.042. [DOI] [PubMed] [Google Scholar]
- 4.Pinhas-Hamiel O, Zeitler P. Acute and chronic complications of type 2 diabetes mellitus in children and adolescents. Lancet. 2007;369:1823–31. doi: 10.1016/S0140-6736(07)60821-6. [DOI] [PubMed] [Google Scholar]
- 5.Urakami T, Suzuki J, Yoshida A, et al. Prevalence of components of the metabolic syndrome in schoolchildren with newly diagnosed type 2 diabetes mellitus. Pediatr Diabetes. 2009;10:508–12. doi: 10.1111/j.1399-5448.2009.00533.x. [DOI] [PubMed] [Google Scholar]
- 6.USDA, USDHHS. Dietary Guidelines for Americans 2010. U.S. Government Printing Office; Washington, DC: 2010. [Google Scholar]
- 7.Monteiro CA, Gomes FS, Cannon G. The snack attack. Am J Public Health. 2010;100:975–981. doi: 10.2105/AJPH.2009.187666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stanley WC, Shah KB, Essop MF. Does junk food lead to heart failure? Importance of dietary macronutrient composition in hypertension. Hypertension. 2009;54:1209–1210. doi: 10.1161/HYPERTENSIONAHA.109.128660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Welsh JA, Sharma AJ, Grellinger L, Vos MB. Consumption of added sugars is decreasing in the United States. Am J Clin Nutr. 2011;94:726–34. doi: 10.3945/ajcn.111.018366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ervin R, Kit B, Carrol M, Ogden C. Consumption of added sugar among U S children and adolescents, 2005–2008. NCHS; Hyattsville, MD: 2012. [PubMed] [Google Scholar]
- 11.Reedy J, Krebs-Smith SM. Dietary sources of energy, solid fats, and added sugars among children and adolescents in the United States. JADA. 2010;110:1477–1484. doi: 10.1016/j.jada.2010.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.U.S. Department of Agriculture ARS. Continuing Survey of Food Intakes by Individuals 1994-96, 1998. 2000 http://www.ars.usda.gov/Services/docs.htm?docid=14531.
- 13.Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. [2003-2004]. [ http://www.cdc.gov/nchs/nhanes/nhanes2003-2004/nhanes03_04.htm]
- 14.Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. [2005-2006]. [ http://www.cdc.gov/nchs/nhanes/nhanes2005-2006/nhanes05_06.htm]
- 15.Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. [2007-2008]. [ http://www.cdc.gov/nchs/nhanes/nhanes2007-2008/nhanes07_08.htm]
- 16.Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. [2009-2010]. [ http://www.cdc.gov/nchs/nhanes/nhanes2009-2010/nhanes09_10.htm]
- 17.Moshfegh AJ, Rhodes DG, Baer DJ, et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88:324–332. doi: 10.1093/ajcn/88.2.324. [DOI] [PubMed] [Google Scholar]
- 18.U.S. Department of Agriculture ARS, Beltsville Human Nutrition Research Center, Food Surveys Research Group (Beltsville, MD) Continuing Survey of Food Intakes by Individuals 1994-96, 1998 and Diet and Health Knowledge Survey 1994-96: Documentation (csfii9498_documentationupdated.pdf) or Data Files (csfii9498_data.exe) Retrieved from USDA Agricultural Research Service, Food Surveys Research Group. http://www.ars.usda.gov/Services/docs.htm?docid=14531.
- 19.U.S. Department of Agriculture ARS, Beltsville Human Nutrition Research Center, Food Surveys Research Group (Beltsville, MD) and U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics (Hyattsville, MD) What We Eat in America, NHANES 2003-2004. 2006 http://www.cdc.gov/nchs/nhanes.htm.
- 20.U.S. Department of Agriculture ARS, Beltsville Human Nutrition Research Center, Food Surveys Research Group (Beltsville, MD) and U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics (Hyattsville, MD) What We Eat in America, NHANES 2005-2006. 2008 http://www.cdc.gov/nchs/nhanes.htm.
- 21.U.S. Department of Agriculture ARS, Beltsville Human Nutrition Research Center, Food Surveys Research Group (Beltsville, MD) and U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics (Hyattsville, MD) What We Eat in America, NHANES 2007-2008. 2010 http://www.cdc.gov/nchs/nhanes.htm.
- 22.U.S. Department of Agriculture ARS, Beltsville Human Nutrition Research Center, Food Surveys Research Group (Beltsville, MD) and U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics (Hyattsville, MD) What We Eat in America, NHANES 2009-2010. 2012 http://www.cdc.gov/nchs/nhanes.htm.
- 23.Ahuja JKA, Montville JB, Omolewa-Tomobi G, et al. USDA Food and Nutrient Database for Dietary Studies, 5.0. U.S. Department of Agriculture ARS, Food Surveys Research Group; Beltsville, MD: 2012. [Google Scholar]
- 24.Food Surveys Research Group. USDA Food and Nutrient Database for Dietary Studies, 4.1. Agricultural Research Service; Beltsville, MD: 2010. [Google Scholar]
- 25.Food Surveys Research Group. USDA Food and Nutrient Database for Dietary Studies, 3.0. Agricultural Research Service; Beltsville, MD: 2008. [Google Scholar]
- 26.Food Surveys Research Group. USDA Food and Nutrient Database for Dietary Studies, 2.0. Agricultural Research Service; Beltsville, MD: 2006. [Google Scholar]
- 27.Food Surveys Research Group. USDA Food and Nutrient Database for Dietary Studies, 5.0. Agricultural Research Service; Beltsville, MD: 2012. [Google Scholar]
- 28.USDA A. USDA National Nutrient Database for Standard Reference. Nutrient Data Laboratory Home Page. http://www.ars.usda.gov/ba/bhnrc/ndl.
- 29.Friday JE, Bowman SA. MyPyramid Equivalents Database for USDA Survey Food Codes, 1994-2002 Version 1.0. 2006 Online. [Google Scholar]
- 30.Bowman SA, Friday JE, Moshfegh A. My Pyramid Equvalents Database, 2.0 for USDA Survey Foods, 2003-2004. Food Surveys Research Group. 2008 [Google Scholar]
- 31.Koegel K, Kuczynski K. Center for Nutrition Policy and Promotion Addendum to the MyPyramid Equivalents Database 2.0. 2011 Online. [Google Scholar]
- 32.National Center for Health Statistics. Overview of NHANES Survey Design and Weights [Google Scholar]
- 33.Miller RG. Simultaneous statistical inference. 2. Springer Verlag; 1981. [Google Scholar]
- 34.Bachman JL, Reedy J, Subar AF, Krebs-Smith SM. Sources of food group intakes among the US population, 2001-2002. JADA. 2008;108:804–814. doi: 10.1016/j.jada.2008.02.026. [DOI] [PubMed] [Google Scholar]
- 35.William J. Clinton Foundation. Alliance for a Healthier Generation – Clinton Foundation and American Heart Association – and industry leaders set healthy school beverage guidelines for U.S. schools. 2006 [Google Scholar]
- 36.Chriqui JF, Eidson SS, Bates H, Kowalczyk S, Chaloupka FJ. State sales tax rates for soft drinks and snacks sold through grocery stores and vending machines, 2007. J Public Health Policy. 2008;29:226–249. doi: 10.1057/jphp.2008.9. [DOI] [PubMed] [Google Scholar]
- 37.Healthy Weight Commitment Foundation. Press Release. Washington, DC: 2010. Food and Beverage Manufacturers Pledging to Reduce Annual Calories By 1.5 Trillion By 2015. [Google Scholar]
- 38.Walmart. Walmart Launches Major Initiative to Make Food Healthier and Healthier Food More Affordable. 2011 [Google Scholar]
- 39.Kleiman S, Ng SW, Popkin B. Drinking to our health: can beverage companies cut calories while maintaining profits? Obes Rev. 2012;13:258–274. doi: 10.1111/j.1467-789X.2011.00949.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ng SW, Guilkey D, Popkin BM. How do recessions affect the caloric and volume purchases of Consumer Packaged foods and beverages in the US? University of North Carolina, Chapel Hill. 2012 [Google Scholar]
- 41.Popkin BM, Nielsen SJ. The sweetening of the world’s diet. Obes Res. 2003;11:1325–1332. doi: 10.1038/oby.2003.179. [DOI] [PubMed] [Google Scholar]
- 42.Duffey KJ, Popkin BM. High-fructose corn syrup: is this what’s for dinner? The Am J Clin Nutr. 2008;88:1722S–1732S. doi: 10.3945/ajcn.2008.25825C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Piernas C, Popkin BM. Food portion patterns and trends among U.S. children and the relationship to total eating occasion size, 1977-2006. J Nutr. 2011;141:1159–1164. doi: 10.3945/jn.111.138727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Piernas C, Popkin BM. Increased portion sizes from energy-dense foods affect total energy intake at eating occasions in US children and adolescents: patterns and trends by age group and sociodemographic characteristics, 1977–2006. Am J Clin Nutr. 201(94):1324–1332. doi: 10.3945/ajcn.110.008466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wang YC, Bleich SN, Gortmaker SL. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988-2004. Pediatrics. 2008;121:e1604–e1614. doi: 10.1542/peds.2007-2834. [DOI] [PubMed] [Google Scholar]
- 46.Pereira RA, Duffey KJ, Sichieri R, Popkin BM. Sources of excessive saturated fat, trans fat and sugar consumption in Brazil: an analysis of the first Brazilian nationwide individual dietary survey. Public Health Nutr. 2012 doi: 10.1017/S1368980012004892. Epub 1-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Steyn NP, Myburgh NG, Nel JH. Evidence to support a food-based dietary guideline on sugar consumption in South Africa. Bull World Health Organ. 2003;81:599–608. [PMC free article] [PubMed] [Google Scholar]
- 48.Duffey KJ, Huybrechts I, Mouratidou T, et al. Beverage consumption among European adolescents in the HELENA study. Eur J Clin Nutr. 2011;66:244–252. doi: 10.1038/ejcn.2011.166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ng SW, Mhurchu C, Jebb S, Popkin B. Patterns and trends of beverage consumption among children and adults in Great Britain, 1986-2009. Br J Nutr. 2011;20:1–16. doi: 10.1017/S0007114511006465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Popkin BM. Sugary beverages represent a threat to global health. Trends Endocrinol Metabol. 2012;23:591–593. doi: 10.1016/j.tem.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 51.Odegaard AO, Koh W-P, Arakawa K, Yu MC, Pereira MA. Soft Drink and Juice Consumption and Risk of Physician-diagnosed Incident Type 2 Diabetes. Am J Epidemiol. 2010;171:701–708. doi: 10.1093/aje/kwp452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.de Ruyter JC, Olthof MR, Seidell JC, Katan MB. A Trial of sugar-free or sugar-sweetened beverages and body weight in children. N Engl J Med. 2012;367:1397–1406. doi: 10.1056/NEJMoa1203034. [DOI] [PubMed] [Google Scholar]
- 53.Ebbeling CB, Feldman HA, Chomitz VR, et al. A randomized trial of sugar-sweetened beverages and adolescent body weight. N Engl J Med. 2012;367:1407–1416. doi: 10.1056/NEJMoa1203388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Kaitosaari T, Ronnemaa T, Raitakari O, et al. Effect of 7-year infancy-onset dietary intervention on serum lipoproteins and lipoprotein subclasses in healthy children in the prospective, randomized Special Turku Coronary Risk Factor Intervention Project for Children (STRIP) study. Circulation. 2003;108:672–677. doi: 10.1161/01.CIR.0000083723.75065.D4. [DOI] [PubMed] [Google Scholar]
- 55.Kaitosaari T, Ronnemaa T, Viikari J, et al. Low-saturated fat dietary counseling starting in infancy improves insulin sensitivity in 9-year-old healthy children: the Special Turku Coronary Risk Factor Intervention Project for Children (STRIP) study. Diabetes Care. 2006;29:781–785. doi: 10.2337/diacare.29.04.06.dc05-1523. [DOI] [PubMed] [Google Scholar]
- 56.Ng SW, Slining MM, Popkin BM. Use of caloric and noncaloric sweeteners in US consumer packaged foods, 2005-2009. J Acad Nutr Diet. 2012 doi: 10.1016/j.jand.2012.07.009. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Burrows TL, Martin RJ, Collins CE. A systematic review of the validity of dietary assessment methods in children when compared with the method of doubly labeled water. J Am Diet Assoc. 2010;110:1501–1510. doi: 10.1016/j.jada.2010.07.008. [DOI] [PubMed] [Google Scholar]
- 58.Livingstone MB, Robson PJ, Wallace JM. Issues in dietary intake assessment of children and adolescents. Br J Nutr. 2004;92:S213–S222. doi: 10.1079/bjn20041169. [DOI] [PubMed] [Google Scholar]
- 59.Bandini LG, Cyr H, Must A, Dietz WH. Validity of reported energy intake in preadolescent girls. Am J Clin Nutr. 1997;65:1138S–1141S. doi: 10.1093/ajcn/65.4.1138S. [DOI] [PubMed] [Google Scholar]
- 60.Bandini LG, Must A, Cyr H, Anderson SE, Spadano JL, Dietz WH. Longitudinal changes in the accuracy of reported energy intake in girls 10-15 y of age. Am J Clin Nutr. 2003;78:480–484. doi: 10.1093/ajcn/78.3.480. [DOI] [PubMed] [Google Scholar]
- 61.Bandini LG, Schoeller DA, Cyr HN, Dietz WH. Validity of reported energy intake in obese and nonobese adolescents. Am J Clin Nutr. 1990;52:421–425. doi: 10.1093/ajcn/52.3.421. [DOI] [PubMed] [Google Scholar]
- 62.Heitmann BL, Lissner L, Osler M. Do we eat less fat, or just report so? Int J Obes Relat Metab Disord. 2000;24:435–442. doi: 10.1038/sj.ijo.0801176. [DOI] [PubMed] [Google Scholar]
- 63.Schoeller DA. Limitations in the assessment of dietary energy intake by self-report. Metabolism. 1995;44:18–22. doi: 10.1016/0026-0495(95)90204-x. [DOI] [PubMed] [Google Scholar]
- 64.Survey of Income and Program Participation (SIPP) Who’s Minding the Kids? Child Care Arrangements. 2010 Spring; http://www.census.gov/hhes/childcare/data/sipp/index.html.
- 65.Survey of Income and Program Participation (SIPP) Who’s Minding the Kids? Child Care Arrangements. 1999 Spring; http://www.census.gov/hhes/childcare/data/sipp/index.html.
- 66.Black AE. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int J Obes Relat Metabol Disord. 2000;24:1119–1130. doi: 10.1038/sj.ijo.0801376. [DOI] [PubMed] [Google Scholar]
- 67.Schoeller DA. Limitations in the assessment of dietary energy intake by self-report. Metabolism. 1995;44:18–22. doi: 10.1016/0026-0495(95)90204-x. [DOI] [PubMed] [Google Scholar]
- 68.Sichert-Hellert W, Kersting M, Schöch G. Underreporting of energy intake in 1 to 18 year old German children and adolescents. Z Ernahrungswiss. 1998 Sep;37(3):242–51. doi: 10.1007/s003940050023. [DOI] [PubMed] [Google Scholar]
- 69.Börnhorst C, Huybrechts I, Ahrens W, et al. Prevalence and determinants of misreporting among European children in proxy-reported 24-hour dietary recalls. British Journal of Nutrition. 2012 doi: 10.1017/S0007114512003194. Epub 2012 Aug 6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.