

Abstract
Background Bioabsorbable plates are frequently utilized in the repair of skull base defects following transsphenoidal operations. Traumatic intracranial pseudoaneurysms are a rare complication of transsphenoidal surgery. To date, iatrogenic carotid pseudoaneurysm associated with the use of an absorbable plate has been reported once.
Results A 57-year-old man with a large nonfunctional pituitary macroadenoma underwent an endoscopic transsphenoidal operation with gross total resection. An absorbable plate was placed extradurally to reconstruct the sellar floor. He experienced delayed repeated epistaxis, followed by a right middle cerebral artery distribution embolic stroke. Computed tomorgraphy (CT) angiogram 6 weeks postoperatively revealed a 6 × 4 mm pseudoaneurysm located on the medial wall of the right cavernous internal carotid artery. Stent coiling was used to successfully obliterate the pseudoaneurysm, and the patient fully recovered.
Conclusion Delayed erosion of the carotid artery wall caused by a plate used to reconstruct the sellar floor may manifest with epistaxis or embolic stroke. The authors' preference is to avoid insertion of a rigid plate for sellar floor reconstruction in the absence of intraoperative cerebrospinal fluid (CSF) leaks, unless it is required to buttress a large skull base defect. Short-segment embolization with stent coiling is the preferred treatment option for carotid pseudoaneurysms following transsphenoidal operations.
Keywords: cavernous, carotid, pseudoaneurysm, artery
Introduction
The transsphenoidal approach is the most commonly utilized operation for the surgical treatment of sellar lesions and is a relatively safe operation in experienced centers.1 Following resection of pituitary adenomas and other sellar tumors, many surgeons utilize absorbable plates to reconstruct the bony sellar floor to serve as a buttress for the sellar contents and repair construct. Although usually safe, vascular injury in conjunction with insertion of rigid plates following sellar tumor resection has been described once before.2
Common complications of transsphenoidal operations include endocrine abnormalities and cerebrospinal fluid (CSF) leaks.3 Vascular injury is a rare but serious complication of transsphenoidal surgery encountered in 0.8 to 1.1% of cases, with an associated mortality of nearly 30%.4,5,6 The majority of vascular injuries are identified at the time of surgery, usually resulting from direct injury to the internal carotid artery during resection of tumor within the cavernous sinus or upon opening of the dura, often resulting in profuse arterial hemorrhage.6,7,8,9 Other described vascular complications include vasospasm, carotid thrombosis, cavernous sinus thrombosis, embolism, caroticocavernous fistula, or pseudoaneurysm.2,3,7,8,10,11,12,13,14,15,16,17,18,19
Postoperative carotid pseudoaneurysm, though rare, represents a grave risk to the patient if unrecognized. It may lead to delayed hemorrhagic or embolic complications when the patient is no longer in a monitored hospital setting. This case report highlights the importance of rapid diagnosis and treatment of these lesions. We present a rare case of delayed pseudoaneurysm and embolic stroke following erosion of a rigid plate into the cavernous internal carotid artery.
Case Report
A 57-year-old man with a nonfunctional pituitary macroadenoma causing vision loss underwent a gross total, endoscopic transsphenoidal resection (Fig. 1). The tumor was invading the right cavernous sinus wall. During the procedure to resect the tumor from this region, there was some venous bleeding that was easily controlled by temporarily packing the area using Gelfoam (Pfizer, New York, New York, USA) with thrombin. Following resection, a custom-fit bioabsorbable plate was placed extradurally to reconstruct the sellar floor. The patient was discharged home on postoperative day 2 in excellent condition. Four weeks later, he experienced epistaxis for which he was treated at an outside emergency department. The bleeding was controlled with nasal packs, and the patient was discharged home. Six weeks following the operation, he presented to clinic with dysarthria as well as left hand and facial weakness and was admitted for further work-up. Neuroimaging revealed subacute infarcts in right middle cerebral artery distribution. Computed tomography (CT) angiogram showed a 6 × 4 mm pseudoaneurysm located on the medial wall of the right cavernous internal carotid artery. A hypodensity likely representing the implanted absorbable plate was noted to be compressing the right carotid artery in this region (Fig. 2). Stent coiling with placement of eight detachable coils was used to successfully obliterate the pseudoaneurysm (Fig. 3). Follow-up digital subtraction angiogram and CT angiogram demonstrated durable obliteration of the pseudoaneurysm with preserved flow through the carotid artery. On follow-up, the patient's neurological deficits have resolved.
Fig. 1.
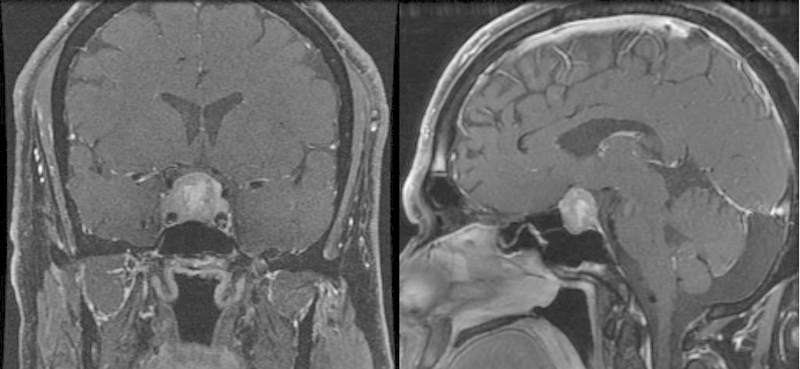
Preoperative MRI Sella with contrast.
Fig. 2.

CT-angiogram of the brain showing hypodense absorbable plate compressing the right cavernous carotid artery.
Fig. 3.
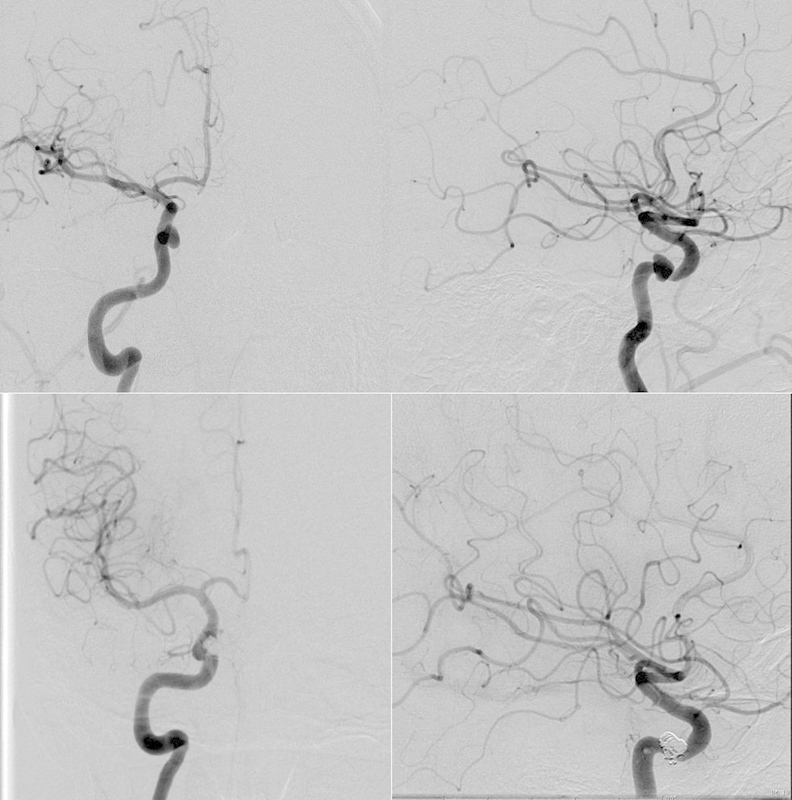
Digital subtraction angiogram showing right cavernous carotid pseudoaneurysm before and after stent-assisted coil embolization.
Discussion
Iatrogenic carotid pseudoaneurysm is an extremely rare complication of transsphenoidal surgery, with only 24 reported cases found in our review of the literature. Only one previous case was associated with sellar floor reconstruction.2 A pseudoaneurysm is caused by injury to the carotid artery wall leading to an encapsulated hematoma in communication with the ruptured artery. In general, an aneurysmal rupture of the cavernous carotid will result in a caroticocavernous fistula. However, severe epistaxis and pituitary apoplexy have been reported in patients whose medial cavernous sinus wall has been eroded by tumor or violated during surgery.4 Thus, the consequences of aneurysmal rupture support urgent treatment of even incidentally diagnosed lesions, as they represent a grave risk to the postoperative patient. Because of the extremely low reported incidence of pseudoaneurysms after transsphenoidal surgery, postoperative angiography is not routinely performed.6 Although in cases where there is significant arterial bleeding or concern for carotid injury, many experts recommend immediate postoperative angiography.6,15
Based on the uneventful operative course and features observed on CT angiogram, the pseudoaneurysm was likely caused by erosion of the absorbable plate into the cavernous carotid artery. This has been previously reported by Crowley et al and was also associated with delayed severe epistaxis followed by transient ischemic deficits.2 Despite its low complication rates, these cases highlight the risks associated with sellar floor reconstruction.20 Both patients were treated via endovascular means with good results. In a majority of cases, the absorbable plates used to reconstruct the bony sellar floor can be custom fit to approximate the size of the defect. The surgeon must take extra care to ensure that the cut edges are as round and smooth as possible, and that the size of the plate is just large enough to be inserted beneath the bony edges of the lateral sellar floor, and in an extradural fashion. Perhaps more importantly, the authors now make every attempt to only use a rigid buttress when necessary—that is, only in cases where intraoperative CSF leaks are observed in the setting of a large bony defect that cannot be repaired or adequately buttressed with routine techniques, including cellulose sponge, Duragen (Integra LifeSciences Corporation, Plainsboro, New Jersey, USA), and fibrin glue.
According to our search of the literature, 18 publications reporting 24 cases of iatrogenic carotid pseudoaneurysm following transsphenoidal surgery were identified (Table 1). Among published cases, the mean patient age was 45.6 (range 22 to 74), with a slight female predominance (13/22 patients). Intraoperative arterial hemorrhage requiring packing was described in 17 of 24 cases; 21% of cases reported the operation as uneventful. We recommend additional delayed imaging in patients with high suspicion for arterial injury, considering multiple reports in which the immediate postoperative angiogram was negative, only to have the patient present with a pseudoaneurysm in a delayed fashion.16,17,21 Common presentations prior to diagnosis included severe epistaxis,10 postoperative high-suspicion angiogram,10 routine follow-up imaging,2 and cranial neuropathy.1 The interval to diagnosis following surgery varied between 0 days and 10 years. Delay to diagnosis may lead to aneurysmal rupture or embolic stroke outside of a monitored setting. In fact, in nine cases reported in the literature, the patient was discharged from the hospital prior to the diagnosis being made.
Table 1. Diagnosis, Treatment, and Outcome of Pseudoaneurysms Following Transsphenoidal Surgery.
| Age/sex | Lesion | Intraoperative findings | Presentation/diagnosis of pseudoaneurysm | Time to diagnosis | Treatment | Outcome | |
|---|---|---|---|---|---|---|---|
| Wilson 197819 | NR | GH adenoma | Hemorrhage controlled with packing | Delayed epistaxis | NR | Emergency carotid ligation | NR |
| Paullus 197914 | 48M | Pituitary adenoma | Hemorrhage controlled with packing | Proptosis, complete left external ophthalmoplegia | 6 days | Clip left supraclinoid ICA, aneurysm embolized with muscle plugs, common carotid ligation | Panhypopituitary |
| Cabezudo 198110 | 41F | GH adenoma | Hemorrhage controlled with packing | Delayed epistaxis | 1 month | Gradual closure of carotid with Selverstone clamp over 7 days | Good |
| Reddy 199016 | 56F | GH Macroadenoma | Hemorrhage controlled with packing | Delayed epistaxis after negative angiogram on POD 1 and 7 | 6 weeks | Surgical clip of supraclinoid ICA and ligation of extracranial ICA | Good |
| Ahuja 19927 | 52F | GH microadenoma | Hemorrhage controlled with packing | Follow-up angiogram | 9 days | Endovascular balloon occlusion of ICA | Temporary hemiparesis |
| Raymond 199715 | 51F | ACTH adenoma | Unremarkable | Delayed epistaxis | 10 years | Endovascular balloon occlusion | Good |
| Raymond 199715 | 28M | GH adenoma | Hemorrhage controlled with packing | Angiogram | 10 days | Surgical packing | Good |
| Raymond 199715 | 74F | Pituitary Macroadenoma | Hemorrhage controlled with packing | Postoperative angiogram | Immediate | Failed carotid occlusion test no further treatment | Death at 2 years secondary to epistaxis |
| Bavinzki 199726 | 54F | NR | NR | Headache, giant aneurysm noted on head CT | 1 year | Cavernous carotid artery occlusion with Fogarty balloon catheter inserted through cervical ICA | Good |
| Chen 199821 | 25F | Traumatic CSF leak | Hemorrhage controlled with packing | Delayed epistaxis | 5 days | Endovascular balloon occlusion of ICA | Balloon migration causing episode of epistaxis, good at 6 years |
| Chen 199821 | 27F | Pituitary adenoma | Hemorrhage controlled with packing | Postoperative angiogram | Immediate | Endovascular balloon and coil occlusion of ICA | Good |
| Chen 199821 | 63M | Recurrent pituitary adenoma | Hemorrhage controlled with packing | Initial negative angiogram delayed epistaxis | 2 weeks | Failed BTO, coil embolization of pseudoaneurysm | Good |
| Laws 19996 | NR | NR | NR | NR | NR | Open repair via pterional craniotomy | NR |
| Dolenc 199913 | 39F | Pituitary adenoma | Hemorrhage controlled with packing | Angiogram | 3 days | Clip ligation of aneurysm | Good |
| Cappabianca 20018 | 22F | GH macroadenoma | Hemorrhage controlled with packing | Angiogram | NR | Coil embolization of pseudoaneurysm | NR |
| Kadyrov 20023 | 40M | Pituitary macroadenoma | Hemorrhage controlled with packing | Screening angiogram | 5 weeks | Stent-assisted coil embolization | Good |
| De Souza 200325 | 38F | GH adenoma | Hemorrhage | Postoperative MRI | NR | Endovascular placement of covered stent | Good |
| Kachhara 200324 | 40M | Prolactinoma macroadenoma | Hemorrhage controlled with packing | Angiogram | 2 days | Carotid ligation in neck and supraclinoid clip ligation | Good |
| Vanninen 200318 | 59F | Pituitary macroadenoma | Hemorrhage controlled with packing | Delayed epistaxis | 17 days | 12 mm PTFE-covered stent manually compressed on a PTCA balloon | Transient hemiparesis and aphasia |
| Ciceri 200612 | 55M | Pituitary adenoma | Unremarkable | Severe epistaxis | 10 days | None, unchanged with 9 years f/u | Good |
| Ciceri 200612 | 39 F | Pituitary adenoma | Unremarkable | Follow-up MRI | 1 year | Stent of ICA followed by coiling 3 months later | Good |
| Ciceri 200612 | 57M | Pituitary adenoma | Hemorrhage | Angiogram | Immediate | Permanent occlusion of the ICA with platinum coils and detachable balloons | Good |
| Crowely 20092 | 55M | Pituitary Macroadenoma | Unremarkable | Delayed epistaxis | 4 weeks | Coil occlusion of left cavernous carotid | Transient expressive aphasia |
| Struffert 200917 | 40M | Pituitary adenoma | Unremarkable | Delayed epistaxis | 10 days | Stent-assisted coil embolization of pseudoaneurysm | Coil migration retreatment by transsphenoidal, good |
| Current | 57M | Pituitary macroadenoma | Unremarkable | Delayed epistaxis, ischemic stroke | 6 weeks | Stent-assisted coil embolization of pseudoaneurysm | Transient hemiparesis, good |
Abbreviations: ACTH, adrenocorticotropic hormone; BTO, balloon test occlusion; CSF, cerebrospinal fluid; CT, computed tomography; GH, growth hormone; ICA, internal carotid artery; MRI, magnetic resonance imaging; NR, not reported, POD, postoperative day; PTCA, percutaneous trasnluminal coronary angioplasty; PTFE, polytetrafluoroethylene.
The treatment options for cavernous carotid pseudoaneurysms include open or endovascular surgery. Although conservative management may be an option, one report in which a patient refused surgical management resulted in death at 2 years secondary to uncontrollable epistaxis.15 Despite reports that conservatively managed postprocedure femoral pseudoaneurysms spontaneously close in 89% of patients, we recommend treatment even in incidental false aneurysms of the carotid because of the higher morbidity associated with carotid rupture.22
Additional surgical options for cavernous carotid pseudoaneurysms include extracranial to intracranial (EC-IC) bypass with carotid occlusion, craniotomy with direct repair of the carotid artery within the cavernous sinus, or trapping the aneurysm via cervical carotid ligation and supraclinoid carotid clip ligation.6,13,15,23,24 Endovascular options may include balloon occlusion of the carotid artery, coil embolization of the pseudoaneurysm or carotid artery, and/or placement of a flow-diverting stent.3,7,8,12,15,18 With the advancement in endovascular techniques, open surgery has become less common. Successful carotid artery occlusion, aneurysm trapping, stenting, or coiling can be achieved without subjecting the patient to the risks associated with open craniotomy and manipulation of a cavernous carotid pseudoaneurysm.
Some authors prefer carotid occlusion, when feasible, to avoid the risks associated with manipulation of the false aneurysm. Coil migration of cavernous pseudoaneurysms has been reported. Struffert described two cases requiring repeat transsphenoidal surgery to retrieve coils that had migrated from a pseudoaneurysm into the patients' nostril.17 The use of a flow-iverting stent may obviate the need for an intra-aneurysmal embolization.18,25 However, flow-diverting stents surrender future endovascular access to the pseudoaneurysm, because once deployed a microcatheter cannot be passed through it. If the patient experiences breakthrough bleeding, he or she could not be treated with further embolic agents.
Conclusion
Although rare, erosion of an absorbable plate used to reconstruct the bony sellar floor may cause a carotid artery pseudoaneurysm, potentially resulting in a subacute presentation of epistaxis or embolic stroke. The authors' preference is to avoid the use of rigid plating for sellar floor reconstruction in the absence of intraoperative CSF leaks, unless required to buttress a large skull base defect and CSF leak repair construct. Short-segment embolization with stent coiling is the preferred option for the treatment of iatrogenic carotid pseudoaneurysms following endonasal skull base operations.
References
- 1.Cappabianca P, Cavallo L M, Colao A, de Divitiis E. Surgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomas. J Neurosurg. 2002;97(2):293–298. doi: 10.3171/jns.2002.97.2.0293. [DOI] [PubMed] [Google Scholar]
- 2.Crowley R W, Dumont A S, Jane J A Jr. Bilateral intracavernous carotid artery pseudoaneurysms as a result of sellar reconstruction during the transsphenoidal resection of a pituitary macroadenoma: case report. Minim Invasive Neurosurg. 2009;52(1):44–48. doi: 10.1055/s-0028-1104611. [DOI] [PubMed] [Google Scholar]
- 3.Kadyrov N A, Friedman J A, Nichols D A, Cohen-Gadol A A, Link M J, Piepgras D G. Endovascular treatment of an internal carotid artery pseudoaneurysm following transsphenoidal surgery. Case report. J Neurosurg. 2002;96(3):624–627. doi: 10.3171/jns.2002.96.3.0624. [DOI] [PubMed] [Google Scholar]
- 4.Berker M, Aghayev K, Saatci I, Palaoğlu S, Onerci M. Overview of vascular complications of pituitary surgery with special emphasis on unexpected abnormality. Pituitary. 2010;13(2):160–167. doi: 10.1007/s11102-009-0198-7. [DOI] [PubMed] [Google Scholar]
- 5.Ciric I Ragin A Baumgartner C Pierce D Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience Neurosurgery 1997402225–236., discussion 236-237 [DOI] [PubMed] [Google Scholar]
- 6.Laws E R Jr. Vascular complications of transsphenoidal surgery. Pituitary. 1999;2(2):163–170. doi: 10.1023/a:1009951917649. [DOI] [PubMed] [Google Scholar]
- 7.Ahuja A Guterman L R Hopkins L N Carotid cavernous fistula and false aneurysm of the cavernous carotid artery: complications of transsphenoidal surgery Neurosurgery 1992314774–778., discussion 778-779 [DOI] [PubMed] [Google Scholar]
- 8.Cappabianca P, Briganti F, Cavallo L M, de Divitiis E. Pseudoaneurysm of the intracavernous carotid artery following endoscopic endonasal transsphenoidal surgery, treated by endovascular approach. Acta Neurochir (Wien) 2001;143(1):95–96. doi: 10.1007/s007010170144. [DOI] [PubMed] [Google Scholar]
- 9.Dusick J R Esposito F Malkasian D Kelly D F Avoidance of carotid artery injuries in transsphenoidal surgery with the Doppler probe and micro-hook blades Neurosurgery 200760402322–328., discussion 328-329 [DOI] [PubMed] [Google Scholar]
- 10.Cabezudo J M, Carrillo R, Vaquero J, Areitio E, Martinez R. Intracavernous aneurysm of the carotid artery following transsphenoidal surgery. Case report. J Neurosurg. 1981;54(1):118–121. doi: 10.3171/jns.1981.54.1.0118. [DOI] [PubMed] [Google Scholar]
- 11.Camp P E, Paxton H D, Buchan G C, Gahbauer H. Vasospasm after trans-sphenoidal hypophysectomy. Neurosurgery. 1980;7(4):382–386. doi: 10.1227/00006123-198010000-00012. [DOI] [PubMed] [Google Scholar]
- 12.Ciceri E F, Regna-Gladin C, Erbetta A. et al. Iatrogenic intracranial pseudoaneurysms: neuroradiological and therapeutical considerations, including endovascular options. Neurol Sci. 2006;27(5):317–322. doi: 10.1007/s10072-006-0703-y. [DOI] [PubMed] [Google Scholar]
- 13.Dolenc V V, Lipovsek M, Slokan S. Traumatic aneurysm and carotid-cavernous fistula following transsphenoidal approach to a pituitary adenoma: treatment by transcranial operation. Br J Neurosurg. 1999;13(2):185–188. doi: 10.1080/02688699943961. [DOI] [PubMed] [Google Scholar]
- 14.Paullus W S, Norwood C W, Morgan H W. False aneurysm of the cavernous carotid artery and progressive external ophthalmoplegia after transsphenoidal hypophysectomy. Case report. J Neurosurg. 1979;51(5):707–709. doi: 10.3171/jns.1979.51.5.0707. [DOI] [PubMed] [Google Scholar]
- 15.Raymond J, Hardy J, Czepko R, Roy D. Arterial injuries in transsphenoidal surgery for pituitary adenoma; the role of angiography and endovascular treatment. AJNR Am J Neuroradiol. 1997;18(4):655–665. [PMC free article] [PubMed] [Google Scholar]
- 16.Reddy K, Lesiuk H, West M, Fewer D. False aneurysm of the cavernous carotid artery: a complication of transsphenoidal surgery. Surg Neurol. 1990;33(2):142–145. doi: 10.1016/0090-3019(90)90024-j. [DOI] [PubMed] [Google Scholar]
- 17.Struffert T, Buhk J H, Buchfelder M, Rohde V, Doerfler A, Knauth M. Coil migration after endovascular coil occlusion of internal carotid artery pseudoaneurysms within the sphenoid sinus. Minim Invasive Neurosurg. 2009;52(2):89–92. doi: 10.1055/s-0029-1215579. [DOI] [PubMed] [Google Scholar]
- 18.Vanninen R L, Manninen H I, Rinne J. Intrasellar latrogenic carotid pseudoaneurysm: endovascular treatment with a polytetrafluoroethylene-covered stent. Cardiovasc Intervent Radiol. 2003;26(3):298–301. doi: 10.1007/s00270-003-2728-4. [DOI] [PubMed] [Google Scholar]
- 19.Wilson C B, Dempsey L C. Transsphenoidal microsurgical removal of 250 pituitary adenomas. J Neurosurg. 1978;48(1):13–22. doi: 10.3171/jns.1978.48.1.0013. [DOI] [PubMed] [Google Scholar]
- 20.Cappabianca P Cavallo L M Esposito F Valente V De Divitiis E Sellar repair in endoscopic endonasal transsphenoidal surgery: results of 170 cases Neurosurgery 20025161365–1371., discussion 1371-1372 [PubMed] [Google Scholar]
- 21.Chen D, Concus A P, Halbach V V, Cheung S W. Epistaxis originating from traumatic pseudoaneurysm of the internal carotid artery: diagnosis and endovascular therapy. Laryngoscope. 1998;108(3):326–331. doi: 10.1097/00005537-199803000-00004. [DOI] [PubMed] [Google Scholar]
- 22.Toursarkissian B Allen B T Petrinec D et al. Spontaneous closure of selected iatrogenic pseudoaneurysms and arteriovenous fistulae J Vasc Surg 1997255803–808., discussion 808-809 [DOI] [PubMed] [Google Scholar]
- 23.Charbel F T Gonzales-Portillo G Hoffman W Cochran E Distal internal carotid artery pseudoaneurysms: technique and pitfalls of surgical management: two technical case reports Neurosurgery 1999453643–648., discussion 648-649 [DOI] [PubMed] [Google Scholar]
- 24.Kachhara R, Menon G, Bhattacharya R N. et al. False aneurysm of cavernous carotid artery and carotid cavernous fistula: complications following transsphenoidal surgery. Neurol India. 2003;51(1):81–83. [PubMed] [Google Scholar]
- 25.de Souza J M, Domingues F S, Espinosa G, Gadelha M. Cavernous carotid artery pseudo-aneurysm treated by stenting in acromegalic patient. Arq Neuropsiquiatr. 2003;61(2B):459–462. doi: 10.1590/s0004-282x2003000300025. [DOI] [PubMed] [Google Scholar]
- 26.Bavinzski G, Killer M, Knosp E, Ferraz-Leite H, Gruber A, Richling B. False aneurysms of the intracavernous carotid artery—report of 7 cases. Acta Neurochir (Wien) 1997;139(1):37–43. doi: 10.1007/BF01850866. [DOI] [PubMed] [Google Scholar]