

Abstract
Central cementifying fibroma is a bony tumor, which is believed to be derived from the cells of the periodontal ligament. Central cemento-ossifying fibroma behaves like, a benign bone neoplasm. This bone tumor consists of highly cellular, fibrous tissue that contains varying amounts of calcified tissue resembling bone, cementum, or both. Central cemento-ossifying fibromas of the mandible are common; however, they are rare in the maxilla region. This tumor is most frequent between 35 and 40 years of ages. In this report we have described a 37-year-old male with cemento-ossifying fibroma of the maxilla region with the mass that had been appeared 2-3 months prior to his first referral. Radiologic imaging such as intra-oral, panoramic, and Cone Beam CT had been performed. Histological analysis was done and finally diagnosis of central cementifying fibroma was made. The postoperative follow up at 12 months revealed no recurrence.
Keywords: Central cementifying fibroma, fibro-osseous lesions, ossifying fibroma, radiology
INTRODUCTION
In 1971, World Health Organization (WHO) categorized four types of cementum-containing lesions: Fibrous dysplasia, ossifying fibroma, cementifying fibroma, and cemento-ossifying fibroma. According to the latest WHO categorization, benign fibro-osseous lesions in the oral and maxillofacial regions were divided into two categories, osteogenic neoplasm and non-neoplastic bone lesions; cementifying ossifying fibroma belonged to the former category. However, the term “cementifying ossifying fibroma” was altered to ossifying fibroma (OF) in the new WHO classification in 2005.[1]
OF is a bony tumor with possible odontogenic origin. It is believed to originate from the cells of the periodontal ligament.[2] This is a layer of fibrous connective tissue surrounding the roots of teeth. It contains multipotential cells that are capable of forming cementum, lamellar bone, and fibrous tissue.[3,4]
The presence of cementum or bone classifies the lesion as cementifying fibroma or OF, respectively, whereas lesions with mixture of both cementum and bone are called cemento-ossifying fibroma.[5]
This tumor generally occurs in young and middle-aged adults, most frequent between 35 and 40 years of ages.[2,6] There is a marked predilection for the female sex, the female:male ratio is 2:1.[6] Central cemento-ossifying fibromas of the mandible are common, but they are unusual in the maxilla.[7]
CASE REPORT
A 37-year-old man was referred to the department of oral and of maxillofacial radiology of dentistry school of Isfahan medical science university. The patient had a chief compliant of pain and swelling in the right maxilla and asymmetry in it [Figure 1]. The patient mentioned that the mass had first appeared 3 months ago and became slightly larger since then. Furthermore, the patient mentioned that he experienced pain in the right side of his face with referral to the right eye and also episodes of blur vision.
Figure 1.
The 37-years old man with a right maxillary enlargement
The intraoral examination demonstrated an enlargement of the buccal maxillary right region, extending to the area of the canine and first premolar. In addition, the patient had a slight swelling at the palatal region [Figure 2]. The swelling was bony hard, non-tender with no fluctuation on manual palpation. The covering mucosa and gingiva had normal color and smooth in texture. The first premolar appeared to have been displaced by the lesion. The first premolar and canine at the right side were positive to thermal testing; percussion and palpation tests were within the normal limits. The needle biopsy did not revealed any sign.
Figure 2.

Photograph of maxillary right region showing buccal and palatal expansion
Radiographic evaluation showed the presence of a lesion extending throughout the maxillary right toberousity and right canine. The margins of the lesion appeared to be well-defined. Bone pattern is radiolucent with a few wispy trabeculae [Figures 3a and b]. The tumor caused displacement of first right premolar with disappearing of its lamina dura. The mass caused expansion in all direction, but the cortical plate of the bone remained intact. The lesion occupied maxillary sinus and expanded its walls outward. Meanwhile a bony partition existed between the walls of the remaining sinus and the mass.
Figure 3.
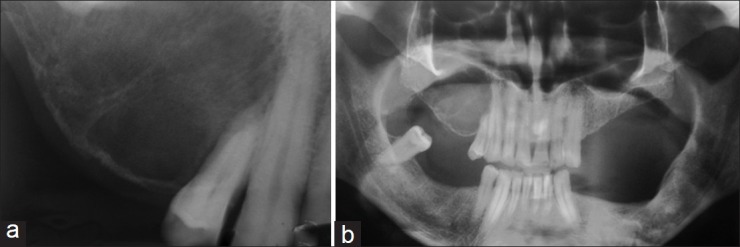
Radiographs, showing the presence of a well-defined radiolucent lesion with a few wispy trabeculae. (a) Periapical, (b) Panoramic images
The CBCT showed a multi locular mass with wispy trabeculaes (similar to the pattern seen on Central Giant Cell Granuloma), occupying and expanding the right maxillary sinus [Figures 4a-c].
Figure 4.

CBCT images showed a large, expansile, well-circumscribed, corticated and multi locular (with wispy trabeculaes) mass involving right maxillary sinus. (a) Axial, (b) Coronal, (c) Tangential
The expansion of Central Ossifying Fibroma into the antrum of the maxilla was convex, which was different from the fibrous dysplasia that its borders are unrecognizable from the antrum.
A comprehensive explanation of treatment was explained to the patient and an informed consent was taken. The tumor was removed under local anesthesia and the gross measures of the specimen were approximately 45 × 30 × 15 mm [Figure 5]. Histological analysis showed a cellular fibroblastic tissue characterized by bundles of collagen densely packed and proliferating fibroblasts. There was presence of spherules of acellular mineralization that resembled dental cementum (cementoid type) [Figures 6a and b]. Diagnosis of central cementifying fibroma was made. The postoperative follow up was favorable, and 1 year later the patient reported no discomfort in the area. A control panoramic X-ray study confirmed good bone regeneration.
Figure 5.

The tumor was removed under local anesthesia and the excised specimen measured 45.30.15 mm
Figure 6.
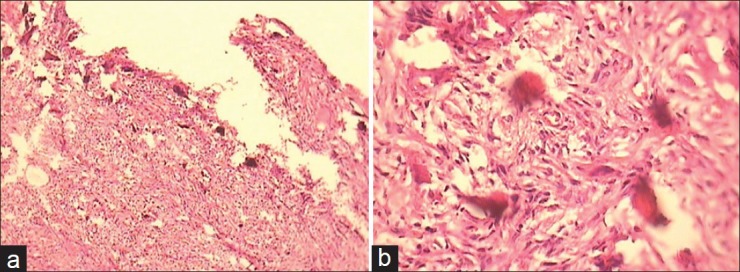
Histological view showing a cellular fibroblastic tissue with spherules of acellular mineralization that resembled dental cementum. (a: Magnification ×10, b: Magnification ×40)
DISCUSSION
COF predominantly affects the craniofacial bone and rarely involves the long bones, among the craniofacial bones; The mandible is the most commonly involved site.[8,9]
COF in the maxilla most often appears in the canine fossa and zygomatic arch area. The clinical features of COF can vary from indolent to aggressive behavior. The disease usually is asymptomatic at the time of discovery.[10]
But growth of COF can produces a noticeable swelling and mild deformity; displacement of teeth may be an early clinical feature.[6] Central cemento-ossifying fibromas are typically solitary and well-defined lesions. In the early stages, it appears as a radiolucent lesion with no evidence of internal radiopacities. As the tumor matures, increasing calcification is obvious and the radiolucent area becomes flecked with opacities until ultimately the lesion appears as an extremely radiopaque mass.[6]
The differential diagnosis includes: Chondrosarcoma or osteosarcoma, fibrous dysplasia, odontogenic cysts, squamous cell carcinomas, calcifying odontogenic cysts (Gorlin cysts), and calcifying epithelial odontogenic tumors (Pindborg tumors). The well-defined border of the central cemento-ossifying fibroma helps differentiate it from the aggressive sarcomas and carcinomas. Fibrous dysplasia has a characteristic “ground glass” appearance not seen in the central cemento-ossifying fibroma. The radiologic differentiation of central COF from Gorlin cysts and Pindborg tumors is difficult; the final diagnosis is based on histologic appearance.[11]
The recommended treatment for this tumor is surgical excision. COF usually “shell out” easily in surgical procedure, but maxillary central COF are more difficult to remove completely than mandibular. This may be attributable to the difference in bone character between the mandible and maxilla and to the available apace for expansion in the maxillary sinus.[2]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Sreenivasan B, Edward JO, Sunil S. Central ossifying fibroma of mandible-A Case Report. OMPJ. 2010. [Last accessed on 2011 Oct 24]. [serial online] 2010 Jan-Jun; 1(1) Available from: http://www.ompj.webs.com/janjun2010articles.htm .
- 2.Tamiolakis DE, Thomaidis VA, Tsamis IO. Cementoossifying fibroma of the maxilla: A case report. Acta Stomat Croat. 2005;39:319–21. [Google Scholar]
- 3.Bertrand B, Eloy P, Cornelis JP, Gosseye S, Clotuche J, Gilliard C. Juvenile aggressive cement-ossifying fibroma: Case report and review of the literature. Laryngoscope. 1993;103:1385–90. doi: 10.1288/00005537-199312000-00013. [DOI] [PubMed] [Google Scholar]
- 4.Hamner JE, 3rd, Lightbody PM, Ketcham AS, Swerdlow H. Cemento-ossifying fibroma of the maxilla. Oral Surg Oral Med Oral Pathol. 1968;26:579–87. doi: 10.1016/0030-4220(68)90341-1. [DOI] [PubMed] [Google Scholar]
- 5.Khanna MA, Buddhavarapu SH, Hussain AK, Amir EM. Cemento-ossifying fibroma of paranasal sinus presenting acutely as orbital cellulitis. J Radiol Case Rep. 2009;3:18–25. doi: 10.3941/jrcr.v3i4.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sarwar HG, Jindal MK, Ahmad SS. Cemento-ossifying fibroma: A rare case. J Indian Soc Pedod Prev Dent. 2008;26:128–31. doi: 10.4103/0970-4388.43195. [DOI] [PubMed] [Google Scholar]
- 7.Sarita M, Raj KA, Daya SM, Rohtas KY. Cemento-ossifying Fibroma of the Maxilla. Indian J Radiol Image. 2000;10:103–4. [Google Scholar]
- 8.Liu Y, Wang H, You M, Yang Z, Miao J, Shimizutani K, et al. Ossifying fibromas of the jaw bone: 20 cases. Dentomaxillofac Radiol. 2010;39:57–63. doi: 10.1259/dmfr/96330046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Eversole LR, Leider AS, Patel MF. Ossifying fibroma: A clinicopathologic study of sixty-four cases. Oral Surg Oral Med Oral Pathol. 1985;60:505–11. doi: 10.1016/0030-4220(85)90239-7. [DOI] [PubMed] [Google Scholar]
- 10.White ST, Pharoah MI. 6th ed. Missouri: Mosby Elsevier; 2009. Oral radiology principles and interpretation. [Google Scholar]
- 11.Kuta AJ, MacDonald W, Kaugars GE. Central cementoossifying fibroma of the maxillary sinus: A review of six cases. AJNR Am J Neuroradiol. 1995;16:1282–6. [PMC free article] [PubMed] [Google Scholar]