

Abstract
Background:
Cross- sectional tomograms have been used for optimal pre-operative planning of dental implant placement. The aim of the present study was to assess the accuracy of Cone Beam Computed Tomography (CBCT) measurements of specific distances around the mandibular canal by comparing them to those obtained from Multi-Slice Computed Tomography (MSCT) images.
Materials and Methods:
Ten hemi-mandible specimens were examined using CBCT and MSCT. Before imaging, wires were placed at 7 locations between the anterior margin of the third molar and the anterior margin of the second premolar as reference points. Following distances were measured by two observers on each cross-sectional CBCT and MSCT image: Mandibular Width (W), Length (L), Upper Distance (UD), Lower Distance (LD), Buccal Distance (BD), and Lingual Distance (LID). The obtained data were evaluated using SPSS software, applying paired t-test and intra-class correlation coefficient (ICC).
Results:
There was a significant difference between the values obtained by MSCT and CBCT measurement for all areas such as H, W, UD, LD, BD, and LID, (P < 0.001), with a difference less than 1 mm. The ICC for all distances by both techniques, measured by a single observer with a one week interval and between 2 observers was 99% and 98%, respectively. Comparing the obtained data of both techniques indicates that the difference between two techniques is 2.17% relative to MSCT.
Conclusion:
The results of this study showed that there is significant difference between measurements obtained by CBCT and MSCT. However, the difference is not clinically significant.
Keywords: Cone beam computed tomography linear measurements, multi-slice computed tomography
INTRODUCTION
Radiography has been performed to evaluate the quantity, quality, and morphology of the remaining alveolar bone at the recipient site of dental implant and surrounding anatomical structures, particularly the positions of the mandibular canal.[1] Neither intraoral nor panoramic radiographs give the three-dimensional information of the imaged area needed for optimal preoperative planning of dental implant placement. Different cross-sectional tomograms, MSCT and, more recently, CBCT examination have been used for this purpose.[2,3]
MSCT involves simultaneous translatory movement of the patient while the X-ray tube and the detector rotate around the gantry axis. This allows continuous data acquisition, image reconstruction, and archiving as the entire volume of interest is scanned. However, MSCT has certain limitations such as high radiation dose, high cost, and limited availability of the procedure. In an attempt to overcome the limitation of MSCT, CBCT devices have been developed specifically for use in the maxillofacial area. CBCT uses a cone-shaped X-ray beam and a more restricted field of view (FOV) than MSCT. The benefits of CBCT are lower costs, smaller device size, and lower radiation dose than MSCT.[4,5,6] Of the studies conducted in this field, the one investigated by Kamburoglu, et al. can be pointed out, in which they reported that linear measurements on CBCT images revealed similar values to real ones.[7]
The aim of the present study was to assess the accuracy of cone beam CT measurements of specific distances around the mandibular canal by comparing them to those obtained from MSCT images made on a 64-slice scanner.
MATERIALS AND METHODS
This experimental laboratory study was performed in the Department of Oromaxillofacial Radiology and Torabinejad Research Center of Isfahan University of Medical Sciences Isfahan, Iran, during the academic year 2011. Ten formalin-fixed donated hemi-mandible specimens (5 right side and 5 left side), which were provided by the Department of Anatomy were used. Mandibles with a history of trauma were not included in the study. Before imaging, orthodontic wires were placed at 7 locations between the anterior margin of the third molar and the anterior margin of the second premolar as reference points. Therefore, in every hemi-mandible, 7 areas were determined to prepare cross-sectional slices and led to preparing a total of 70 cross-sectional images of 70 areas. CBCT images were acquired with the CBCT unit (GalileosSirona Dental system charlotte siemens, Germany). The equipment was operated at 10 mA and 85 KVP. The scan time was 14 seconds. The X-ray detector consisted of a 9-inch image intensifier and a charge-coupled device camera. The fixed field of view (FOV) was 15 cm resulting in a scan volume of 15 × 15 × 15 cm and the voxel size was 0.3 × 0.3 × 0.3 mm. Mandibles were fixed and submerged in a plastic box full of water for beam attenuation and stabilized on a stand that was free from any metallic parts. The anterior symphyseal region of the mandible was in front of chin holder and vertical laser used to position the mandible until the mid-sagittal plane was perpendicular to the floor and the horizontal laser reference coincided with the posterior alveolar ridge[8] [Figure 1]. The reconstructed axial projection images were processed with reformatting software GALAXIS to obtain transverse cross-sectional images of the mandible at the sites of orthodontic wires. All acquired images were burnt on high quality CDs.
Figure 1.

Hemi-mandibule and its position in the CBCT unit
After imaging, the following distances were measured on each cross–sectional cone-beam CT image [Figure 2]: tW, i.e. the longest axis in the bucco-lingual direction of each section; L, i.e. the longest axis in the apico-basal direction of each section; UD, i.e., the distance between the top of the canal and the top of the alveolar ridge; LD, i.e. the distance between the bottom of the canal and the base of the mandible; BD, i.e. the distance between the anterior-most point of the canal and the perpendicular point on the buccal margin of the mandible; and LID, i.e., the distance between the posterior-most point of the canal and the perpendicular point on the lingual margin of the mandible. All distances were recorded in millimeters by two trained, independent oral radiologists. The measurements were recorded directly from the computer monitors in the mornings. The mandibles were also imaged by a MSCT scanner (Siemens Somatom Sensation 64 slice, Germany) in Milad Hospital during the academic year 2011, using the same protocol routinely used in clinical practice. Axial sectional images were acquired with the scanning plane for the mandibles parallel to the long axis of the body of the mandible [Figure 3]. The sectional images were acquired with 80 mA and 120 KV.[2] The raw data were reformatted with reformatting software to obtain transverse cross-sectional images. The same distances were measured on the corresponding cross-sectional MSCT images using measurement Syngo software. Reproducibility of measurements was assessed by having each observer separately repeat both MSCT and CBCT measurements after one week interval to eliminate memory bias.
Figure 2.
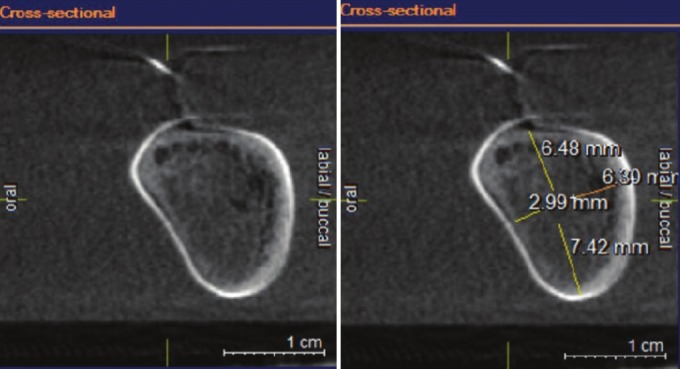
CBCT cross-sectional images
Figure 3.
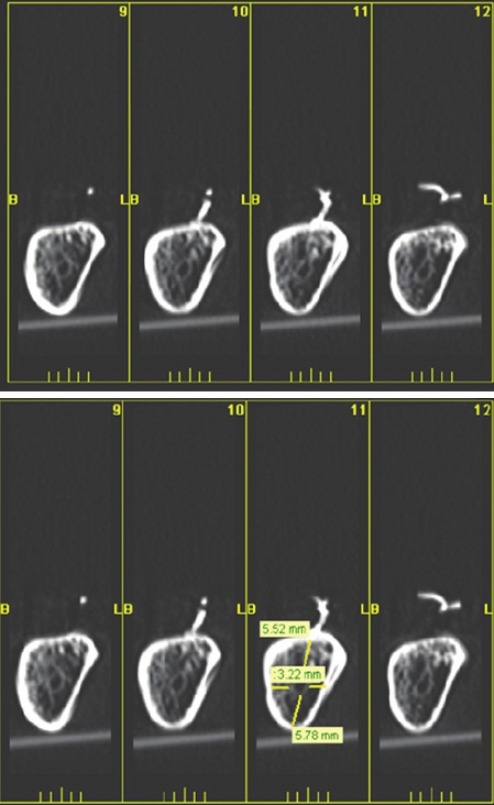
MSCT cross-sectional images
In total, 840 measurements were recorded (6 distances were measured at 7 sections on 10 specimens, for 420 measurements per observer per reading per technique). The obtained data were evaluated using SPSS software, applying paired t-test and ICC.
RESULTS
The paired t-test showed that there was a significant difference between the values obtained by MSCT and CBCT measurement techniques for all areas under investigation such as H, W, UD, LD, BD, and LID, (P < 0.001), with a difference of less than 1 mm.[9]
ICC was 98% and P value was 0.001 for all measurements, using ICC for the measurement of two observers for both MSCT and CBCT techniques. Regarding a high ICC for both techniques, the mean value was calculated for the measurements by two observers and the data was reported as a single value. The calculated ICC for all distances by both techniques, measured by a single observer with a one week interval was 99%. Comparing the obtained data of both techniques indicate that the differences between two techniques is 2.17% relative to MSCT [Table 1].
Table 1.
The average data obtained by CBCT and MSCT techniques, the difference and the average error percentage for the techniques

DISCUSSION
In general, MSCT equipment has been proven to be a precise tool to measure the distance between skeletal structure parts. Previous studies showed that the accuracy of linear measurements obtained by CBCT is comparable to the measurements by MSCT, which is considered as a gold standard.[9] In addition to close consistency between the two techniques, the values reported by two observers during two weeks were also correlated. The previous studies on CBCT were focused on the accuracy of linear distances of marked points. In a study, the accuracy of linear measurement of obtained images by CBCT was compared to real values and indicated that the average of difference percentage is 2.31%. The significant statistical difference is not clinically valuable so the result is similar to the results of our study (1/7%).[10]
In another study, the accuracy of linear measurements from CBCT with different numbers of basic images was compared to real values. In this study, the average of difference percentage for many measurements was reported less than 5%, which is almost consistent with values obtained from our study (2.17%). The study also showed that the accuracy of measurements obtained from three dimensional images, regardless of the number of required basic images for recreating a better quality image, were not significantly different in comparison to real values.[11]
In a study, the accuracy of measurements from two dimensional images of CBCT was measured with different positions of dried skulls. The accuracy was not significantly different in different skull positions.[12]
In some of the studies, the accuracy of linear measurements from CBCT images was compared to real value and the differences were less than 1 mm and the average of difference percentage was 2.3%, which was consistent with the results of our study.[2,13]
Today, it has been recognized that dimensional accuracy of cross-sectional tomograms to measure the above mentioned distance, with measurement error of 1 mm is admittable for assessing the implant location.[14]
In another study, the accuracy of two CBCT imaging systems (New Tom and CB Mercuray) was compared and the average of difference percentages was reported as less than 0.19%, which is not consistent with values obtained by our study (2.1%). This inconsistency could be due to comparing the measurements by CBCT with those obtained by MSCT and not with real values.[15]
In a study, the linear measurements by two techniques (CBCT and MSCT) on dried skulls were compared. There was no significant difference between observers and MSCT and CBCT techniques. There was a significant statistical difference in this study, which could be due to available equipment, related software, and accuracy of observers. Regarding the mentioned point, the difference was not clinically significant.[16]
Another study showed that measurements of crown width of unerupted teeth in CBCT images were significantly larger than real measurements, which were consistent with our study results. However, differences were not clinically significant.[17]
In other studies, the measurements by CBCT images compared to measurements using dried skulls showed underestimated measurements by CBCT, which is inconsistent with results of the present study. In this study, the measurements which were obtained by CBCT have higher values than ones by MSCT which can be due to the fact that measurements were done by different types of equipment and software.[18,19]
In a study, linear measurement accuracy obtained by CBCT images was compared to real values. The results showed that there was no significant statistical difference between the values by CBCT and real values, which was not consistent with results of the present study. The present study showed a significant difference but the difference was not clinically significant. The inconsistency could be due to difference between CBCT equipment and their image receptors. Image transfer from computer memory to CD, leads to compacting data and losing some image data.[20] In this study, the measurements by CBCT were a little higher than MSCT that it may be because of scattered radiation caused by the metallic orthodontic band used in this study.
CONCLUSION
Based on the findings of the present study, there is a considerable difference between measurements obtained by CBCT and MSCT. However, the difference is not clinically significant. Considering the lower exposure and cost of CBCT it can be used instead of MSCT for linear measurement in implant placement.
Footnotes
Source of Support: This study has been financially supported by Isfahan University of Medical Sciences. (Project code 390020)
Conflict of Interest: None declared
REFERENCES
- 1.Hanazawa T, Sano T, Seki K, Okano T. Radiologic measurements of the mandible: A comparison between CT-reformatted and conventional tomographic images. Clin Oral Implants Res. 2004;15:226–32. doi: 10.1111/j.1600-0501.2004.00991.x. [DOI] [PubMed] [Google Scholar]
- 2.Suomalainen A, Vehmas T, Kortesniemi M, Robinson S, Patola J. Accuracy of linear measurents using dental cone beam and conventional multislice computed tomography. Dentomaxillofac Radiol. 2008;37:10–7. doi: 10.1259/dmfr/14140281. [DOI] [PubMed] [Google Scholar]
- 3.Marmulla R, Wörtche R, Mühling J, Hassfeld S. Geometric accuracy of theNewTom 9000 Cone Beam CT. Dentomaxillofac Radiol. 2005;34:28–31. doi: 10.1259/dmfr/31342245. [DOI] [PubMed] [Google Scholar]
- 4.Al-Ekrish AA, Ekram M. A comparative study of the accuracy and reliability of multidetector computed tomography and cone beam computed tomography in the assessment of dental implant site dimensions. Dentomaxillofac Radiol. 2011;40:67–75. doi: 10.1259/dmfr/27546065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kobayashi K, Shimoda S, Nakagawa Y, Yamamoto A. Accuracy in measurement of distance using limited cone-beam computerized tomography. Int J Oral Maxillofac Implants. 2004;19:228–31. [PubMed] [Google Scholar]
- 6.Scarfe WC, Farman AG, Levin MD, Gane D. Essentials of maxillofacial cone beam computed tomography. Alpha Omegan. 2010;103:62–7. doi: 10.1016/j.aodf.2010.04.001. [DOI] [PubMed] [Google Scholar]
- 7.Kamburoglu K, Kilic C, Ozen T, Yuksel SP. Measurements of mandibular canal region obtained by cone beam computed tomography: Cadavric study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:e34–42. doi: 10.1016/j.tripleo.2008.10.012. [DOI] [PubMed] [Google Scholar]
- 8.Berco M, Rigali PH, Jr, Miner RM, DeLuca S, Anderson NK, Will LA. Accuracy and reliability of linear cephalometric measurements from cone-beam computed tomography scans of a dry human skull. Am J Orthod Dentofacia lOrthop. 2009;136:17.e1–9. doi: 10.1016/j.ajodo.2008.08.021. [DOI] [PubMed] [Google Scholar]
- 9.Monsour PA, Dudhia R. Implant radiography and radiology. Aust Dent J. 2008;53(Suppl 1):S11–25. doi: 10.1111/j.1834-7819.2008.00037.x. [DOI] [PubMed] [Google Scholar]
- 10.Periago DR, Scarfe WC, Moshiri M, Scheetz JP, Silveira AM, Farman AG. Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod. 2008;78:387–95. doi: 10.2319/122106-52.1. [DOI] [PubMed] [Google Scholar]
- 11.Brown AA, Scarfe WC, Scheetz JP, Silveira AM, Farman AG. Linear accuracy of cone beam CT derived 3D images. Angle Orthod. 2009;79:150–7. doi: 10.2319/122407-599.1. [DOI] [PubMed] [Google Scholar]
- 12.Ludlow JB, Davies – Ludlow LE, Brooks SL. Dosimetry of two extra Oral direct digital imaging devices: New Tom cone beam CT and orthophos plus DS Panoramic unit. Dentomaxillofac Radiol. 2003;32:229–34. doi: 10.1259/dmfr/26310390. [DOI] [PubMed] [Google Scholar]
- 13.Lagravère MO, Carey J, Toogood RW, Major PW. Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2008;134:112–6. doi: 10.1016/j.ajodo.2006.08.024. [DOI] [PubMed] [Google Scholar]
- 14.Ekestubbe A, Gröndahl K, Gröndahl HG. Quality of preimplant low-dose tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:738–44. doi: 10.1016/s1079-2104(99)70018-1. [DOI] [PubMed] [Google Scholar]
- 15.Stratemann SA, Huang JC, Maki K, Miller AJ, Hatcher DC. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol. 2008;37:80–93. doi: 10.1259/dmfr/31349994. [DOI] [PubMed] [Google Scholar]
- 16.Loueble M, Van Assche N, Carpentier K, Maes F, Jacobs R, van Steenberghe D, et al. Comparative localized linear accuracy of small-field cone-beam CT and multislice CT for alveolar bone measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:512–8. doi: 10.1016/j.tripleo.2007.05.004. [DOI] [PubMed] [Google Scholar]
- 17.Sakabe J, Kuroki Y, Fujimaki S, Nakajima I, Honda K. Reproducibility and accuracy of measuring unerupted teeth using limited cone beam x-ray CT. Dentomaxillofac Radiol. 2007;36:2–6. doi: 10.1259/dmfr/65418489. [DOI] [PubMed] [Google Scholar]
- 18.Baumgaertel S, Palomo JM, Palomo L, Hans MG. Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofacial Orthop. 2009;136:19–25. doi: 10.1016/j.ajodo.2007.09.016. [DOI] [PubMed] [Google Scholar]
- 19.Lascala CA, Panella J, Marques MM. Analysis of the accuracy of linear measurements obtained by cone beam Computed tomography (CBCT-NewTom) Dentomaxillofac Radiol. 2004;33:291–4. doi: 10.1259/dmfr/25500850. [DOI] [PubMed] [Google Scholar]
- 20.Moreira CR, Sales MA, Lopes PM, Cavalcanti MG. Assessment of linear and angular measurements on three-dimensional cone-beam computed tomographic images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:430–6. doi: 10.1016/j.tripleo.2009.01.032. [DOI] [PubMed] [Google Scholar]