

Abstract
Background:
In the northern states, there is hardly any scientific study except road traffic accidents (RTAs) statistics obtained by the Ministry of Home whereas the main way of transportation is by road. There is the increasing load of motor vehicles on the already dilapidated roadways which has resulted in the increasing trend of RTAs in Assam.
Objectives:
To find out the prevalence, probable epidemiological factors and morbidity and mortality pattern due to RTAs in Dibrugarh district.
Materials and Methods:
Descriptive study was carried out in Dibrugarh district from September 1998 to August 1999 under the department of Community Medicine. The information was collected from Assam Medical College and Hospital and cross checked with the police report. A medical investigation including interview, clinical and radiological investigation was carried out; in case of fatality, post-mortem examination was examined in details. An on the spot investigation was carried out in accessible RTAs to collect the probable epidemiological factors.
Results:
RTAs affected mainly the people of productive age group which were predominantly male. Majority of the RTAs were single vehicle accidents and half of the victims were passengers. Accident rate was maximum in twilight and winter season demanding high morbidity and mortality. Head and neck, U.limb and L.limb were commonly involved.
Conclusion:
RTAs is a major public health problem in Assam which needs more scientific study.
Keywords: Abbreviated injury scale, injury severity score, lower limb, road traffic accidents, upper limb
Introduction
The morbidity and mortality patterns are changed due to health and the consequent demographic transition. The health system has to face the double burden of disease as a result of the epidemiological transition including communicable as well asnon-communicable diseases like-cerebrovascular diseases, cardiovascular diseases, neuropsychiatric condition, malignant neoplasm, injuries etc., All types of Injuries like road traffic Injuries, interpersonal violence (IPV), war and self inflation injuries etc., are large and neglected health problem in all regions, accounting fivemillions persons died in 2000. It accounts for (12%) of global burden of disease worldwide. In 2000, an estimated 1.26 million people worldwidedied as a result of Road traffic injuries. 90% of all road traffic injuries death occurred in low and middle income countries. The injury related disease burden is expected to raise over the next 20 years particularly in case of road traffic injuries, IPV, war and self inflation injuries. For adult men aged 15-44 years road traffic accidents (RTAs) are the biggest cause of ill health and premature death worldwide.(1)
In India, 11% of deaths due to non-communicable diseases are due to injuries and 78% of injury deaths are due to RTAs. The Indian Council of Medical Research (ICMR) study on “Causes of Death by Verbal Autopsy” has revealed that injury rank among the first five major cause of death in adults. It is the leading cause of mortality for young adults less than 45 years and a major burden of disease across all age group.(2)
In India, there are some urban based studies of RTAs. In the northern states, there is hardly any scientific study except RTAs statistics obtained by the Ministry of Home. In Assam, the main way of transportation is by road. Due to the changing socioeconomic scenario of the state, the need for rapid movement of a large section of the people is increasing day by day. There is the increasing load of motor vehicles on the already dilapidated roadways which has resulted in the increasing trend of RTAs in Assam. Assam is also a state experiencing double burden of the disease. It is reeling with epidemics like Malaria (contributing >5% of total malaria cases)(3) JE, Gastroenteritis with high infant (66/1000 live birth) and maternal mortality rates (490/1 laces live birth)(4) and over and above there is anincreasing trend of chronic diseases like Hypertension, Diabetes and its consequent accompanying episodes of Cardiovascular, Cerebrovascular emergency and Cancers. In the state of Assam according to the data available it was found that about 34.9% of the male population smoke tobacco while a high rate of 48.2% chew tobacco. Injury was one of the commonest morbidity (14%) that has to be dealt by the emergency response service.(3)
A study has been carried out in Forensic Medicine (FSM) department of Guwahati Medical College, Assam which found that 23.84% of all autopsies were due to RTAs victims.(5) In emergency related services, provided by NRHM, Assam using MRITUNJOY 108-Injury related health problem 13%(mostly RTAs), occupying 3rd rank next to pregnancy related (35%) and acute abdomen (15%) during the period from Nov. 2008 to June 2010.(6)
In 2007, State Assembly of Assam recorded 4403 nos. of RTAs, which injured 5697 persons and killed 1604 case.(7)
The health infrastructure of the region was established to deal with the common morbidities as per the national priority like RCH and control of different Communicable diseases. To deal with these morbidities valuable resources of the existing health institution has to be diverted. RTA is another emerging morbidity in a developing state like Assam which is not only siphoning off a large chunk of specialist man hour as well as other valuable resources of the health services. As such to plan the services properly we must have an idea of its magnitude as well as the type of service requirement for those affected by RTA. With this backdrop, the current study was conducted with the objectives of finding out the magnitude of problem, its epidemiological factors and morbidity and mortality pattern due to RTAs in a district of Assam.
Materials and Methods
This was a descriptive study, conducted in Dibrugarh district is situated in upper Zone Assam, one of the seven north-eastern states India. Dibrugarh district is one of the twenty seven districts of Assam. Almost all the districts of Assam including Dibrugarh are situated in plain (96.24%) except North Cachar and Karbi Anglong hill districts. In all the places, November to January is the winter season with heavy fog except on daylight and the monsoon season start in the month of April/June for period ofthree to four months. The road condition is almost similarand the mean population density of the state is 340 persons/sq km (2004) which is almost same with the study district (351 persons/sq.km). The district wise mean length of P.W.D road is 1405 km as against 1309 km in the study area. Mean employee of the state registered through exchange is 68178 persons (2003) which is less than the study area (95759). Each district has a similar type of health infrastructure in the Govt. sector-i.e., sub centre, PHC, CHC and district level hospital. The private health facility is located mainly in the urban area. Mean nos. motor vehicle accident (2003) is 130.48 as against 155 in Dibrugarh district (Crime branch).
The population of the district is 11, 85072 (2001), having rural: Urban ratio 4.18:1. There are six urban areas, the population density is 351 persons per sq. km, the total surface area is 3,381 sq. km. The total length of the road is 1309 km, where the National Highway 74 km, State Highway 96 km and other P.W.D roads 1139 kms. There are six nos. of Block P.H.Cs and five nos. of C.H.Cs in the district. Assam Medical College and Hospital, Dibrugarh is situated in the outskirt that provides the secondary and tertiary level services in the Government Sector. The numbers of police station and outpost in the district are 14 and 6 respectively (1994-95). There are 66,907 nos. of registered motor-vehicles in the district.
The study was conducted from September 1998 to August 1999 in Dibrugarh based on the following valid assumption: a) All the RTAs requiring hospitalisation likely to attend the Casualty/O.P.D. in a Govt. Health Care institution to avail the round the clock specialised service b) The cases are of medico legal. c) In case of death, a post-mortem examination is carried out in all cases. Any RTAs occurring in Dibrugarh district were included in the study. There are multiple sources of event registration i.e., Emergency ward, O, P, D., F.S.M. Department, Police Station, MVI office, Newspaper, eye witnesses etc., The term RTAs (i.e., road traffic accidents) included the Motor Vehicle Traffic and Road Vehicle Accidents.
The information of injuries related to RTAs were collected regularly from the Casualty, O.P.D and F.S.M department of Assam Medical College and Hospital in a standard proformaand cross checked with the police report. After this, a medical investigation including interview, clinical and radiological investigation was carried out; in case of fatality, post-mortem examination was examined in details. An on the spot investigation of 85% of accidents was carried out following the accident, otherwise required information was collected from the above mentioned sources mainly from the eye witness and confirm the veracity of the information. These information included-vehicle designs, driver status and other environmental factors like roads, weather etc., The injury regions were described according to the anatomical sites i.e., Head and neck, U.limb, L.limb, Chest, Abdomen and Perineum. Injury severity were quantified using the abbreviated injury scale (AIS)14 and described as mean AIS of the above body regions in injured and fatal cases - i) Minor injury - AIS 1-2. ii) Moderate injury - AIS 3. iii) Severe injury - AIS > 4. All the extremities were related on a scale AIS 1-3. Thus a moderate (AIS = 3) extremity injury by definition was the most severe level of extremity injury.
Results
Magnitude of problem: The study showed the prevalence of RTAs 39.04 per 100000 populations, injury rate 55.60 per 100000 populations and mortality rate 5.48 per 100000 populations.
In this study, the total 463 RTAs occurred which caused 659 (91%) injury and 65 (9%) death.
The mean age of affected persons is 31 years with male: Female ratio 7.13:1 (male 88%). More than two-third (73%) of victims are in the age group of 15-44 years. Only 10% victims are under 15 years of age group.
Age and sex distribution of the injured cases is displayed in Figure 1.
Figure 1.
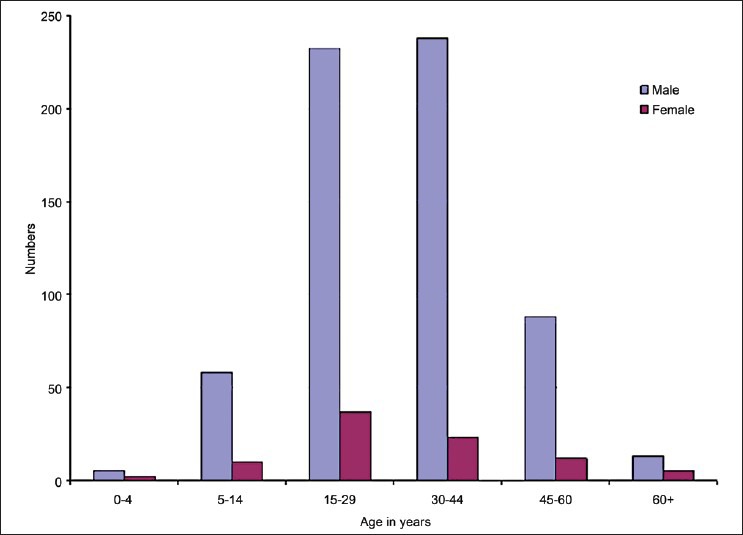
Age and sex distribution of the injured cases
The accident rates are 35 RTAs/100kms/yr and 7 RTAs/1000 vehicles/yr.
The single vehicle accident (self accident or non-collision type) comprises 42% of all the RTAs. 34% accidents are collision type and almost one quarter (24%) of accidents involves the pedestrian. The single vehicle accident is mostly caused by M.Cycle (19%) and M.Car (17%). 3/4 of the pedestrian accident is caused by M.Car (18%), followed by M.Cycle (4.5%).
Seasonal trend of RTAs is displayed in Figure 2.
Figure 2.
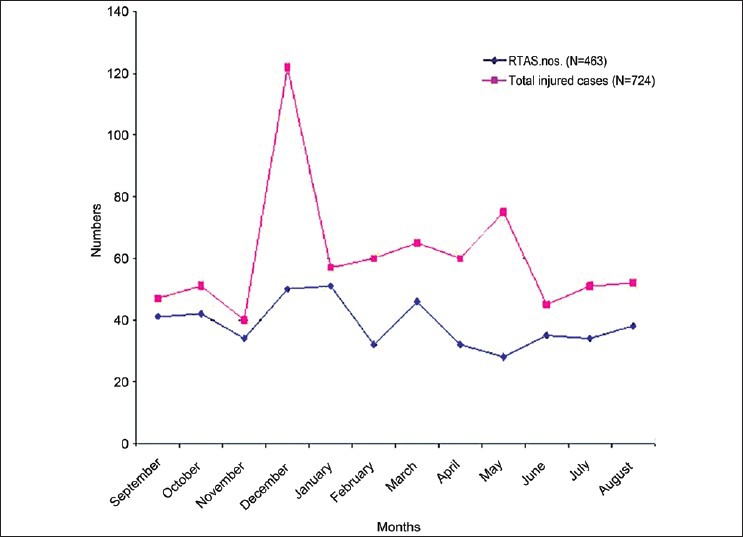
Seasonal trend of RTAs
RTAs are marginally increased in the month of December and January (P > 0.05) but the nos, of injured (fatal and non fatal) are increased in the month of December (P < 0.05, statistically significant). The accident (nos./hr) is maximum (50%) in twilight (light phase of night), followed by day light (34%) and dark phase of light (16%).
89% drivers are in the age group of 15-44 years, 15% have no licence and nobody used seat belt, 19% had consumed alcohol during the previous 24 hrs of driving.
The study has shown that head and neck (66%) is commonly involved in an accident, followed by upper and lower limb (44% and 41% respectively). The least affected sites are chest (14%), abdomen (3%) and perineum (1.5%).
Types of injury combination are shown in Figure 3.
Figure 3.
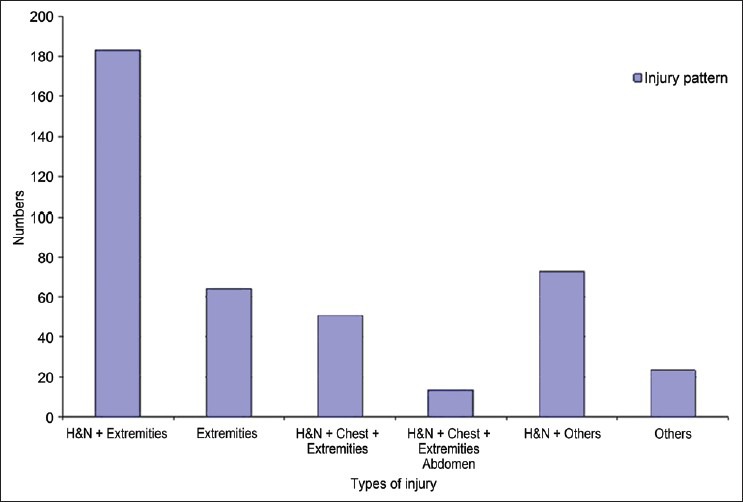
Types of injury combination
Most common injury patterns are head and neck with extremities (45%) followed by extremities (15%) and head and neck + chest + abdomen (12%). The study has shown that head and neck is the most severely affected site (mean AIS 2.2) followed by chest and abdomen.
Discussion
In this study, the magnitude of problems is i.e. prevalence of RTAs 39.04 per 100000 populations, injury rate 55.60 per 100000 populations and mortality rate 5.48 per 100000 populations.
According to State Assembly report-2007, magnitude of prevalence of RTAs are16.55 per 100000 populations, injury rate 21.41 per 100000 populations and mortality rate 6.03 per 100000 populations.(7)
The prevalence rate and injury rate of RTAs are not similar which may be due to different methodology in recording system of RTAs. In our study, one of the valid assumptions was that all the cases are medico legal in nature, so invariably will be recorded in the police dept but practically it was evident that many minor injury and accidents are settled between the parties which are reported to the health facility for treatment purpose only and not recorded as medico legal cases. This may be the reason of lower rate of non-fatal injuries and morbidities reflected in government report. However, it is observed that the case fatality rate has been similar because fatality cases are medico legal and invariably recorded in both health and police department. Moreover this study was conducted during 1998-99 and the magnitude ofproblem has beencompared with the data of 2007. The change of transportation system, health system cannot be denied but still it has relevance because of a compatible fatality rate which is one of the most important outcome of the natural history of RTAs. This study has many limitations in estimating the burden of RTAs, studying the disease epidemiology, using in policy making but undoubtedly it will help to conduct further research study in this relevant field in the remote area of north eastern region.
Singh et al., recorded the trend of RTAs victims from 1999 to 2003 and nos. of RTAs victims were 21.04 to 25.24% amongst all autopsies.(5)
Majority of the victims (73%) are in the productive age (15-44 years) group which are predominantly males (88%). Only 10% victims under 15 years of age group are affected. Some of the particular high risk behaviour like-alcohol consumption, driving in high speed etc., is common in this specific group. So, adult males are commonly involved in RTAs. Similar observation was reported by WHO in the Injury Chart Book. Corresponding findings were reported by Jha et al.,(8) and Patil et al.(9,10)
Swaddiwudhipong et al.,(10,11) also observed a similar trend in the type of RTAs, their results showing single vehicle accident 66.4%, collision type 27.14% accident with pedestrian 6.49%. Frequency of type of RTAs depends on epidemiological factors (i.e., and type of vehicle, footpath, road condition etc). In this study, the variation of these frequencies may be due to the epidemiological factors related to the study. In single vehicle accident, the agent i.e., M. Cycle, a two wheeler motorized vehicle is comparatively unstable in moving condition than three or four wheeler motorized vehicles. The host i.e., motorcyclist which are mainly males have some high risk behaviours like alcohol consumption, driving in high speed etc.
RTAs are increased in the winter season as the drivers have poor adaptability to light in foggy environment. The month of “December” may be regarded as the “month of festival” (picnic, new-year celebration, game competition etc.) during which period the vehicles are driven with alcohol intoxication and transport volumes are increased rapidly. Nos. of vehicles and pedestrians are maximum in day light (school, office hrs.), followed by light phase of light (marketing, recreation hrs.) and dark phase of night (rest hrs.). But the driver and pedestrian have poor adaptability to twilight (light phase of night) for which the accident rate is maximum (50%) followed by daylight (34%) which is due to thick concentration of vehicles and pedestrian in the road.
Wang et al.,(11,12) also observed a similar seasonal trend that accidents were increased in winter month.
In the study area, major portion of road curvature is straight in which the driver drives the vehicle in a relaxed mood. Another peculiarity of this area is that the roads have mostly rough and irregular surface and few smooth surfaces are distributed in between them. The driver has a tendency to increase the speed in the smooth surface of straight road and control of the vehicle is lost when they touch the rough and irregular surface.
Swaddiwudhipong et al.,(10,11) observed that majority of the accident occurred in straight road and only 30.8% in rough surface and 34.9% with high speed. In this study, the frequency of RTAs is different in rough surface and/or with high speed, which may be due to its own epidemiological context (rough surface distribution, traffic legislation etc.)
Swaddiwudhipong et al.,(10,11) observed that 17.1% drivers had no driving licence and 24.3% were alcoholic.
The study has shown that head and neck (66%), upper and lower limb (44% and 41% respectively) are commonly involved followed by chest (14%), abdomen (3%) and perineum (1.5%).
Jha et al.,(8,9) and Patil et al.,(9,10) also showed a similar trend of fracture amongst the injured patient.
In this study, all types of injury (fracture and non-fracture) are included according to the body regions involved. The most active and mobile body parts respond quickly to any stimulus. In an accident similarly, the most active and mobile body part (head and neck, extremities) try to maintain the equilibrium of the body, so they are commonly involved.
In this study, the commonest injury pattern is head and neck with extremities (45%). Istomin(12,13) also described that in road accidents predominant injury sites were head and neck with extremities (35.9%).
In severity category, head and neck is the most severely affected site (mean AIS 2.2) followed by chest and abdomen. All the vital organs of the body are present in head and neck, chest and abdomen, so these regions are severely injured in RTAs.
In a study of child pedestrian injury, Lapidus et al.,(14,15) found a similar pattern of injury severity in body regions.
RTAs in Private Practioner: During the study period, only few organized private health sector was functioning which was not developed to tackle the RTAs emergency and so, they referred to the Assam Medical College, Dibrugarh which is the only secondary and tertiary level hospital in the district.
The study was a preliminary study to assess the magnitude and epidemiology of RTAs but had the limitation like- coverage, on the spot visit of all the RTAs but showed the greater percentage than usual recording system. So, further study is necessary covering more districts to find out the real picture of RTAs in Assam. However, the burden and general pattern of RTA is likely to follow similar pattern as the topography, climatic and road condition, average population and vehicle density, socio-cultural factors (festival celebration, alcohol consumption frequency etc.), poor traffic legislation etc., are more or less similar in all the districts. Still, it is agreed the limitation of the study in estimating the burden of the health problem in the state but definitely it will help to conduct further research study in Assam.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Peden M, McGee K, Sharma G. Geneva: World Health Organization; 2002. The injury chart book: A graphical overview of the global burden of injuries; p. 05. [Google Scholar]
- 2.Shah B, Menon GR. Preface Workshop on development of a feasibility module for road injury surveillance, July 11th-12th. 2006 [Google Scholar]
- 3.NRHM report-Assam, 2008. [Last accessed on 2010 Jul 5]. Available from: www.nrhmassam .
- 4.NFHS-3. [Last accessed on 2010 Jul 5]. Available from: http://www.nrhmassam.in/nfs3.php .
- 5.Singh YN, Bairagi K, Das KC. An epidemiological study of RTAs victims in Medico legal autopsies. J Indian Acad Forensic Med. 2005;27:166–9. [Google Scholar]
- 6. [Last accessed on 2010 Jul 5]. Available from: http//: www.nrhmassam .
- 7. [Last accessed on 2008 Apr 25]. Available from: http://www.indianexpress.com/news/assam .
- 8.State Assembly Record. 2007 [Google Scholar]
- 9.Jha N, Srinivasa DK, Roy G, Jagdish S. Injury pattern amongst road traffic cases: A study from South India. Indian J Community Med. 2003;28:85–90. [Google Scholar]
- 10.Patil SS, Kakade RV, Durgawala PM, Kakade SV. Pattern of road traffic injuries: A study from Western Maharastra. Indian J Community Med. 2008;1:56–7. doi: 10.4103/0970-0218.39248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Swaddiwudhipong W, Nguntra P, Mahasakpan P, Koonchotes S, Tantriratna G. “Epidemiologic characteristics of drivers, vehicles, pedestrians and road environments in road traffic injuries in rural Thailand”. Southeast Asian J Trop Med Public Health. 1994;25:37–44. [PubMed] [Google Scholar]
- 12.Wang ZG, Jiang J. An overview of road traffic trauma research in China. J Traffic Med. 1998;26:25–30. [Google Scholar]
- 13.Istomin GP. Injuries in RTAs: Improvement of the system of prevention rendering of medical aid and treatment of the victims. Ortop Travamatol Protez. 1989;6:1–7. [PubMed] [Google Scholar]
- 14.The Abbreviated Injury Scale: 1985 revision AAAM, deplaines. [Last accessed on 1999 Oct 22]. Available from: http://www.aaam1.org/ais .
- 15.Lapidus G, Braddock M, Banco L, Montenegro L, Hight D, Earniello V. Child pedestrian injury: A population based collision and injury severity profile. J Trauma. 1991;3:1110–5. [PubMed] [Google Scholar]