

Abstract
Background
Nasopharyngeal carcinoma with leptomeningeal involvement is rare and typically has poor prognosis.
Methods and Results
We present a case report of a patient with nasopharyngeal carcinoma who was treated with high-dose intravenous methotrexate and remains asymptomatic and without clinical evidence of disease 6 years later.
Conclusions
Systemic high-dose methotrexate should be evaluated in the treatment of advanced nasopharyngeal carcinoma with central nervous involvement.
Keywords: methotrexate, nasopharyngeal carcinoma, leptomeningeal disease, CNS involvement, high-dose methotrexate
Leptomeningeal metastasis from nasopharyngeal carcinoma (NPC) occurs in fewer than 5% of patients.1-3 However, direct intracranial extension is more common because of the anatomic proximity of the nasopharynx to the skull base, occurring among nearly 17% of patients who present with locoregionally advanced, T4 tumors,4,5 and between 8% and 30% with cranial neuropathies.6-9 Fewer than 10 case reports exist in the literature of patients with NPC and leptomeningeal involvement,3,10 and none reports clinical resolution of neurological deficits. In this report, we describe a patient with extensive involvement of the neuroaxis by tumor who was successfully treated with high-dose intravenous methotrexate. The chemotherapeutic choice of methotrexate was based on its activity in head and neck cancer, reported activity in leptomeningeal disease in solid tumors, and an evolving standard of care for its use as primary therapy in primary central nervous system lymphoma.
CASE REPORT
A 31-year-old white man presented with a 4-month history of progressively worsening headaches, nasal congestion, diplopia, bilateral otalgia and aural fullness, hoarseness, dysphagia, and a 20-pound weight loss.
On physical examination, he had left-sided weakness of cranial nerves V (V2, V3) and VI as well as right-sided X, XI, and XII deficits. Examination was consistent with bilateral conductive hearing loss, a right-sided serous effusion, and a retracted left tympanic membrane. Physical exam was otherwise unremarkable. Fiber-optic nasopharyngoscopy was notable for extensive erosion of the nasopharyngeal roof and fixed right vocal fold.
Axial T1-weighted fat-suppressed MRI revealed an infiltrative mass in the nasopharynx extending into bilateral parapharyngeal spaces (Figure 1, arrow-heads), into the intracranial compartment (Figure 1, arrows) through the clivus with a large dural-based mass anterior to the brain stem. A lumbar puncture revealed no evidence of malignant neoplasm on cytology. A biopsy of the nasopharynx confirmed the diagnosis of nasopharyngeal carcinoma, undifferentiated type (lymphoepithelioma), and positive for Epstein–Barr virus (see Figure 2). The disease was clinically staged IVA, T4N0M0 NPC, WHO type III.
FIGURE 1.
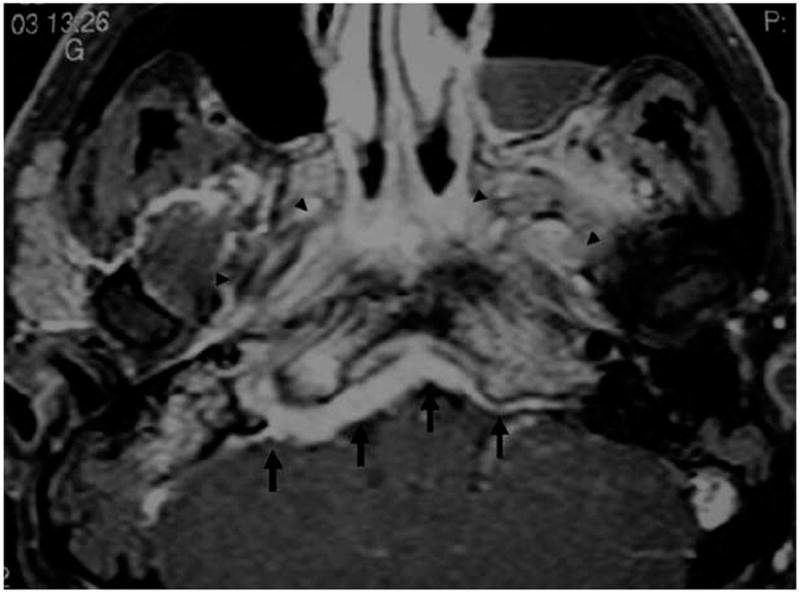
High-resolution axial T1-weighted fat-suppressed MR image shows a large mass in the nasopharynx and bilateral parapharyngeal spaces (arrowheads) that infiltrates the clivus and extends into the intracranial compartment (arrows).
FIGURE 2.
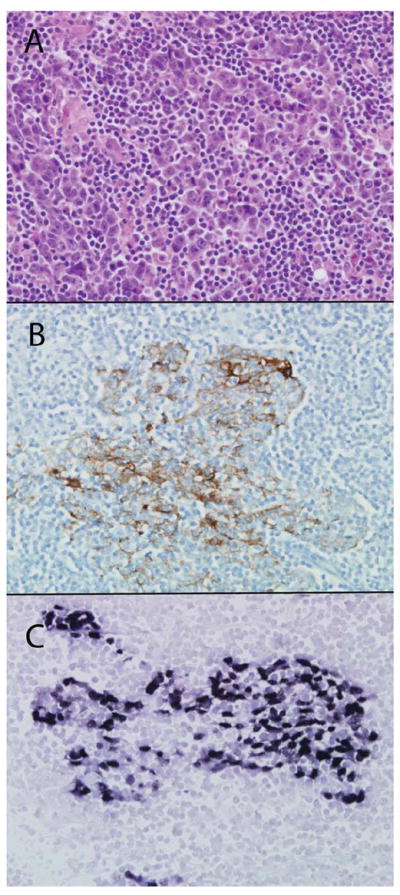
Histopathology of nasopharyngeal biopsy. (A) Hema-toxylin and eosin stain showed irregular cords of nonkeratinized undifferentiated cells within a background of lymphocytes. (B) The tumor cells were immunoreactive for cytokeratin (immuno-histochemical staining for AE1:AE3). (C) In situ hybridization for Epstein–Barr virus (EBV)-encoding RNA was positive for EBV.
The patient was administered 3 cycles of high-dose intravenous cisplatin (100 mg/m2, days 1, 22, and 43) concurrent with standard-fractionation definitive external beam radiation therapy to the nasopharynx (total dose [TD]: 7020 cGy), bilateral necks (TD: 6040 cGy to upper and posterior necks, 5,040 cGy to lower neck/supraclavicular fossa), and skull base boost (TD: 6646 cGy)11 (see Figure 3).
FIGURE 3.
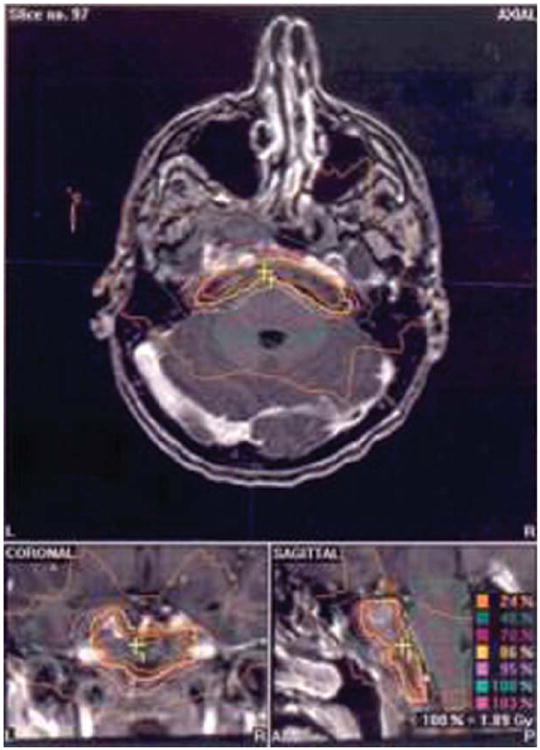
Axial, coronal, and sagittal MR image reconstruction representing stereotactic radiosurgical dose delivery to boost portions of the primary tumor adjacent to normal structures with increased conformality. The cluster of colored isodose lines marked by (+) indicates the dose distribution that spares the brain stem posteriorly and optic chiasm cranially.
After a 3-week break, he received adjuvant cisplatin 60 mg/m2 on day 1 and 5-fluorouracil (5-FU) 750 mg/m2/day on days 1 to 4 every 4 weeks for 3 courses (dose reduced by 20% because of cytopenia). At the end of therapy, the patient had residual radiographic abnormalities at the primary site, although clinically no residual cranial nerve (CN) deficits. CNs II–XII were grossly intact and symmetric. He had no lymphadenopathy.
Approximately 15 months after initial presentation, he complained of anorexia, fatigue, urinary frequency and urgency, constipation, and saddle anesthesia. On examination, sensation was decreased below T10 in the lower abdomen, back, and in bilateral lower extremities. Decreased proprioception and vibratory sensation were noted in lower extremities bilaterally. Strength was 5/5 with normal tone. Patellar reflexes were 2+.
Contrast-enhanced spine MRI revealed multiple intradural and extramedullary nodular enhancing masses throughout the thoracic, lumbar, and sacral spine, consistent with leptomeningeal metastatic foci (see Figure 4). Brain MRI demonstrated a decreased nasopharyngeal mass with resolution of the previously shown intracranial mass and no leptomeningeal disease. Palliative radiation therapy (TD: 3500 cGy/14 fractions) was delivered to a field encompassing the T5–S3 vertebral bodies (Figure 5). Subsequently, high-dose methotrexate (HDMTX; 8 gm/m2 adjusted per measured 24-hour creatinine clearance) was administered intravenously (IV) every 2 weeks for 3 courses to achieve central nervous system (CNS) penetration.12 Therapy was administered on an inpatient basis to prevent precipitation of the chemotherapy in the renal tubules with aggressive hydration, urine alkalynization, and leucovorin rescue. All neurological deficits resolved. On radiographic surveillance 10 months later, a single 4-cm mediastinal lymph node was identified and resected. Pathology was consistent with the original tumor. He was treated with 3 cycles of adjuvant docetaxel 35 mg/m2 on days 1 and 8 and irinotecan 50 mg/m2 on days 1 and 8 of a 21-day cycle. Six years after diagnosis, the patient remains asymptomatic without evidence of recurrent disease.
FIGURE 4.

Sagittal postcontrast T1-weighted image of the thoracic and lumbar spine demonstrates multiple enhancing nodules throughout the intradural extramedullary space that are characteristic of leptomeningeal drop metastases.
FIGURE 5.
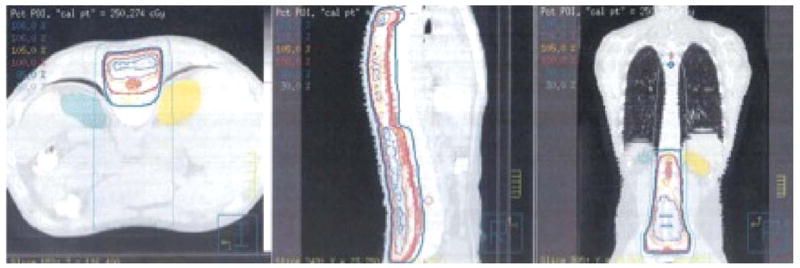
Axial, sagittal, and coronal CT reconstruction representing dose delivery to the spinal axis from T5 to S3.
DISCUSSION
Treatment of leptomeningeal metastatic disease from solid tumors is typically palliative, with median survival of 4 to 6 weeks without treatment.13,14 Radiation therapy is frequently administered to sites of symptomatic or bulky disease to alleviate impairments of cerebrospinal fluid (CSF) flow from extensive CNS involvement, to improve the distribution of intrathecal chemotherapy,15,16 and may improve the quality of life.15
Patients with extensive CNS involvement are frequently treated with palliative intrathecal chemotherapy and have a median survival of approximately 3 to 4 months.17 The goal of intrathecal chemotherapy is to circumvent the blood–brain barrier (BBB) and to expose tumor cells to sufficient concentration of chemotherapy for adequate time. Retrospective analyses have shown that any form of chemotherapy for treatment of CNS disease improves survival.14 Methotrexate, cytarabine (ARA-C), and thiotepa are compatible with intrathecal administration. Randomized controlled trials comparing intrathecal methotrexate with thiotepa17 and methotrexate with ARA-C for the treatment of leptomeningeal metastases from solid tumors have found no difference in survival or toxicity profiles.17 Nevertheless, methotrexate has been considered the first-line agent for treatment of leptomeningeal metastases and has been associated with moderate response rates18,19 and clearance of malignant cells from the CSF in up to 60% of cases.20 A common intrathecal regimen of methotrexate consists of 10 to 12 mg twice per week for 4 weeks followed by weekly administration for 4 to 8 weeks17,21-23 and results in uniform distribution through the neuroaxis.24
Methotrexate has been used as a single agent for treatment of recurrent and metastatic squamous cell carcinoma of the head and neck, with low (<10%) response rates to the traditional regimen of 40 mg/m2/week.25 Randomized trials comparing either moderate or HDMTX (1.5 to 3.0 g/m2/week, IV) to the weekly traditional dose regimen report higher overall response rates (as high as 55%), but no difference in complete response rates or survival.26,27 Although methotrexate has been incorporated into the therapeutic armamentarium for NPC in multiagent chemotherapy, we are unaware of single-agent response data specific to this malignancy.
Intravenous dosing of HDMTX has been established as the standard of care in patients with lymphoma (primary CNS, acute lymphocytic leukemia).28 When administered intravenously, methotrexate enters cells by passive diffusion. Plasma concentration of methotrexate appears to correlate well with CNS concentration, such that higher infusion dose results in similarly elevated CNS concentrations.29
At adequate concentrations, methotrexate is capable of crossing the BBB, although sustaining cytotoxic concentration is dependent on rate, dose, and method of administration. Dosing in the range of 1–7.5 g/m2 (IV) has been found to achieve therapeutic cytotoxic concentrations (1 μM).30 The theoretical advantage of IV administration is that more uniform dose distribution is achievable throughout the CNS than with intrathecal administration.31 Intrathecal dosing initially achieves a peak concentration higher than IV dosing, although higher CSF and systemic concentrations are sustained for up to 6 days with IV dosing.32
When retrospectively compared with intrathecal administration, HDMTX (8 g/m2 every 2 weeks for the first month, followed by additional doses at weeks 4 and 8 in responders) was associated with significantly improved median overall survival (13.8 vs 2.3 months, p = .003) among patients with leptomeningeal disease.32 A pharmacokinetic analysis demonstrated that a lower induction dose of methotrexate (700 mg/m2) prior to a continuous 23-hour infusion (2800 mg/m2) was an effective alternative dosing regimen to achieve adequate CSF concentrations, although clinical outcomes with this regimen have not yet been evaluated in clinical trials.31
Prior to methotrexate, whole brain radiation therapy (WBRT) was the mainstay of treatment for primary CNS lymphoma. WBRT was associated with a median survival of 10 to 14 months and high recurrence rates.33-37 HDMTX (5–8 g/m2) has been used as a monotherapy (±WBRT) and in combination with other chemotherapeutic agents,34,38-40 to achieve 2-year overall survival rates of 51% to 70%.12,41,42 Sequential therapy comprising HDMTX (1–3.5 g/m2) followed by WBRT has resulted in 2-year overall survival of 60% to 85%, with median survival up to 3 years.35,43 Metho-trexate prior to radiation may reduce leukoencephalopathy and limit the effects of radiation-induced limitations of diffusion and efficacy, including BBB restoration, endothelial proliferation, and tumor cell resistance induction.44 Data from phase I and phase II trials have demonstrated methotrexate to be associated with improvement in median survival over WBRT alone; nonetheless, methotrexate in combination with radiotherapy is the most commonly used regimen for patients with primary CNS lymphoma.
CONCLUSIONS
We present a case of leptomeningeal metastases of NPC for which the treatment paradigm of CNS lymphoma was applied with excellent response. The patient remains asymptomatic 6 years later without evidence of clinical disease. We recommend the investigation of systemic methotrexate for the treatment of NPC with CNS involvement in future clinical trials. This may have been a rare patient with an unusually good prognosis who, despite medical therapy, would have done well; however, after methotrexate his cranial neuropathies were reversed.
References
- 1.Khor TH, Tan BC, Chua EJ, Chia KB. Distant metastases in nasopharyngeal carcinoma. Clin Radiol. 1978;29:27–30. doi: 10.1016/s0009-9260(78)80160-3. [DOI] [PubMed] [Google Scholar]
- 2.Cvitkovic E, Bachouchi M, Boussen H, et al. Leukemoid reaction, bone marrow invasion, fever of unknown origin, and metastatic pattern in the natural history of advanced undifferentiated carcinoma of nasopharyngeal type: a review of 255 consecutive cases. J Clin Oncol. 1993;11:2434–2442. doi: 10.1200/JCO.1993.11.12.2434. [DOI] [PubMed] [Google Scholar]
- 3.Redman BG, Tapazoglou E, Al-Sarraf M. Meningeal carcinomatosis in head and neck cancer. Report of six cases and review of the literature. Cancer. 1986;58:2656–2661. doi: 10.1002/1097-0142(19861215)58:12<2656::aid-cncr2820581218>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 4.Lee AW, Au JS, Teo PM, et al. Staging of nasopharyngeal carcinoma: suggestions for improving the current UICC/AJCC Staging System. Clin Oncol (R Coll Radiol) 2004;16:269–276. doi: 10.1016/j.clon.2004.01.008. [DOI] [PubMed] [Google Scholar]
- 5.Baker SR, Wolfe RA. Prognostic factors in nasopharyngeal malignancy. Cancer. 1982;49:163–169. doi: 10.1002/1097-0142(19820101)49:1<163::aid-cncr2820490132>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 6.Liu L, Liang S, Li L, et al. Prognostic impact of magnetic resonance imaging-detected cranial nerve involvement in nasopharyngeal carcinoma. Cancer. 2009;115:1995–2003. doi: 10.1002/cncr.24201. [DOI] [PubMed] [Google Scholar]
- 7.Li JC, Mayr NA, Yuh WT, Wang JZ, Jiang GL. Cranial nerve involvement in nasopharyngeal carcinoma: response to radiotherapy and its clinical impact. Ann Otol Rhinol Laryngol. 2006;115:340–345. doi: 10.1177/000348940611500504. [DOI] [PubMed] [Google Scholar]
- 8.Ilhan O, Sener EC, Ozyar E. Outcome of abducens nerve paralysis in patients with nasopharyngeal carcinoma. Eur J Ophthalmol. 2002;12:55–59. doi: 10.1177/112067210201200111. [DOI] [PubMed] [Google Scholar]
- 9.Roh JL, Sung MW, Kim KH, et al. Nasopharyngeal carcinoma with skull base invasion: a necessity of staging subdivision. Am J Otolaryngol. 2004;25:26–32. doi: 10.1016/j.amjoto.2003.09.011. [DOI] [PubMed] [Google Scholar]
- 10.Ngan RK, Yiu HH, Cheng HK, Chan JK, Sin VC, Lau WH. Central nervous system metastasis from nasopharyngeal carcinoma: a report of two patients and a review of the literature. Cancer. 2002;94:398–405. doi: 10.1002/cncr.10179. [DOI] [PubMed] [Google Scholar]
- 11.Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized Intergroup study 0099. J Clin Oncol. 1998;16:1310–1317. doi: 10.1200/JCO.1998.16.4.1310. [DOI] [PubMed] [Google Scholar]
- 12.Batchelor T, Carson K, O’Neill A, et al. Treatment of primary CNS lymphoma with methotrexate and deferred radiotherapy: a report of NABTT 96-07. J Clin Oncol. 2003;21:1044–1049. doi: 10.1200/JCO.2003.03.036. [DOI] [PubMed] [Google Scholar]
- 13.Grossman SA, Krabak MJ. Leptomeningeal carcinomatosis. Cancer Treat Rev. 1999;25:103–119. doi: 10.1053/ctrv.1999.0119. [DOI] [PubMed] [Google Scholar]
- 14.Waki F, Ando M, Takashima A, et al. Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. J Neurooncol. 2009;93:205–212. doi: 10.1007/s11060-008-9758-3. [DOI] [PubMed] [Google Scholar]
- 15.Mehta M, Bradley K. Radiation therapy for leptomeningeal cancer. Cancer Treat Res. 2005;125:147–158. doi: 10.1007/0-387-24199-x_9. [DOI] [PubMed] [Google Scholar]
- 16.Glantz MJ, Hall WA, Cole BF, et al. Diagnosis, management, and survival of patients with leptomeningeal cancer based on cerebrospinal fluid-flow status. Cancer. 1995;75:2919–2931. doi: 10.1002/1097-0142(19950615)75:12<2919::aid-cncr2820751220>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 17.Grossman SA, Finkelstein DM, Ruckdeschel JC, Trump DL, Moynihan T, Ettinger DS. Randomized prospective comparison of intraventricular methotrexate and thiotepa in patients with previously untreated neoplastic meningitis. Eastern Cooperative Oncology Group. J Clin Oncol. 1993;11:561–569. doi: 10.1200/JCO.1993.11.3.561. [DOI] [PubMed] [Google Scholar]
- 18.Siegal T. Leptomeningeal metastases: rationale for systemic chemotherapy or what is the role of intra-CSF-chemotherapy? J Neurooncol. 1998;38:151–157. doi: 10.1023/a:1005999228846. [DOI] [PubMed] [Google Scholar]
- 19.Lassman AB, Abrey LE, Shah GD, et al. Systemic high-dose intravenous methotrexate for central nervous system metastases. J Neurooncol. 2006;78:255–260. doi: 10.1007/s11060-005-9044-6. [DOI] [PubMed] [Google Scholar]
- 20.Grant R, Naylor B, Greenberg HS, Junck L. Clinical outcome in aggressively treated meningeal carcinomatosis. Arch Neurol. 1994;51:457–461. doi: 10.1001/archneur.1994.00540170033013. [DOI] [PubMed] [Google Scholar]
- 21.Demopoulos A. Leptomeningeal metastases. Curr Neurol Neurosci Rep. 2004;4:196–204. doi: 10.1007/s11910-004-0039-z. [DOI] [PubMed] [Google Scholar]
- 22.Siegal T, Lossos A, Pfeffer MR. Leptomeningeal metastases: analysis of 31 patients with sustained off-therapy response following combined-modality therapy. Neurology. 1994;44:1463–1469. doi: 10.1212/wnl.44.8.1463. [DOI] [PubMed] [Google Scholar]
- 23.Glantz MJ, Jaeckle KA, Chamberlain MC, et al. A randomized controlled trial comparing intrathecal sustained-release cytarabine (DepoCyt) to intrathecal methotrexate in patients with neoplastic meningitis from solid tumors. Clin Cancer Res. 1999;5:3394–3402. [PubMed] [Google Scholar]
- 24.Balis FM, Poplack DG. Central nervous system pharmacology of antileukemic drugs. Am J Pediatr Hematol Oncol. 1989;11:74–86. doi: 10.1097/00043426-198921000-00017. [DOI] [PubMed] [Google Scholar]
- 25.Stewart JS, Cohen EE, Licitra L, et al. Phase III study of gefitinib compared with intravenous methotrexate for recurrent squamous cell carcinoma of the head and neck. J Clin Oncol. 2009;27:1864–1871. doi: 10.1200/JCO.2008.17.0530. corrected. [DOI] [PubMed] [Google Scholar]
- 26.Taylor SGt, McGuire WP, Hauck WW, Showel JL, Lad TE. A randomized comparison of high-dose infusion methotrexate versus standard-dose weekly therapy in head and neck squamous cancer. J Clin Oncol. 1984;2:1006–1011. doi: 10.1200/JCO.1984.2.9.1006. [DOI] [PubMed] [Google Scholar]
- 27.Ervin TJ, Kirkwood J, Weichselbaum RR, Miller D, Pitman SW, Frei E., III Improved survival for patients with advanced carcinoma of the head and neck treated with methotrexate-leucovorin prior to definitive radiotherapy or surgery. Laryngoscope. 1981;91:1181–1190. doi: 10.1288/00005537-198107000-00018. [DOI] [PubMed] [Google Scholar]
- 28.Kwong YL, Yeung DY, Chan JC. Intrathecal chemotherapy for hematologic malignancies: drugs and toxicities. Ann Hematol. 2009;88:193–201. doi: 10.1007/s00277-008-0645-y. [DOI] [PubMed] [Google Scholar]
- 29.Gilchrist NL, Caldwell J, Watson ID, et al. Comparison of serum and cerebrospinal fluid levels of methotrexate in man during high-dose chemotherapy for aggressive non-Hodgkin’s lymphoma. Cancer Chemother Pharmacol. 1985;15:290–294. doi: 10.1007/BF00263903. [DOI] [PubMed] [Google Scholar]
- 30.Hryniuk WM, Bertino JR. Treatment of leukemia with large doses of methotrexate and folinic acid: clinical-biochemical correlates. J Clin Invest. 1969;48:2140–2155. doi: 10.1172/JCI106181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tetef ML, Margolin KA, Doroshow JH, et al. Pharmacokinetics and toxicity of high-dose intravenous methotrexate in the treatment of leptomeningeal carcinomatosis. Cancer Chemother Pharmacol. 2000;46:19–26. doi: 10.1007/s002800000118. [DOI] [PubMed] [Google Scholar]
- 32.Glantz MJ, Cole BF, Recht L, et al. High-dose intravenous methotrexate for patients with nonleukemic leptomeningeal cancer: is intrathecal chemotherapy necessary? J Clin Oncol. 1998;16:1561–1567. doi: 10.1200/JCO.1998.16.4.1561. [DOI] [PubMed] [Google Scholar]
- 33.Abrey LE, DeAngelis LM, Yahalom J. Long-term survival in primary CNS lymphoma. J Clin Oncol. 1998;16:859–863. doi: 10.1200/JCO.1998.16.3.859. [DOI] [PubMed] [Google Scholar]
- 34.DeAngelis LM, Yahalom J, Thaler HT, Kher U. Combined modality therapy for primary CNS lymphoma. J Clin Oncol. 1992;10:635–643. doi: 10.1200/JCO.1992.10.4.635. [DOI] [PubMed] [Google Scholar]
- 35.Glass J, Gruber ML, Cher L, Hochberg FH. Preirradiation methotrexate chemotherapy of primary central nervous system lymphoma: long-term outcome. J Neurosurg. 1994;81:188–195. doi: 10.3171/jns.1994.81.2.0188. [DOI] [PubMed] [Google Scholar]
- 36.Rampen FH, van Andel JG, Sizoo W, van Unnik JA. Radiation therapy in primary non-Hodgkin’s lymphomas of the CNS. Eur J Cancer. 1980;16:177–184. doi: 10.1016/0014-2964(80)90149-8. [DOI] [PubMed] [Google Scholar]
- 37.Nelson DF, Martz KL, Bonner H, et al. Non-Hodgkin’s lymphoma of the brain: can high dose, large volume radiation therapy improve survival? Report on a prospective trial by the Radiation Therapy Oncology Group (RTOG): RTOG 8315. Int J Radiat Oncol Biol Phys. 1992;23:9–17. doi: 10.1016/0360-3016(92)90538-s. [DOI] [PubMed] [Google Scholar]
- 38.Ferreri AJ, Reni M, Dell’Oro S, et al. Combined treatment with high-dose methotrexate, vincristine and procarbazine, without intrathecal chemotherapy, followed by consolidation radiotherapy for primary central nervous system lymphoma in immuno-competent patients. Oncology. 2001;60:134–140. doi: 10.1159/000055310. [DOI] [PubMed] [Google Scholar]
- 39.Ferreri AJ, Reni M, Foppoli M, et al. High-dose cytarabine plus high-dose methotrexate versus high-dose methotrexate alone in patients with primary CNS lymphoma: a randomised phase 2 trial. Lancet. 2009;374:1512–1520. doi: 10.1016/S0140-6736(09)61416-1. [DOI] [PubMed] [Google Scholar]
- 40.Poortmans PM, Kluin-Nelemans HC, Haaxma-Reiche H, et al. High-dose methotrexate-based chemotherapy followed by consolidating radiotherapy in non-AIDS-related primary central nervous system lymphoma: European Organization for Research and Treatment of Cancer Lymphoma Group Phase II Trial 20962. J Clin Oncol. 2003;21:4483–4488. doi: 10.1200/JCO.2003.03.108. [DOI] [PubMed] [Google Scholar]
- 41.Guha-Thakurta N, Damek D, Pollack C, Hochberg FH. Intravenous methotrexate as initial treatment for primary central nervous system lymphoma: response to therapy and quality of life of patients. J Neurooncol. 1999;43:259–268. doi: 10.1023/a:1006210703827. [DOI] [PubMed] [Google Scholar]
- 42.Pels H, Schmidt-Wolf IG, Glasmacher A, et al. Primary central nervous system lymphoma: results of a pilot and phase II study of systemic and intraventricular chemotherapy with deferred radiotherapy. J Clin Oncol. 2003;21:4489–4495. doi: 10.1200/JCO.2003.04.056. [DOI] [PubMed] [Google Scholar]
- 43.O’Brien PC, Roos DE, Pratt G, et al. Combined-modality therapy for primary central nervous system lymphoma: long-term data from a phase II multicenter study (Trans-Tasman Radiation Oncology Group) Int J Radiat Oncol Biol Phys. 2006;64:408–413. doi: 10.1016/j.ijrobp.2005.07.958. [DOI] [PubMed] [Google Scholar]
- 44.Ferreri AJ, Reni M, Villa E. Therapeutic management of primary central nervous system lymphoma: lessons from prospective trials. Ann Oncol. 2000;11:927–937. doi: 10.1023/a:1008376412784. [DOI] [PubMed] [Google Scholar]