

Abstract
Objective
To evaluate the effects of a brief group cognitive-behavioral (CB) depression prevention program for high-risk adolescents with elevated depressive symptoms at 1- and 2-year follow-up.
Method
In this indicated prevention trial, 341 at-risk youth were randomized to a group CB intervention, group supportive expressive intervention, CB bibliotherapy, or educational brochure control condition.
Results
Group CB participants showed significantly greater reductions in depressive symptoms than brochure control participants by 1-year follow-up and compared to bibliotherapy participants by 1- and 2-year follow-up, but not relative to supportive expressive participants. Supportive expressive participants showed greater symptom reduction than CB bibliotherapy participants at 2-year follow-up. Risk for onset of major or minor depression over the 2-year follow-up was significantly lower for group CB participants (14%; OR = 2.2) and CB bibliotherapy participants (3%; OR = 8.1) than brochure controls (23%).
Conclusions
Results indicate that this group CB intervention reduces initial symptoms and risk for future depressive episodes, although both supportive expressive therapy and CB bibliotherapy also produce intervention effects that persist long term. Indeed, CB bibliotherapy emerged as the least expensive method of reducing risk for future episodes of depression.
Keywords: depression, prevention, high-risk, adolescent, alternative interventions
Major depression is a common, recurrent, and impairing condition that increases risk for future suicide attempts, academic failure, interpersonal problems, unemployment, substance abuse, and delinquency (Klein, Torpey, & Bufferd, 2008). Because less than one third of depressed youth receive treatment (Newman et al., 1996) it is crucial to develop prevention programs for this psychiatric condition.
At present, cognitive-behavioral (CB) interventions that primarily focus on reducing negative cognitions have the most empirical support. CB interventions have produced significantly greater reductions in depressive symptoms than assessment-only control groups in universal trials (Jaycox, Reivich, Gillham, & Seligman, 1994; Shochet et al., 2001; Spence, Sheffield, & Donovan, 2003), in selected trials with high-risk youth (Seligman, Schulman, & Tryon, 2007), and in indicated trials involving youth with elevated depressive symptoms (Clarke et al., 1995, 2001; Garber et al., 2009; Stice, Burton, Bearman, & Rohde, 2006). Although these interventions typically produce significantly greater reductions in depressive symptoms than observed in assessment-only control groups, effects rarely persist through 1- and 2-year follow-up. A meta-analytic review found that only 4 out of 17 trials of CB depression prevention programs produced effects that remained significant at 1-year follow-up, with an average effect size of only an r = .08 across the 17 trials (Stice, Shaw, Bohon, Marti, & Rohde, 2009). For instance, Clarke et al. (1995) found that a 15-session group CB intervention resulted in greater reductions in depressive symptoms by posttest compared to an assessment-only control condition for adolescents with depressive symptoms, though this effect was nonsignificant at 1-year follow-up. CB interventions have significantly reduced risk for future onset of major depression during follow-up in some trials (Clarke et al., 1995; 2001; Stice, Rohde, Seeley, & Gau, 2008) but not others (Gillham, Hamilton, Freres, Patton & Gallop, 2006; Seligman, Schulman, DeRubeis, & Hollon, 1999; Seligman et al., 2007; Sheffield et al., 2006). Garber and associates (2009) found that their group CB intervention significantly reduced risk for onset of depressive episodes relative to assessment-only controls over a 6-month period during which booster sessions were administered monthly.
Although several CB prevention programs have produced promising findings, the long duration of these interventions makes them challenging to implement. In addition, we believe that adolescents are more likely to benefit from prevention programs that have only a few simple concepts to remember. In line with this thesis, a meta-analytic review of obesity prevention programs found that programs that focus on fewer concepts produced significantly larger effects than those that focus on numerous concepts (Stice, Shaw, & Marti, 2006). It is possible that a similar process occurs for depression prevention programs. Thus, we developed a brief 6-session group CB prevention program that focused exclusively on reducing negative cognitions and increasing pleasant activities among individuals with elevated depressive symptoms. An earlier report from this indicated depression prevention trial found that participants assigned to this program showed significantly greater reductions in initial depressive symptoms and psychosocial impairment and reduced risk for onset of future major depression than educational brochure controls through 6-month follow-up (Stice, Rohde et al., 2008). The present report describes the effects for this group CB program through 1- and 2-year follow-up.
Another gap in the literature is that few trials have compared CB prevention programs to placebo or alternative interventions. This comparison is necessary to determine whether effects result because of the specific therapeutic procedures theorized to produce intervention effects or nonspecific effects common to all group-based interventions (e.g., therapeutic alliance, group cohesion, installation of hope, participant expectancies). Indeed, one criterion for establishing that an intervention is efficacious is that it outperforms a placebo or alternative intervention (American Psychiatric Association, 1995).
Five trials have compared CB depression prevention programs to alternative interventions. Merry, McDowell, Wild, Bir, and Cunliffe (2004) found that a universal CB program produced greater reductions in depressive symptoms at posttest than an arts and crafts intervention, though effects were nonsignificant by 18-month follow-up. Stice et al. (2006) found that participants assigned to a CB program, supportive expressive therapy, CB bibliotherapy, expressive writing, and a journaling intervention showed greater reductions in symptoms than assessment-only controls at posttest, but only bibliotherapy produced effects that persisted through 6-month follow-up. CB participants showed greater symptom reductions relative to only journaling participants and only at posttest. Bibliotherapy participants showed greater symptom reductions than expressive writing participants at 6-month follow-up. Gillham et al. (2007) found that a CB depression prevention program did not produce greater symptom reductions than a nonspecific comparison intervention or an assessment-only control condition. Horowitz, Garber, Ciesla, Young, and Mufson, (2007) found that both a CB and an interpersonal therapy intervention reduced symptoms relative to assessment-only controls through posttest, but not 6-month follow-up; there were no significant differences between the two interventions. An earlier report from the present trial (Stice, Rohde et al., 2008) found that group CB participants showed greater symptom reductions at posttest than supportive expressive and CB bibliotherapy participants, though effects were nonsignificant by 6-month follow-up. Supportive expressive and bibliotherapy participants both showed greater symptom reductions than assessment-only controls through 6-month follow-up, with supportive expressive participants showing greater reductions than bibliotherapy participants at posttest, implying that nonspecific factors contribute to CB intervention effects or that interventions with either general group nonspecific therapeutic factors or CB material produce effects.
Thus, trials provide limited evidence that group CB depression prevention programs significantly outperform alternative interventions. Further, most of these trials used brief follow-up periods. The present report compared the effects of the brief group CB prevention program against a supportive expressive intervention that was intended to control for nonspecific therapeutic factors and a CB bibliotherapy that was intended to control for CB content at 1- and 2-year follow-up. The goals of supportive expressive interventions, which have been used in prior depression treatment trials (Brent et al., 1997; Shaw, 1977), are to establish and maintain rapport, provide support, and help the client identify and express emotions. Bibliotherapy refers to the prescription of books for the treatment of a disorder. We thought it vital to compare the apparent intervention of choice for the prevention of depression (i.e., group CB) to bibliotherapy because the latter is much less expensive and easier to disseminate. Our primary outcomes were reductions in depressive symptoms, risk for onset of major/minor depressive disorder, and improvements in social adjustment. We targeted adolescents with depressive symptoms because meta-analytic reviews found that selected and indicated programs targeting high-risk youth produce larger effects than universal programs offered to unselected adolescents (Horowitz & Garber, 2006; Stice et al., 2009). In theory, youth struggling with subdiagnostic depression may be more likely to engage in the prevention program because they are more motivated to change. It may also be easier to acquire intervention skills when they can be applied to current symptoms. We focused on adolescents with depressive symptoms because risk factor studies have found that this is typically the most potent predictor of future onset of major depression (Lewinsohn et al., 1994; Seeley, Stice, & Rohde, 2009; Weissman et al., 1992) and this population has responded to CB prevention programs (Clarke et al., 1995, 2001; Garber et al., 2009).
Methods
Participants
Participants were 341 high school students (56% female) who ranged in age from 14 to 19 years (M = 15.6; SD = 1.2) at pretest. The sample was composed of 2% Asians, 9% African Americans, 46% Caucasians, 33% Hispanics, and 10% who specified other or mixed heritage, which was somewhat more ethnically diverse than the greater Austin area (7% African American, 18% Hispanic, 65% Caucasian) because we systematically recruited at schools with high proportions of minority students to maximize the ethnic diversity of our sample. Educational attainment of parents, a proxy for socioeconomic status, was 26% high school graduate or less; 17% some college; 35% college graduate; 18% graduate degree, which was somewhat higher than the population from which we sampled (34% high school graduate or less; 25% some college; 26% college graduate; 15% graduate degree), potentially because of the proximity to a large state university. Twenty-eight percent of the sample had received treatment services for emotional/behavioral problems during the 1-year period preceding the study. Past treatment services did not significantly differ by condition (χ2[3,338] = 1.36; p = .711; group CB 26%, supportive expressive 24%, CB bibliotherapy 28%, and brochure control 23%). Of those who received treatment, 41% received individual therapy, 9% group or family therapy, 8% took medication, and 42% a combination of treatment types. Past treatment type did not significantly differ by condition (χ2[9,91] = 12.37; p = .192). Twenty-nine percent of participants received treatment services for psychiatric problems during the 2-year follow-up; rates did not significantly differ by condition (χ2[3,313] = 4.25; p = .236; group CB 21%, supportive expressive 28%, CB bibliotherapy 30%, and brochure control 22%). Of those receiving treatment during the study 41% received individual therapy, 14% group or family therapy, 10% took medication, and 34% a combination of treatment types. Treatment type during the follow-up did not significantly differ by condition (χ2[9,92] = 6.68; p = .670).
Procedures
Participants were recruited using mass mailings, handbills distributed during the lunch hour, and posters that invited students experiencing sadness to participate in a trial of interventions designed to improve current and future mood. Interested students were given a depression screener (the Center for Epidemiologic Studies-Depression scale [CES-D; Radloff, 1977]) and a consent form. Those who returned a signed consent form and scored 20 or above on the CES-D were invited to complete a pretest assessment. We selected this cutoff because an epidemiologic study (Roberts, Lewinsohn, & Seeley, 1991) found that 31% of community-dwelling adolescents scored above 20 on the CES-D and this cutoff appeared to maximize sensitivity for detecting youth at risk for major depression. Students who met diagnostic criteria for current major depression upon interview were excluded and given treatment referrals (there were no other exclusion criteria). All participants were provided with treatment referral information and encouraged to seek treatment if their depressive symptoms escalated during the trial. If a youth endorsed suicidal ideation during any interview, project staff contracted for safety with the studend and called the student’s parent to emphasize the importance of seeking treatment and provide additional referral information. This issue emerged during 14 interviews over the course of the study. Four participants endorsed suicidal ideation during eligibility interviews (prior to randomization) and were excluded because they met criteria for current major depression. Ten youth endorsed suicidal ideation during follow-up interviews (3 group CB participants, 1 supportive expressive participant, 3 bibliotherapy participants, and 3 control participants).
Participants were recruited at six schools (40–75 students per school) between 2004 and 2007 and were randomly assigned, within blocks created by gender and school, by the project coordinator using computer-generated random numbers to intervention condition: (1) group CB (n = 89), (2) group supportive expressive (n = 88), (3) CB bibliotherapy (n = 80), or (4) educational brochure control (n = 84). Group CB and supportive expressive interventions consisted of six weekly 1-hour sessions. Groups contained 3–10 same-sex participants; CB groups contained an average of 6.3 participants and supportive expressive groups an average of 6.8 participants. Groups were facilitated by a clinical psychology graduate student and co-facilitated by an undergraduate psychology student. Facilitators were assigned to conduct groups based on: 1) academic or clinical training experiences that enhanced the facilitator’s ability to lead either CB or supportive expressive groups; 2) preference for the therapeutic approach (CB or supportive expressive); 3) time availability to conduct a group on a weekly basis for six weeks; and 4) gender (the gender of at least one of the facilitators matched the gender of group participants). Facilitators (n=13) conducted an average of 4 groups. Five facilitators (38%) conducted only CB groups, 3 (23%) conducted only SE groups, and 5 (38%) conducted both CB and SE groups. If a participant missed a session, a brief (10–15 minute) individual session was conducted with the youth to review missed material when possible. Detailed manuals for group interventions contained a theoretical rationale for the program, general facilitator guidelines, material needed for each session, and outlines for all six sessions (session topics, points to cover in each section, anticipated time requirements for each section, home practice assignments for the CB condition). The manuals were designed to provide consistency across facilitators and provide a comparable level of guidance for both forms of group intervention, but were not verbatim scripts. The report of the acute effects of this trial (Stice, Rohde et al., 2008) provides information on facilitator training, supervision, and competence and fidelity ratings.
Participants completed a survey and diagnostic interview at pretest, posttest, 6-month, 1-year, and 2-year follow-ups. They were paid $20 for completing each assessment. Participant flow through the study is shown in Figure 1. Assessors, who were blinded to condition, had at least a BA in psychology and received 40 hours of training in the use of the semi-structured interviews, which involved didactic presentations on diagnostic criteria and interview skills, practice ratings of pre-recorded interviews, and interview role-plays. Assessors were required to show a minimum kappa agreement of .80 for diagnosis with expert raters before starting data collection and to maintain this throughout the study (assessed in a randomly selected 10% of taped interviews). Assessments and groups were conducted at schools after classes at the convenience of participants. The local Institutional Review Board approved this study.
Figure 1.

Flow of participants through each stage of the study.
CB Depression Prevention Intervention
In the design of our brief CB program we drew upon the Clarke et al. (1995) program, general CB concepts for the prevention and treatment of depression, and our experience with the design of eating disorder prevention programs. Didactic presentation was minimized because psychoeducational interventions are less effective than interventions that actively engage participants (Stice & Shaw, 2004). The 6 weekly 1-hour sessions focused on building group rapport, increasing participant involvement in pleasant activities (Sessions 1–6), learning and practicing cognitive restructuring techniques (Sessions 2–4), and developing response plans for future life stressors (Sessions 5–6). In-session exercises were used that required youth to apply the skills taught in the intervention. Homework1 was used to reinforce the skills taught in the sessions and help participants learn how to apply these skills to their daily life. We also used motivational enhancement exercises to maximize willingness to use the new skills, strategic self-presentation to facilitate internalization of key principles, behavioral techniques to reinforce use of the new skills, and group activities to foster feelings of social support and group cohesion.
Supportive Expressive Group Intervention
The goals of this intervention were to establish and maintain rapport, provide support, and help participants identify and express feelings; this group did not cover any specific skills from the other conditions. The 6 weekly 1-hour sessions provided a forum to discuss feelings in a safe environment based on the rationale that (a) sharing our inner feelings with another person reduces stress and improves our mood, (b) listening to others helps us realize we are not alone, and (c) it’s more helpful to listen than tell others what to do. The sessions were devoted to open sharing, providing participants with a venue to discuss and process their emotional experiences since the previous meeting. Participants were encouraged to discuss changes in their experiences, as well as any emerging problems or worries. No direct advice was given. Participants and facilitators actively supported and responded to one another. All sessions concluded with a summary statement by the facilitators that focused on common themes that emerged in the session.
CB Bibliotherapy Intervention
Participants in the bibliotherapy condition were given copies of Feeling Good (Burns, 1980), which provides relevant and practical CB techniques for preventing and reducing negative moods and is considered an effective self-help book for depression. It is written at a high-school reading level. The book covers several topics (e.g., understanding feelings of sadness, building self-esteem) but the majority of text is focused on repeated examples of cognitive restructuring.
Educational Brochure Control Condition
At pretest, participants were given a National Institute of Mental Health brochure that describes major depression and recommends treatment for depressed youth (“Let’s Talk About Depression” Pub. 01–4162), as well as information about local treatment options. They completed the same assessments as those in the other conditions, which allowed us to monitor depression and suicidal ideation, and to contact parents and provide treatment referrals as necessary (as was done in all conditions). Participants and their parents were also asked to contact research staff if they believe that the adolescent’s depression had worsened. We selected this control group because it represents an ecologically valid control condition of what is generally provided to youth in local schools.
Measures
Depressive symptoms and diagnosis
Sixteen items assessing major depression symptoms based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM–IV; American Psychiatric Association, 1994) were adapted from the Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS; Kaufman, Birmaher, Brent, Rao, & Ryan, 1996), a semi-structured diagnostic interview. Adolescents reported the peak severity of each symptom over their lifetime and over the past month at baseline or since the last interview at each follow-up assessment on a month-by-month basis. Items used an expanded response format (response options: 1 = not at all to 4 = severe symptoms [with ratings of 3 and 4 reflecting diagnostic levels]). We averaged across the 16 severity items to form a continuous depressive symptom composite, which captured severity of symptoms over the past 6 months for the 1-year follow-up and over the past 12 months for the 2-year follow-up. Responses were also used to determine whether participants met diagnostic criteria for major or minor depression over their lifetime and since the last assessment. This adapted version of the K-SADS has shown test-retest reliability (k = .63 to 1.00) and interrater reliability for depression diagnosis (k = .73 to 1.00), internal consistency (α = .68 to .84), and predictive validity (Nolen-Hoeksema, Stice, Wade, & Bohon, 2007). To assess the inter-rater reliability in the present trial, a randomly selected subset of participants (5% of all interviews) were re-interviewed within a 3-day period by a second assessor who was blind to the first diagnosis, resulting in high inter-rater agreement for diagnoses (k = .83) and for the continuous symptom composite (r = .85). Another randomly selected subset of participants (5% of all interviews) completed a second diagnostic interview with the same assessor 1 week later, resulting in high test-retest reliability for diagnoses (k = .83) and for the continuous symptom composite (r = .93). In the present trial the depressive symptom severity score showed internal consistency (α = .75) and sensitivity to detecting intervention effects (Stice, Rohde et al., 2008). At baseline, 28% of the participants reported a past history of major depression and 12% reported past minor depression (differences in rates between the four intervention conditions were nonsignificant).
We also included the 21-item Beck Depression Inventory (BDI; Beck, Steer, & Garbin, 1988) to allow more direct comparisons with results from previous depression prevention trials. For each item, participants select from among four responses reflecting the increasing levels of symptom severity (0 = no symptom present to 3 = severe symptom present) in the past two weeks. The BDI has acceptable internal consistency (α .73 to .95), test–retest reliability (r = .60 to .90), and convergent validity with clinician ratings of depressive symptoms (mean r = .75; Beck et al., 1988). In the present study, the BDI had good internal consistency at baseline (α = .82). Although we report results for the BDI, our primary outcome measure is the interviewer-assessed depressive symptoms because this measure covers a broader time period and incorporates the interviewer’s synthesis and interpretation of the adolescent’s report. The BDI correlated with the K-SADS depressive symptom composite at baseline (r = .58).
Social adjustment
We used 17 items adapted from the Social Adjustment Scale–Self Report for Youth (Weissman, Orvaschel, & Padian, 1980) to assess social impairment in school, peer, spare time, and family domains (response options: 1 = never to 5 = always). The 17-item version has shown internal consistency (α = .77), 1-week test-retest reliability (r = .83), and sensitivity to detecting intervention effects (Stice, Marti, Spoor, Presnell, & Shaw, 2008). In the present study the scale had marginal internal consistency at baseline (α = .71)
Results
Preliminary Analysis
Participants assigned to the four conditions did not differ on demographic characteristics reported in Table 1 or baseline outcome measures reported in Table 2, with the exception of baseline interview-assessed depressive symptoms F(3,337) = 4.94, p = .002, η2 = .04. A Scheffe comparison showed that bibliotherapy participants had significantly lower baseline depressive symptoms than group CB and supportive expressive participants, but not brochure controls. Thus, subsequent analysis controlled for baseline depressive symptoms.
Table 1.
Descriptive Statistics by Condition for Study Demographic Characteristics
| Group CB n = 89 |
Supportive expressive n = 88 |
CB Bibliotherapy n = 80 |
Brochure Control n = 84 |
|||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Female | 51 | 57.3 | 48 | 54.5 | 43 | 53.8 | 50 | 59.5 |
| Race | ||||||||
| Black | 5 | 5.6 | 6 | 6.8 | 7 | 8.8 | 12 | 14.3 |
| Hispanic | 37 | 41.6 | 31 | 35.2 | 19 | 23.8 | 24 | 28.6 |
| White | 37 | 41.6 | 40 | 45.5 | 44 | 55.0 | 35 | 41.7 |
| Other | 10 | 11.2 | 11 | 12.5 | 10 | 12.5 | 13 | 15.5 |
| Age | ||||||||
| 14 years | 20 | 22.5 | 15 | 17.0 | 14 | 17.5 | 20 | 23.8 |
| 15 years | 29 | 32.6 | 25 | 28.4 | 30 | 37.5 | 29 | 34.5 |
| 16 years | 17 | 19.1 | 23 | 26.1 | 24 | 30.0 | 16 | 19.0 |
| 17 years | 17 | 19.1 | 22 | 25.0 | 11 | 13.8 | 13 | 15.5 |
| 18 years | 6 | 6.7 | 3 | 3.4 | 1 | 1.3 | 6 | 7.1 |
| Maximum parental education | ||||||||
| Grade school graduate | 8 | 10.0 | 10 | 11.9 | 6 | 7.6 | 8 | 9.5 |
| High school graduate | 13 | 16.3 | 15 | 17.9 | 12 | 15.2 | 17 | 20.2 |
| Some college | 18 | 22.5 | 15 | 17.9 | 13 | 16.5 | 13 | 15.5 |
| College graduate | 29 | 36.3 | 31 | 36.9 | 30 | 38.0 | 30 | 35.7 |
| Advanced degree | 12 | 15.0 | 13 | 15.5 | 18 | 22.8 | 16 | 19.0 |
Notes. CB = Cognitive Behavioral; No pairwise comparisons are statistically significant at p < .05 for any participant characteristics.
Table 2.
Descriptive Statistics by Intervention Condition for Study Outcome Measures
| Outcome Measures | Group CB n = 89 |
Supportive expressive n = 88 |
CB Bibliotherapy n = 80 |
Brochure Control n = 84 |
||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Depressive symptoms | ||||||||
| Pretest | 1.88 | 0.35 | 1.83 | 0.37 | 1.68 | 0.31 | 1.81 | 0.30 |
| Posttest | 1.52 | 0.33 | 1.63 | 0.34 | 1.62 | 0.36 | 1.69 | 0.36 |
| 6-month follow-up | 1.52 | 0.44 | 1.56 | 0.42 | 1.45 | 0.39 | 1.67 | 0.45 |
| 1-year follow-up | 1.51 | 0.41 | 1.50 | 0.41 | 1.48 | 0.41 | 1.59 | 0.41 |
| 2-year follow-up | 1.48 | 0.43 | 1.48 | 0.37 | 1.51 | 0.43 | 1.55 | 0.43 |
| Beck Depression Inventory | ||||||||
| Pretest | 20.12 | 10.38 | 20.27 | 9.83 | 18.21 | 7.53 | 19.60 | 9.23 |
| Posttest | 10.71 | 9.07 | 14.55 | 10.68 | 14.48 | 9.11 | 16.48 | 9.80 |
| 6-month follow-up | 11.87 | 10.06 | 12.92 | 10.27 | 15.84 | 10.93 | 17.48 | 10.98 |
| 1-year follow-up | 13.24 | 11.38 | 12.00 | 9.44 | 12.58 | 9.86 | 14.45 | 10.04 |
| 2-year follow-up | 10.19 | 9.09 | 11.75 | 9.36 | 11.59 | 8.71 | 12.60 | 9.44 |
| Social adjustment | ||||||||
| Pretest | 2.80 | 0.49 | 2.74 | 0.49 | 2.74 | 0.52 | 2.73 | 0.52 |
| 6-month follow-up | 2.51 | 0.51 | 2.64 | 0.58 | 2.66 | 0.48 | 2.67 | 0.52 |
| 1-year follow-up | 2.43 | 0.50 | 2.44 | 0.52 | 2.57 | 0.39 | 2.50 | 0.48 |
| 2-year follow-up | 2.27 | 0.54 | 2.36 | 0.50 | 2.36 | 0.48 | 2.34 | 0.49 |
Notes. CB = Cognitive Behavioral; SD = standard deviation.
Three percent of participants did not provide data at posttest, 9% at the 6-month follow-up, 15% at the 1-year follow-up, and 22% at the 2-year follow-up. On average participants completed 4.4 assessments (SD = 0.9) and the number of completed assessments was not associated with intervention condition, F(3,337) = 1.13, p = .338 or any baseline outcomes or demographic factors (at p < .05). Attendance in the two group conditions was not associated with baseline demographic factors or outcomes at baseline or at follow-up assessments. We employed an intent-to-treat analysis by using maximum likelihood estimates to impute missing data with the NORM software program (Schafer, 1999), as it produces more accurate and efficient parameter estimates than listwise deletion or last-observation-carried-forward (Schafer & Graham, 2002).
Intervention Effects for Primary Outcomes
Omnibus repeated measures analysis of covariance models (ANCOVA) tested whether there was differential change in the continuous outcomes across conditions over the 2-year follow-up (condition was a four-level between-subjects factor, time was a five level within-subjects factor for depressive symptoms and BDI and a four level within-subjects factor for social functioning). Time X Condition interactions indicated there was significantly differential change across conditions for depressive symptoms: F(12,1348) = 3.07; p < .001; η2 = .03, and BDI scores: F(12,1348) = 3.80; p < .001; η2 = .03, but not for social adjustment : F(9,1011) = 1.63; p = .101; η2 = .01. For outcomes with significant omnibus Time X Condition interactions, separate follow-up repeated measures ANCOVA models tested whether groups significantly differed from each other from pretest to 1-year follow-up and from pretest to 2-year follow-up. The Time X Condition interactions (see Table 3) test whether participants in one condition showed significantly greater changes in the outcome than did those in the other condition.
Table 3.
Repeated Measures Analysis of Covariance Pairwise Contrasts
| Cognitive Behavioral | Supportive Expressive | Bibliotherapy | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coeff | SE | 95% CI | p | d | Coeff | SE | 95% CI | p | d | Coeff | SE | 95% CI | p | d | |
| Depressive Symptoms | |||||||||||||||
| Supportive | |||||||||||||||
| 1-year | 0.01 | 0.02 | −0.03,0.06 | .571 | 0.09 | ||||||||||
| 2-year | 0.02 | 0.03 | −0.04–0.07 | .559 | 0.09 | ||||||||||
| Bibliotherapy | |||||||||||||||
| 1-year | 0.06 | 0.02 | 0.01–0.11 | .015 | 0.38 | 0.05 | 0.02 | −0.01–0.09 | .058 | 0.30 | |||||
| 2-year | 0.08 | 0.03 | 0.03–0.13 | .004 | 0.45 | 0.06 | 0.02 | 0.02–0.11 | .011 | 0.40 | |||||
| Control | |||||||||||||||
| 1-year | 0.05 | 0.02 | 0.01–0.10 | .023 | 0.30 | 0.04 | 0.02 | −0.01–0.08 | .090 | 0.26 | −0.01 | 0.02 | −0.05–0.04 | .757 | .05 |
| 2-year | 0.05 | 0.03 | −0.01–0.10 | .056 | 0.29 | 0.03 | 0.02 | −0.01–0.08 | .145 | 0.22 | −0.03 | 0.02 | −0.08–0.02 | .231 | .19 |
|
| |||||||||||||||
| Beck Depression Inventory | |||||||||||||||
| Supportive | |||||||||||||||
| 1-year | −0.49 | 0.60 | −1.67–0.69 | .413 | 0.12 | ||||||||||
| 2-year | 0.50 | 0.58 | −0.64–1.64 | .390 | 0.13 | ||||||||||
| Bibliotherapy | |||||||||||||||
| 1-year | 0.44 | 0.58 | −0.69–1.57 | .442 | 0.12 | 0.93 | 0.53 | −0.10–1.97 | .078 | 0.28 | |||||
| 2-year | 1.17 | 0.54 | 0.11–2.23 | .030 | 0.34 | 0.67 | 0.54 | −0.40–1.74 | .218 | 0.19 | |||||
| Control | |||||||||||||||
| 1-year | 0.62 | 0.62 | −0.61–1.84 | .322 | 0.15 | 1.11 | 0.58 | −0.04–2.25 | .058 | 0.29 | 0.18 | 0.55 | −0.91–1.26 | .751 | .05 |
| 2-year | 1.03 | 0.60 | −0.15–2.23 | .087 | 0.26 | 0.54 | 0.61 | −0.66–1.74 | .377 | 0.14 | −0.13 | 0.57 | −1.25–0.99 | .818 | .04 |
Effects relative to brochure controls
Group CB participants showed significantly greater reductions in depressive symptoms than brochure control participants at the 1-year follow-up, but this effect was only marginal at 2-year follow-up. Although supportive expressive participants showed marginally greater symptom reductions than brochure controls at 1-year follow-up, this effect was nonsignificant at 2-year follow-up. Bibliotherapy participant did not show significantly greater symptom reductions than brochure controls at either follow-up.
Effects relative to other active interventions
Group CB participants showed significantly greater reductions in depressive symptoms than bibliotherapy participants at both the 1- and 2-year follow-up. However, group CB participants did not show significantly greater reductions in depressive symptoms relative to supportive expressive participants at either follow-up. Supportive expressive participants showed marginally greater symptom reductions than bibliotherapy participants at the 1-year follow-up and significantly greater symptom reductions at 2-year follow-up.
Effects for the BDI
With regard to BDI scores, Group CB participants showed greater reductions in BDI scores than bibliotherapy participants at the 2-year, but not the 1-year, follow-up assessment. Although the three other significant follow-up comparisons for interview-assessed depressive symptoms (shown in the top half of Table 3) were not detected for the BDI (shown in the bottom half of Table 3), the findings for the remaining contrasts replicated across the two measures.
As shown in Table 3, the effect sizes, as measured by Cohen’s d-statistic, for the significant and marginal effects ranged from .30 to .45, with an average d = .38. These effect sizes were medium to large per Cohen’s criteria (1988).
Moderation
Sex and age were individually added to the models described above to test for moderation of intervention effects for the depressive symptoms and BDI scores at 1- and 2-year follow-up. No evidence of sex as a moderator was found for depressive symptoms at 1-year (F(9,951) = 1.07; p = .380; η2 = .01) or 2-year follow-up (F(12,1268) = 1.59; p = .087; η2 = .02) or for age as a moderator at 1-year (F(9,951) = 0.69; p = .721; η2 = .01) or 2-year follow-up (F(12,1268) = 0.82; p = .631; η2 = .01). No evidence of sex as a moderator was found for BDI at 1-year (F(9,951) = 0.62; p = .782; η2 = .01) or 2-year follow-up (F(12,1268) = 0.61; p = .832; η2 = .01) or for age as a moderator at 1-year (F(9,951) = 0.44; p = .915; η2 = <.01) or 2-year follow-up (F(12,1268) = 0.56; p = .873; η2 = .01).
Reliable Change
We used the reliable change index to test for clinically significant change in depressive symptoms and BDI scores over the 2-year follow-up (Jacobson & Truax, 1991). Omnibus tests indicated significantly different rates of reliability change in depressive symptoms, χ2(3, 341) = 12.49; p = .006 and BDI scores, χ2(3, 341) = 10.15; p = .017. Follow-up contrasts indicated reliable change rates for depressive symptoms were significantly greater in group CB participants (48.3%, p = .013, odds ratio [OR] = 2.21, 95% confidence interval [CI] = 1.18 to 4.13) than brochure controls (29.8%). Follow-up contrasts for the BDI indicated that reliable change rates were significantly higher in group CB participants (31.5%, p = .041, OR = 2.11, 95% confidence interval CI = 1.03 to 4.31) relative to brochure controls (17.9%) and for supportive expressive participants (25.0%, p = .043, OR = 2.33, 95% confidence interval CI = 1.03 to 5.30) relative to bibliotherapy participants (12.5%).
Intervention Effects for Major/Minor Depression Onset
By the 2-year follow-up, 46 (14%) of the participants had shown onset of major depression (40 cases) or minor depression (6 cases): 19 (23%) of brochure control participants, 12 (14%) of group CB participants, 13 (15%) of group supportive expressive participants, and 2 (3%) of CB bibliotherapy participants. Figure 2 shows cumulative survival functions adjusted for baseline depressive symptoms for the percentage of participants in each condition that showed onset of major/minor depression from baseline to 2-year follow-up. Using 2-tailed tests, Cox proportional hazard models showed that group CB participants (β = 0.80; SE = 0.38; p = .033; OR = 2.23; 95% CI = 1.07–4.67) and bibliotherapy participants (β = 2.10; SE = 0.75; p = .004; OR = 8.13; 95% CI = 1.89–34.96) showed significantly lower risk for onset of depressive episodes during the 2-year follow-up than brochure controls. The incidence for major/minor depression onset did not differ significantly for the remaining contrasts: group CB versus supportive expressive, β = 0.15; SE = 0.40; p = .709; OR = 1.16; 95% CI = 0.52–2.56; group CB versus bibliotherapy, β = −1.29; SE = 0.77; p = .093; OR = 0.28; 95% CI = 0.07–1.24; supportive expressive versus brochure controls, β = 0.65; SE = 0.37; p = .076; OR = 1.92; 95% CI = 0.94–3.97; and supportive expressive versus bibliotherapy, β = −1.44; SE = 0.77; p = .060; OR = 0.24; 95% CI = 0.05–1.06.
Figure 2.
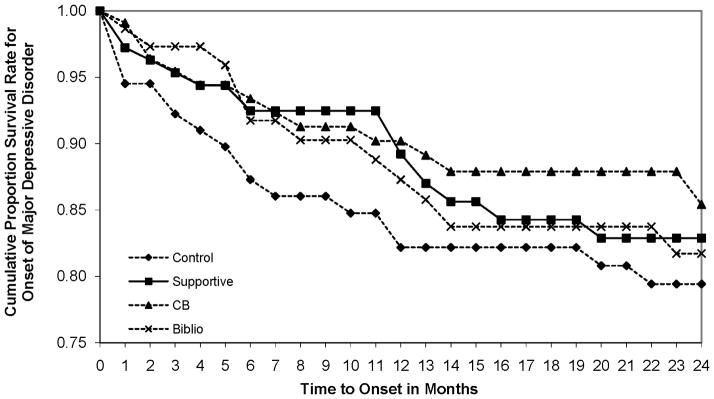
Covariate-adjusted survival curves for onset of major/minor depression by intervention condition. CB = cognitive-behavioral.
Discussion
Participants in the group CB depression prevention program showed significantly greater reductions in depressive symptoms than brochure control participants by 1-year follow-up, though this effect was only marginal by 2-year follow-up. These results are encouraging given that most group CB depression prevention programs do not produce effects that persist to either 1- or 2-year follow-up (Stice et al., 2009). The effect sizes for depressive symptoms (d = .30 at 1-year follow-up and .29 at 2-year follow-up) were medium in magnitude and compare favorably to the average effect sizes from follow-up from recent meta-analytic reviews of depression prevention programs (d = .11; Horowitz & Garber, 2006) and (d = .20; Stice et al., 2009), particularly given that the intervention was only 6 sessions (vs. an average of 11 sessions). Moreover, the pretest to 1-year follow-up effect size per hour of intervention (d = .05) compares favorably to the average parallel effect size for longer CB interventions evaluated in prevention trials (d = .014; Stice et al., 2009). There are several possible explanations for the fact that we observed stronger and more persistent effects for our brief CB depression prevention program than have been previously observed for longer CB depression prevention programs. First, our brief CB program included a focus on increasing pleasant activities, which has not been a core topic in longer CB prevention programs. Second, the longer CB depression prevention programs have typically included a focus on improving coping, problem-solving, and social skills. As noted, it is possible that adolescents are more likely to remember two core skills for combating depression that were covered in our brief CB program versus the wider range of concepts covered in the longer CB programs.
Supportive expressive participants showed marginally greater reductions in depressive symptoms by 1-year follow-up than brochure controls, but this effect was nonsignificant at 2-year follow-up. Bibliotherapy participants did not show significantly greater reductions in depressive symptoms than brochure controls at either follow-up assessment. It might be argued that bibliotherapy did not reduce depressive symptoms because participants in this condition received a small dose of this intervention, as they only read a portion of the book. Yet, data suggested that on average they read 150 pages from pre to post and another 50 pages during follow-up, which would take approximately 5.5 hours, assuming an average high school reading level (Carver, 1990). This is close to the average number of hours participants spent in the group CB intervention (M = 5.1 hours in session, plus time completing homework outside of session), suggesting that dosage was similar for the two CB interventions. However, the timing of the intervention across these two conditions probably differed, which may have influenced the differential effects of these two interventions. It might also be argued that depressive symptoms reduction effects were more difficult to detect for biblotherapy because this group had less of an opportunity to show regression to the mean during the follow-up due to their initially lower symptoms. However, bibliotherapy participants did not differ from brochure controls at baseline on either measure of depressive symptoms, yet bibliotherapy participants still did not show greater symptom reductions than controls on these two outcomes.
Importantly, group CB participants showed significantly greater reductions in depressive symptoms relative to bibliotherapy participants, but not relative to supportive expressive participants, through 1- and 2-year follow-up. There was also evidence that supportive expressive participants showed significantly greater reductions in depressive symptoms than bibliotherapy participants at 2-year follow-up, though this effect was only marginal at 1-year follow-up. We compared group CB to both supportive expressive therapy and CB bibliotherapy as these two alternate interventions can be conceptualized as dismantled aspects of group CB, with the supportive expressive group providing nonspecific therapeutic factors without a CB-specific focus, and bibliotherapy delivering CB content without group-based nonspecific factors. Thus, the evidence that group CB did not significantly outperform the supportive expressive intervention in the present trial or one previous trial (Stice et al., 2006) during follow-up suggests that nonspecific factors unrelated to the CB content may contribute to the therapeutic effects of the group CB prevention program. In line with this interpretation, a report on mediators that account for the effects of these interventions found that group CB resulted in significant increases in emotional expression and reductions in loneliness relative to controls (Stice, Rohde, Seeley, & Gau, 2010). However, it is also possible that both CB content and emotional support are two effective methods of reducing depressive symptoms, even though group CB showed stronger effects relative to controls than did supportive expressive therapy in the present trial and a previous trial (Stice et al., 2006). Either interpretation of these findings implies that it may be possible to improve intervention effects by devoting a greater focus to nonspecific group processes, such as building group rapport and expectations for positive intervention effects.
The evidence that group CB significantly outperformed a credible alternative intervention (bibliotherapy) is a novel contribution to the literature given that only two previous trials have provided evidence that group CB produces significantly greater reductions in depressive symptoms than alternative interventions (Merry et al., 2004; Stice et al., 2006), though these two prior trials only observed these effects from pretest to posttest. The present trial is the first to indicate that group CB significantly outperformed an alternative intervention through 1- and 2-year follow-up. Yet, it is important to acknowledge that group CB did not significantly reduce the risk for future onset of major or minor depression relative to either the supportive expressive or bibliotherapy, which is key outcome for a depression prevention intervention.
Another important finding is that risk for onset of major or minor depression over the 2-year follow-up was significantly lower for group CB participants (14%) and bibliotherapy participants (3%) relative to brochure controls (23%). It should be noted that baseline differences in depressive symptoms could not have contributed to these effects because group CB and bibliotherapy participants did not differ from controls on either baseline measure of depressive symptoms and because we controlled for baseline differences in depression in the analyses. This is an important finding because most group CB depression prevention programs have not reduced risk for future onset of depressive episodes during follow-up (Gillham et al., 2006; Seligman et al., 1999; Seligman et al., 2007; Sheffield et al., 2006), with only two exceptions (Clarke et al., 1995; 2001). Indicated prevention interventions target individuals with signs of a problem to prevent future onset of a clinically significant disorder that would warrant treatment. Although most participants in the present study did not develop major or minor depression during follow-up and thus did not require early intervention for newly emerging depression, two of the three active interventions received support as indicated depression prevention interventions. Of note, whereas group CB did not significantly reduce risk for onset of depressive episodes relative to the supportive expressive and CB bibliotherapy, data indicated that CB bibliotherapy produced marginally greater reductions in risk for future depressive episodes than both group CB and the supportive expressive intervention, though these effects should be interpreted with caution given that they were marginal and bibliotherapy participants entered the study at a slightly lower depression level, which may have impacted the incidence rates for depressive episodes in a manner that could not be statistically controlled.
The overall pattern of findings suggests that group CB produces significantly greater reductions in initial depressive symptoms than either the supportive expressive and CB bibliotherapy during and after intervention, but that CB bibliotherapy produced marginally greater reductions in risk for onset of future depressive episodes relative to both group CB and the supportive expressive intervention. Indeed, the incidence of new depressive episodes was lowest in the bibliotherapy condition (3%). It is possible that the significantly lower level of depressive symptoms reported on the interview (but not the BDI) at baseline for bibliotherapy participants relative to group CB and supportive expressive participants might have contributed to the lower incidence of depressive disorder, but this seems unlikely because we statistically controlled for baseline depressive symptom. Another explanation for the low incidence of depression in the bibliotherapy condition is that participants did not come into contact with other youth with elevated depressive symptoms, as they did in the two group interventions. A third explanation for the low incidence of depression in the bibliotherapy condition is that participants were able to return to the book if they experienced a worsening of depressive symptoms during the 2-year follow-up. In line with this interpretation, data suggest that participants in this condition read approximately 50 additional pages during follow-up. Although the present findings suggest that bibliotherapy has limited efficacy for reducing initial depressive symptoms in high-risk youth, results do suggest that this intervention prevents future onset of depressive episodes over a long period of time.
It was curious that CB bibliotherapy appeared to be effective at reducing risk for future onset of depressive episodes, yet was ineffective at reducing initial depressive symptoms, particularly given that the reduction in depressive symptoms should have resulted in reduced risk for future onset of depressive episodes. This pattern of findings seems to suggest that nonspecific factors associated with group interventions are particularly effective in reducing initial depressive symptoms, such as discussing feeling of depression and triggers for these emotions and the realization that other adolescents in the school are having similar experiences.
Although it is more common to conduct detailed costing analyses in effectiveness or dissemination trials, rather than efficacy trials, we calculated the basic costs of delivering group CB verses CB bibliotherapy for participants in this trial. Facilitators were paid approximately $15 per hour and spent approximately 15 hours conducting each group (e.g., initial training, setup and actual intervention delivery, make-up sessions, group supervision). Costs for staff and supervision are estimated at $645 per group. This translates into $80 per student, as opposed to $8 per student for the cost of the self-help book used in bibliotherapy.
The incidence of depressive episodes in the present study was lower than some previous reports examining indicated depression prevention programs (e.g., Clarke et al., 1995; 2001; Garber et al., 2009; Gillham et al., 2006). It appears that this difference emerged because we recruited participants on the basis of a single risk factor whereas some trials required that participants have two risk factors (e.g., elevated symptoms and a parental history of depression). Depression incidence for non-intervention control groups was higher in double versus single risk factor studies (1-year depression onset rates of approximately 29% vs. 22%, respectively). The incidence in the present study for the control participants is comparable to other single risk factor studies. Thus, it appears that we had less power to detect differential risk of future depressive episode onset relative to indicated trials involving doubly at-risk youth.
It was also noteworthy that the BDI was less sensitive in detecting the effects of these prevention programs than interview-assessed depressive symptoms. Only one of the four effects that were significant for the interviewer-based depressive symptom measure emerged with the BDI. Results suggest that although is it more cumbersome and expensive, blinded diagnostic interviews provide a more sensitive measure of depressive symptoms in prevention trials, presumably because interviews assessed symptom severity during the entire period of time since the last assessment, as opposed to the past two weeks for the BDI. This interpretation suggests that it is critical to capture symptom fluctuation, including peak symptom severity, during the follow-up period in prevention trials. It is also possible that the BDI was less sensitive than the K-SADS interview because the former taps more self-perceived distress and the latter is a more objective indicator of depressive symptom severity. Researchers conducting efficacy and effectiveness trials in the area of depression prevention and treatment are encouraged to collect and report both interviewer-based and survey measures of adolescent depression to better understand the ability of both measures to detect change and to inform future large dissemination trials, in which it may be feasible to only use surveys to assess depressive symptoms.
Although the group CB depression prevention program resulted in improved social adjustment relative to the supportive expressive intervention, bibliotherapy, and educational brochure controls through 6-month follow-up (Stice, Rohde et al., 2008), these effects did not persist through 1- and 2-year follow-up. It might be argued that this measure was not sufficiently sensitive to detect intervention effects on social functioning over such a long period, but we have observed intervention effects using this same measure through 3-year follow-up in another prevention trial (Stice, Marti et al., 2008). The pattern of results in the present trial suggest that it might be useful to consider ways to refine the group CB prevention program so that it produces more lasting effects on psychosocial functioning (e.g., by having the home exercises focus on improving social functioning). To keep our CB intervention brief, we focused almost exclusively on cognitive restructuring and behavior activation and did not include additional CB skills for depression, such as social skills, communication, and problem-solving, which might lead to more persistent improvements in functioning at home, school, and with peers. Other depression prevention programs, particularly those developed by Seligman, Gillham, and colleagues (Gillham et al., 2007; Seligman et al., 1999), have included a broader range of skills, including interpersonal skills and problem-solving, but no depression prevention intervention to our knowledge has found long-term effects for social adjustment or psychosocial functioning.
Limitations of this trial should be noted. First, over 20% of the sample did not participate in the final follow-up assessment. Although there was no indication of differential attrition across intervention conditions or as a function of demographic variables, it was possible that incidence of depressive episodes might have been higher with a complete sample. Second, this report relies solely on adolescent-based data rather than multiple informants, although parent report data can introduce additional complications to interpretation and adolescent reports of depression are considered the most reliable and valid single source of data in the area of depression (e.g., Cantwell, Lewinsohn, Rohde, & Seeley, 1997). Third, it would have been informative to collect objective measures of social adjustment, such as grades and school attendance, and parental report of functioning in the home. Fourth, data were not collected on other outcomes that might have been affected by these interventions (e.g., anxiety disorders) because of concerns regarding respondent burden. Lastly, group CB and supportive expressive participants were nested within groups, which may have contributed to non-independent data regarding change in the outcomes and increased risk for chance findings (Kenny & Judd, 1986).
In conclusion, results from this indicated prevention trial suggest that this brief CB depression prevention program produces clinically meaningful and long-lasting effects, including both reductions in initial depressive symptoms in a high-risk population that persist for more than one year as well as reduced risk for future depressive episodes over a two-year follow-up period. The reductions in depressive symptoms for group CB were superior to bibliotherapy but not relative to a nondirective alternative group intervention, suggesting that nonspecific factors associated with any psychosocial intervention may have significant depression prevention effects for at-risk adolescents. Although group CB was not significantly superior to the alternative group intervention, the supportive expressive control intervention did not reduce depressive symptoms or the incidence of depressive episodes relative to the educational brochure control condition, implying that the group CB prevention program was more efficacious. Whereas the results in terms of reductions in depressive symptoms and risk for depressive episodes favored the group CB program, the fact that CB bibliotherapy significantly reduced risk for future depressive episodes relative to group CB, supportive expressive, and brochure control participants is noteworthy. If replicated, the preventive effects for bibliotherapy have important public health implications, given the ease of dissemination and low cost of this intervention. In addition to independent replication, future research should examine ways of increasing the effects of both CB prevention interventions, including more effective methods of identifying at-risk adolescents, motivating them to attend sessions or read bibliotherapy material, improving homework compliance, greater generalization of CB material to important aspects of the lives, and methods for maintaining the gains that are achieved. One potentially significant improvement would be supplementing group CB with bibliotherapy. Finally, research in the area of indicated prevention for adolescent depression needs to begin investigating and addressing the barriers to wide-scale dissemination of empirically supported depression prevention interventions. Clear gains are being made in the prevention of adolescent depression and given a programmatic and scientifically rigorous body of research, we may yet realize the ultimate goal of reducing the prevalence of depression through prevention.
Acknowledgments
This study was supported by a research grants MH67183 and MH80853 from the National Institute of Health.
Thanks go to project research assistants, Courtney Byrd, Kathryn Fischer, Amy Folmer, Cassie Goodin, Jacob Mase, and Emily Wade, a multitude of undergraduate volunteers, the Austin Independent School District, and the participants who made this study possible.
Footnotes
The proportion of assigned homework assignments completed by participants in the CB group was counted for each session they attended and correlated with change in depressive symptom scores from baseline to each of the post baseline assessments. The correlation of the homework score with change in depressive symptoms from baseline to posttest was r = .24 (p = .026) indicating that group CB participants who completed more homework assignments showed greater decreases in depressive symptom scores. Correlations with homework completion and change in depressive symptom scores at the 6-month, 1-year, and 2-year follow-up assessments were nonsignificant.
Contributor Information
Eric Stice, Department of Psychology, University of Texas at Austin.
Paul Rohde, Oregon Research Institute.
Jeff M. Gau, Oregon Research Institute
Emily Wade, Department of Psychology, University of Texas at Austin.
References
- American Psychological Association Task Force on Psychological Intervention Guidelines. Template for developing guidelines: Interventions for mental disorders and psychological aspects of physical disorders. Washington, DC: APA; 1995. [Google Scholar]
- Burns DD. Feeling Good: The New Mood Therapy. New York: William Morrow & Company; 1980. [Google Scholar]
- Beck AT, Steer RM, Garbin M. Psychometric properties of the Beck Depression Inventory: 25 years of evaluation. Clinical Psychology Review. 1988;8:77–100. [Google Scholar]
- Brent DA, Holder D, Kolko D, Birmaher B, Baugher M, Roth C, Iyengar S, Johnson BA. A clinical psychotherapy trial for adolescent depression comparing cognitive, family, and supportive therapy. Archives of General Psychiatry. 1997;54:877–885. doi: 10.1001/archpsyc.1997.01830210125017. [DOI] [PubMed] [Google Scholar]
- Cantwell DP, Lewinsohn PM, Rohde P, Seeley JR. Correspondence between adolescent report and parent report of psychiatric diagnostic data. Journal of the American Academy of Child and Adolescent Psychiatry. 1997;36:610–619. doi: 10.1097/00004583-199705000-00011. [DOI] [PubMed] [Google Scholar]
- Carver RP. Reading rate: A review of research and theory. San Diego: Academic Press, Inc; 1990. [Google Scholar]
- Clarke G, Hawkins W, Murphy M, Sheeber L, Lewinsohn PM, Seeley JR. Targeted prevention of unipolar depressive disorder in an at-risk sample of high school adolescents: A randomized trial of group cognitive intervention. Journal of the American Academy of Child and Adolescent Psychiatry. 1995;34:312–321. doi: 10.1097/00004583-199503000-00016. [DOI] [PubMed] [Google Scholar]
- Clarke GN, Hornbrook M, Lynch F, Polen M, Gale J, Beardslee W, O’Connor E, Seeley J. A randomized trial of a group cognitive intervention for preventing depression in adolescent offspring of depressed parents. Archives of General Psychiatry. 2001;58:1127–1134. doi: 10.1001/archpsyc.58.12.1127. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analyses for the behavioral sciences. New Jersey: Lawrence Erlbaum; 1988. [Google Scholar]
- Garber J, Clarke GN, Weersing VR, Beardslee WR, Brent DA, Gladstone TRG, DeBar LL, Lynch FL, D’Angelo E, Hollon SD, Shamseddeeen W, Iyengar S. Prevention of depression in at-risk adolescents: A randomized controlled trial. Journal of the American Medical Association. 2009;301:2215–2224. doi: 10.1001/jama.2009.788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillham JE, Hamilton J, Freses DR, Patton K, Gallop R. Preventing depression among early adolescents in the primary care setting: A randomized controlled study of the Penn Resiliency Program. Journal of Abnormal Child Psychology. 2006;34:203–219. doi: 10.1007/s10802-005-9014-7. [DOI] [PubMed] [Google Scholar]
- Gillham JE, Reivich KJ, Freres DR, Chaplin TM, Shatte AJ, Samuels B, et al. School-based prevention of depressive symptoms: A randomized controlled study of the effectiveness and specificity of the Penn Resiliency Program. Journal of Consulting and Clinical Psychology. 2007;75:9–19. doi: 10.1037/0022-006X.75.1.9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillham JE, Reivich KJ, Freres DR, Lascher M, Litzinger S, Shatte A, Seligman ME. School-based prevention of depression and anxiety symptoms in early adolescence: A pilot of a parent intervention component. School Psychology Quarterly. 2006;21:323–348b. [Google Scholar]
- Horowitz JL, Garber J. The prevention of depressive symptoms in children and adolescents: A meta-analytic review. Journal of Consulting and Clinical Psychology. 2006;74:401–415. doi: 10.1037/0022-006X.74.3.401. [DOI] [PubMed] [Google Scholar]
- Horowitz JL, Garber J, Ciesla JA, Young J, Mufson L. Prevention of depressive symptoms in adolescents: a randomized trial of cognitive-behavioral and interpersonal prevention programs. Journal of Consulting and Clinical Psychology. 2007;75:693–706. doi: 10.1037/0022-006X.75.5.693. [DOI] [PubMed] [Google Scholar]
- Jacobson NS, Truax P. Clinical significance: A statistical approach to defining change in psychotherapy research. Journal of Consulting and Clinical Psychology. 1991;59:12–19. doi: 10.1037//0022-006x.59.1.12. [DOI] [PubMed] [Google Scholar]
- Jaycox LH, Reivich KJ, Gillham J, Seligman MEP. Prevention of depressive symptoms in school children. Behavioral Research and Therapy. 1994;32:801–816. doi: 10.1016/0005-7967(94)90160-0. [DOI] [PubMed] [Google Scholar]
- Kaufman J, Birmaher B, Brent D, Rao U, Ryan N. The schedule for affective disorders and schizophrenia for school-age children. University of Pittsburgh Medical Center; Pittsburgh: 1996. [Google Scholar]
- Klein DN, Torpey DC, Bufferd SJ. Depressive disorders. In: Beauchaine TP, Hinshaw SP, editors. Child and Adolescent Psychopathology. 2008. pp. 477–509. [Google Scholar]
- Kenny DA, Judd CM. Consequences of violating the independence assumption in analysis of variance. Psychological Bulletin. 1986;99:422–431. [Google Scholar]
- Lewinsohn PM, Roberts RE, Seeley JR, Rohde P, Gotlib IH, Hops H. Adolescent psychopathology: II. Psychosocial risk factors for depression. Journal of Abnormal Psychology. 1994;103:302–315. doi: 10.1037//0021-843x.103.2.302. [DOI] [PubMed] [Google Scholar]
- Merry S, McDowell H, Wild C, Bir J, Cunliffe R. A randomized placebo-controlled trial of a school-based depression prevention program. Journal of the American Academy of Child and Adolescent Psychiatry. 2004;43:538–547. doi: 10.1097/00004583-200405000-00007. [DOI] [PubMed] [Google Scholar]
- Newman DL, Moffitt TE, Caspi A, Magdol L, Silva PA, Stanton WR. Psychiatric disorder in a birth cohort of young adults: Prevalence, comorbidity, clinical significance, and new case incidence from ages 11 to 21. Journal of Consulting and Clinical Psychology. 1996;64:552–562. [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Stice E, Wade E, Bohon C. Reciprocal relations between rumination and bulimic, substance abuse, and depressive symptoms in adolescent females. Journal of Abnormal Psychology. 2007;116:198–207. doi: 10.1037/0021-843X.116.1.198. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Schafer JL. NORM: multiple imputation of incomplete data under normal model, version 2.03, software for Windows 95/98/NT, available from. 1999 < www.stat.psu.edu/~jls/misoftwa.html>.
- Seeley J, Stice E, Rohde P. Screening for depression prevention: Identifying adolescent girls at high risk for future depression. Journal of Abnormal Psychology. 2009;118:161–170. doi: 10.1037/a0014741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seligman ME, Schulman P, DeRubeis RJ, Hollon SD. The prevention of depression and anxiety. Prevention and Treatment. 1999:2. [Google Scholar]
- Seligman ME, Schulman P, Tryon AM. Group prevention of depression and anxiety symptoms. Behaviour Research and Therapy. 2007;45:1111–1126. doi: 10.1016/j.brat.2006.09.010. [DOI] [PubMed] [Google Scholar]
- Shaw BF. Comparison of cognitive therapy and behavior therapy in the treatment of depression. Journal of Consulting and Clinical Psychology. 1977;45:543–551. doi: 10.1037//0022-006x.45.4.543. [DOI] [PubMed] [Google Scholar]
- Sheffield JK, Spence SH, Rapee R, Kowalenko N, Wignall A, Davis A, McLoone J. Evaluation of universal, indicated, and combined cognitive-behavioral approaches to the prevention of depression among adolescents. Journal of Consulting and Clinical Psychology. 2006;74:66–79. doi: 10.1037/0022-006X.74.1.66. [DOI] [PubMed] [Google Scholar]
- Shochet IM, Dadds MR, Holland D, Whitefield K, Harnett PH, Osgarby SM. The efficacy of a universal school-based program to prevent adolescent depression. Journal of Clinical Child Psychology. 2001;30:303–315. doi: 10.1207/S15374424JCCP3003_3. [DOI] [PubMed] [Google Scholar]
- Spence SH, Sheffield JK, Donovan CL. Preventing adolescent depression: An evaluation of the problem solving for life program. Journal of Consulting and Clinical Psychology. 2003;71:3–13. doi: 10.1037//0022-006x.71.1.3. [DOI] [PubMed] [Google Scholar]
- Stice E, Burton E, Bearman SK, Rohde P. Randomized trial of a brief depression prevention program: An elusive search for a psychosocial placebo control condition. Behaviour Research and Therapy. 2006;45:863–876. doi: 10.1016/j.brat.2006.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Marti N, Spoor S, Presnell K, Shaw H. Dissonance and healthy weight eating disorder prevention programs: Long-term effects from a randomized efficacy trial. Journal of Consulting and Clinical Psychology. 2008;76:329–340. doi: 10.1037/0022-006X.76.2.329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Rohde P, Seeley J, Gau J. Brief cognitive-behavioral depression prevention program for high-risk adolescents outperforms two alternative interventions: A randomized efficacy trial. Journal of Consulting and Clinical Psychology. 2008;76:595–606. doi: 10.1037/a0012645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Rohde P, Seeley J, Gau J. Testing mediation of intervention effects in randomized trials: An evaluation of three depression prevention programs. Journal of Consulting and Clinical Psychology. 2010;78:273–280. doi: 10.1037/a0018396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Shaw H. Eating disorder prevention programs: A meta-analytic review. Psychological Bulletin. 2004;130:206–227. doi: 10.1037/0033-2909.130.2.206. [DOI] [PubMed] [Google Scholar]
- Stice E, Shaw H, Marti CN. A meta-analytic review of obesity prevention programs for children and adolescents: The skinny on interventions that work. Psychological Bulletin. 2006;132:667–691. doi: 10.1037/0033-2909.132.5.667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice E, Shaw H, Bohon C, Marti CN, Rohde P. A meta-analytic review of depression prevention programs for children and adolescents: Factors that predict magnitude of intervention effects. Journal of Consulting and Clinical Psychology. 2009;77:486–503. doi: 10.1037/a0015168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weissman MM, Fendrich M, Warner V, Wickramaratne P. Incidence of psychiatric disorder in offspring at high and low risk for depression. Journal of the American Academy of Child and Adolescent Psychiatry. 1992;31:640–648. doi: 10.1097/00004583-199207000-00010. [DOI] [PubMed] [Google Scholar]
- Weissman MM, Orvaschel H, Padian N. Children’s symptom and social functioning self-report scales: Comparison of mothers’ and children’s reports. Journal of Nervous and Mental Disease. 1980;168:736–740. doi: 10.1097/00005053-198012000-00005. [DOI] [PubMed] [Google Scholar]