

Abstract
Primary osteosarcoma is a common malignant bone tumour that principally affects the long bones, but relatively rare in flat bones, in children and adolescents. This study presents a rare case of primary rib osteosarcoma in a 59-year old man. The patient underwent second radical excision of the tumour due to a short time relapse after the first operation. Chest wall reconstruction, neoadjuvant chemotherapy before the second operation and postoperative chemotherapy were also performed. To date, 5 months have passed with no recurrence being observed.
Keywords: Rib, Osteosarcoma, Recurrence, Management, Adult
INTRODUCTION
Osteosarcoma is the most common primary malignant bone tumour which principally occurs during childhood and adolescence. Osteosarcoma is often found in the metaphysis of long bones [1]; however, its occurrence as a primary tumour in the rib is rare in adults [2]. This study describes a rare case of primary rib osteosarcoma, which relapsed in a short time, and its subsequent successful management in a 59-year old man.
CASE REPORT
A 59-year old man presented increasing right-sided chest pain and weight loss prior to admission. At the outset, he reported intermittent right-sided chest pain, which later became constant and more severe, particularly at night, for approximately 4 months. He had undergone radiological examination before admission, but no significant information could be observed from the chest radiography film or computed tomography (CT) scan of the chest. Moreover, positron emission tomography (PET)-CT showed that the shape of the right fifth rib was normal. However, a collection of radioactive materials in the anterolateral section of the right fifth rib was observed (Fig. 1A). The patient reported severe right chest pain and weight loss (approximately 10 kg) upon admission, but his physical examination revealed no abnormality. Moreover, the results of the haematological examination were roughly normal. However, the alkaline phosphatase (ALP) level was relatively higher. Bone emission computed tomography (ECT) showed abnormal tracer concentration in the right fourth and fifth ribs (Fig. 1B). After sufficient preoperative preparation, a part of the fourth and fifth ribs was extensively removed, together with adjacent intercostal muscles. Postoperative histopathological outcome confirmed an osteosarcoma originating from the rib. Furthermore, immunohistochemistry staining showed sporadic positive staining of CD99 and S-100, as well as negative staining of myogenin, MyoD1 and cytokeratin (CK) (Fig. 2).
Figure 1:
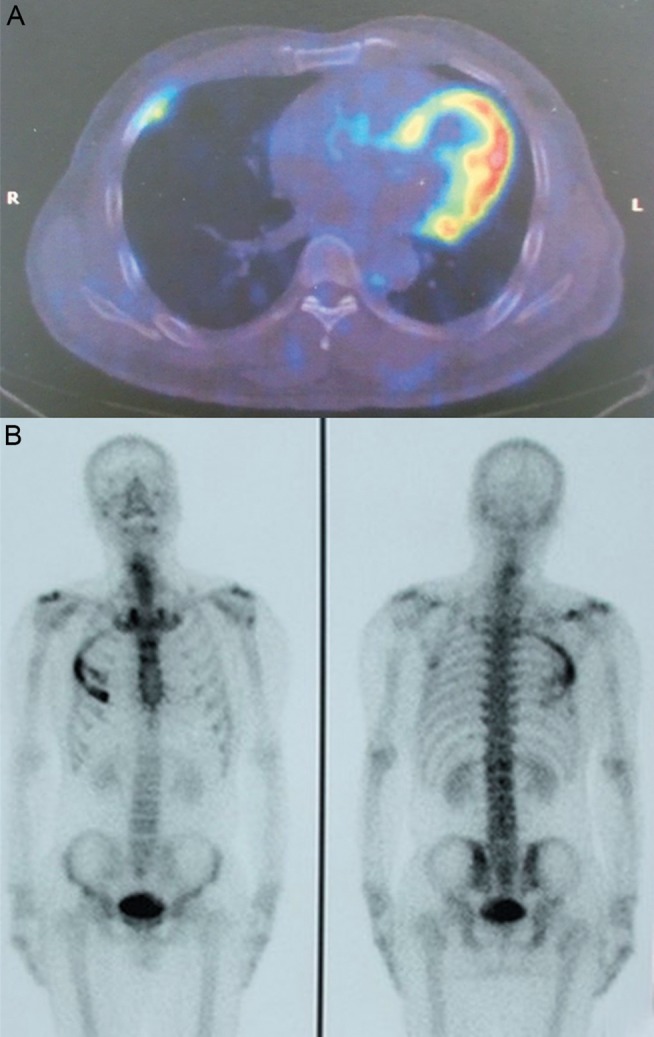
(A) PET-CT showed a collection of radioactive material in the anterolateral section of the right fifth rib despite the normal shape of the rib. (B) Bone ECT showed abnormal tracer concentration in the right fourth and fifth ribs.
Figure 2:
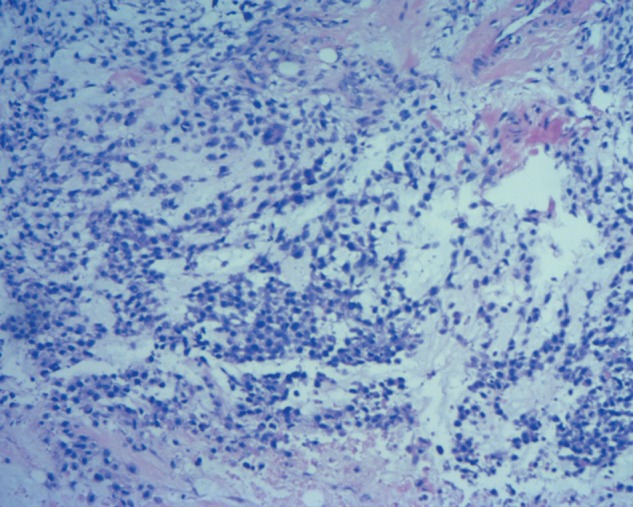
The postoperative histopathological outcome and immunohistochemistry staining showed sporadic positive staining of CD99 and S-100, as well as negative staining of myogenin, MyoD1 and CK, in the osteosarcoma originating from the rib.
The patient was readmitted to our department because of severe chest pain after approximately 1 month. The level of ALP was higher than the postoperative value. The chest CT still did not provide sufficient informative images of masses. The PET-CT showed a radioactive material concentrated in the right fourth to sixth ribs, and the bone ECT also revealed abnormal tracer concentration therein. We considered that rib osteosarcoma may have recurred and affected the adjacent ribs. To optimize efficacy, the patient underwent neoadjuvant chemotherapy and a second operation. Recurring rib osteosarcoma and tumour invasion infiltrating a part of the diaphragm and superior lobe of the right lung were found during the operation. Thus, proximal resection of the right fourth to seventh ribs, adjacent intercostal muscles, a part of the invasive diaphragm and the superior lobe of the right lung were resected. Right thoracoplasty and reconstruction of the affected chest wall defect were performed using titanium plates. The postoperative histopathological outcome was consistent with the preoperative diagnosis. Given the tumour recurrence and involvement of adjacent tissues, the patient underwent postoperative chemotherapy. To date, 5 months have passed and he has not complained of any right chest pain. The ALP level has recovered and maintains a normal value since the second surgery. No evidence for tumour recurrence, enlarged mediastinal nodes or focal lung lesions has been observed.
DISCUSSION
Osteosarcoma is most often found in the metaphysis of long bones [1], but is relatively rare in flat bones. Approximately 70–75% of cases occur between 10 and 25 years of age [2]. Osteosarcoma occurring as a tumour of the rib is rare [2], especially in adults.
The most common presentations of primary rib osteosarcoma are chest pain and a palpable chest wall mass [3]. The ALP levels are meaningful for the diagnosis and prognosis of primary rib osteosarcoma [4]. In the present case, the change in chest pain was consistent with the ALP level. However, a palpable chest wall mass was not found. Bone ECT and PET-CT are important in the diagnosis of the tumour because of the negative outcome of the chest X-ray and CT. Histopathological findings as the gold standard confirm the diagnosis of rib osteosarcoma.
The standard therapy for osteosarcoma is a combination of chemotherapy and surgery [1]; however, a significant number of patients with standard therapy will still relapse [5]. The risk factors for recurrence after surgery are still unknown due to the rarity of rib osteosarcoma. Several independent risk factors associated with the probability of developing recurrences, which can only be obtained from several studies of long-bone osteosarcoma, may include the axial site and the large size of the primary tumour, primary metastases and poor response to first-line chemotherapy [5]. In the present case, the incomplete surgical removal of tumour foci in the first operation should also be included in the risk factors for recurrence.
To promptly detect the relapse of rib osteosarcoma, the significance of detecting measures should be highlighted. Routine chest radiography, CT scans, PET-CT, bone ECT and testing of ALP level are always utilized to detect the relapse of rib osteosarcoma. In the present case, the importance of PET-CT and bone ECT has been confirmed, and the ALP level is a significant indicator for inspecting the severity of rib osteosarcoma.
Relapsed therapy of osteosarcoma is not standardized; however, surgical removal of all detectable tumour foci is recommended whenever feasible [5]. Therefore, reoperation should be carried out based on the confirmation of recurrence and having no distant metastases. Meanwhile, postoperative chemotherapy will greatly improve patient survival [3].
In conclusion, this study presents a rare case of primary rib osteosarcoma relapsing in a short time after the first operation as well as its successful management. Haematological examination for the ALP level, bone ECT and PET-CT are important measures to detect the recurrence of primary rib osteosarcoma. The optimal therapy is a combination of neoadjuvant chemotherapy, second radical operation and postoperative chemotherapy once relapse of rib osteosarcoma is observed. The resection range should at least include the adjacent rib beyond the primary rib osteosarcoma. If possible, preoperative biopsy of tumour under local anaesthesia should be taken to confirm the pathological type and to decide the subsequent resection range.
Conflict of interest: none declared.
REFERENCES
- 1.Mueller F, Fuchs B, Kaser-Hotz B. Comparative biology of human and canine osteosarcoma. Anticancer Res. 2007;27:155–64. [PubMed] [Google Scholar]
- 2.Deitch J, Crawford AH, Choudhury S. Osteogenic sarcoma of the rib: a case presentation and literature review. Spine. 2003;28:E74–7. doi: 10.1097/01.BRS.0000048507.31949.E8. [DOI] [PubMed] [Google Scholar]
- 3.Lim W, Ahmad Sarji S, Yik Y, Ramanujam T. Osteosarcoma of the rib. Biomed Imaging Interv J. 2008;4:e7. doi: 10.2349/biij.4.1.e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Garzotto CK, Berg J, Hoffmann WE, Rand WM. Prognostic significance of serum alkaline phosphatase activity in canine appendicular osteosarcoma. J Vet Intern Med. 2000;14:587–92. doi: 10.1892/0891-6640(2000)014<0587:psosap>2.3.co;2. [DOI] [PubMed] [Google Scholar]
- 5.Kempf-Bielack B, Bielack SS, Jürgens H, Branscheid D, Berdel WE, Exner GU, et al. Osteosarcoma relapse after combined modality therapy: an analysis of unselected patients in the Cooperative Osteosarcoma Study Group (COSS) J Clin Oncol. 2005;23:559–68. doi: 10.1200/JCO.2005.04.063. [DOI] [PubMed] [Google Scholar]