

Abstract
Introduction The fossa of Rosenmüller, also known as the lateral pharyngeal recess, is a well-established site of origin of nasopharyngeal carcinoma. It is located in the lateral pharyngeal wall behind the cartilaginous portion of the Eustachian tube, the torus tubarius, and is named after Johann Christian Rosenmüller (JCR).
Objective We present a history on the life and extensive works of Johann Christian Rosenmüller, a German physician and anatomist.
Results Johann Christian Rosenmüller was a dedicated anatomist. In addition to identifying the fossa of Rosenmüller, his influence extends to various other anatomic subjects, including the Rosenmüller gland, the palpebral portion of the lacrimal gland, and the organ of Rosenmüller (i.e., the caudal remnant of the mesonephric duct). He was also an avid speleologist, studying the composition of caves and their life forms. For his contributions to this field, he had a cave in Germany and an extinct species named after him—Rosenmüllerhöhle and Ursus spelaeus Rosenmüller, respectively.
Conclusion The fossa of Rosenmüller plays an important role in the growth and surgical treatment of nasopharyngeal carcinoma. We present a brief glimpse into the life of Johann Christian Rosenmüller, for whom it was named.
Keywords: fossa of rosenmüller, johann christian rosenmüller, nasopharyngeal carcinoma, history
Introduction
The fossa of Rosenmüller is a bilateral projection of the nasopharynx just below the skull base. It is also called the lateral pharyngeal recess or simply the pharyngeal recess. The fossa is covered by nasopharyngeal mucosa and is the most common site of origin of nasopharyngeal carcinoma (NPC). NPC is a highly malignant neoplasm and is the most common malignant neoplasm of the nasopharynx. Although the incidence of NPC is relatively rare worldwide at under 1 per 100,000, it is quite common in some regions of China, Southeast Asia, and Africa—up to almost 25 per 100,000.1 As the early symptoms of NPC may mimic benign ear conditions, the most common presentation of NPC is cervical lymphadenopathy, which is an advanced stage of the disease and may preclude surgical intervention for local control. This lends importance to early detection and analysis of the site of origin of NPC, the fossa of Rosenmüller. The anatomy of the fossa was first described in 1808 by Johann Christian Rosenmüller.2
Family History
Johann Christian Rosenmüller (JCR) was born on May 25, 1771, in Hessberg, a town in the area now called Veilsdorf in the district of Hildburghausen, Thuringia, Germany (Fig. 1). His father, Johann Georg Rosenmüller (1736 to 1815), was a German protestant theologian and well-known orator. JCR's passion for his studies was instilled in him by his father, who became a professor of theology and divinity at Erlangen and Giessen, two of the more prominent universities in Germany, and later became a professor at Leipzig University. His father became well known for his works on the history of biblical translations.3 JCR's only sibling, an older brother Ernst Friedrich Karl Rosenmüller (1768 to 1835) was an orientalist and theologian, following in their father's footsteps and actually studying under their father at Leipzig University. All three Rosenmüllers were at Leipzig University from 1786 until their respective passing, with the two younger ones studying there initially and then eventually becoming faculty at the university like their father. The only exception was from 1792 to 1794, when JCR left for a short stint at Erlangen. There is no mention of JCR's mother in the literature and he was never married. Although his father and brother took a more philosophical path, JCR combined his passions for illustrations, adventure, and medicine and began a long history of significant contributions to the academic field, as detailed below.
Fig. 1.
Picture of Johann Christian Rosenmüller. (Public domain).
Academic and Medical History
JCR began his academic life in schools in Königsberg, Bavaria. He went on to high school in Erfurt, the capital city of Thuringia. At a young age, it was obvious that JCR had a great talent for illustrations. After a short stay at the University of Giessen, he proceeded to the University of Leipzig in 1786, at the young age of 15, where he spent the bulk of his academic career. In 1792, he graduated with a Magister's (Master of Arts) degree. He then went on to the University of Erlangen, where he began his studies in medicine. After 2 years, he returned to Leipzig and continued his medical training. Secondary to his passions and illustrative talent, he was appointed prosector of the Anatomical Theater, dissecting cadavers for anatomic demonstrations. JCR received his doctorate in 1797 as a doctor of medicine and became a general practitioner in Leipzig in 1799. In 1802, he was appointed associate professor of anatomy and surgery at Leipzig.4
JCR became the medical assessor faculty at the University of Leipzig in 1804, succeeding Ernst Benjamin Gottlieb Hebenstreit, who died in 1803. From 1804 to 1812, he was a Professor of Anatomy and Surgery at the University. He then became the Dean of the Medical Faculty in 1812, and he held this position until 1820. During this time, he also held the position “Rector of the University of Leipzig” (President of the University) three times: the summer sessions in 1816 and 1818, and the winter session in 1818. Throughout this time, his scientific career continued to gain greater recognition. Other prominent awards include:
1806-1809: Appointed Universitätsphysikus; he was called on during this time as the physician for prominent community figures, including high-ranking political prisoners.
1808: Admitted into the Leipzig Minerva Masonic Lodge.
1811: Appointed to the Royal Saxon Court as a Councillor.
1814: Awarded the Knight's Cross (3rd class) of the Russian Order of St. Wladimir.
After a long history with angina pectoris, JCR died of a sudden attack of his symptoms on the night of February 28, 1820. He was 49 years old and died just 5 years after his father.4 His grave site at Leipzig has since been destroyed, with only two inscriptions saved from the headstone: “Arzt und Anatom” (physician and anatomist). The headstone from his father's and brother's graves remains intact (Fig. 2).
Fig. 2.

Grave plaques for Ernst Friedrich Karl and Johann Georg Rosenmüller, [Alter Johannisfriedhof] Leipzig. (Licensed under Wikimedia Commons: Creative Commons License BY-SA 3.0. Available at: http://de.wikipedia.org/w/index.php?title=Datei:GrabtafelnRosenm%C3%BCller.JPG&filetimestamp=20120313013033. Accessed September 2012.
Other Achievements
Interestingly, JCR also specialized in speleology, the scientific study of caves, including their make-up, structure, and life forms. While still at Erlangen, he authored a book describing remarkable caves in the Muggendorf area, which was eventually published in 1796.5 Among these was one particular cave, now known as Rosenmüllerhöhle or Rosenmüller's Cave, discovered in 1793, which is still available for guided tours and presents an impressive image when lit by candlelight (Fig. 3A, B). In 1794, JCR as a young medical student and prosector, submitted and successfully defended his dissertation, entitled “Quaedam de ossibus cujusdam fossilibus animalis, ejus et cognitionem historiam accurationem illustrantis,” describing the fossil bones of what appeared to be a bear found in a cave in southeast Germany,6 now referred to as the Zoolithean Caves. His findings were published and focused on the prominence of these bones in caves and the specialized pattern of fusion of the cranial bones of the species7 (Fig. 4A, B). His subsequent studies and inability of other well-known scientists of his time to attribute this finding to any previous known species led to the establishment of the new subspecies Ursus spelaeus Rosenmüller, also known as the cave bear (Fig. 5), a species that had been long extinct at that time.6 His collection of fossil bones was initially thought to be lost but was rediscovered and now resides in the Museum für Naturkunde in Berlin.8
Fig. 3.
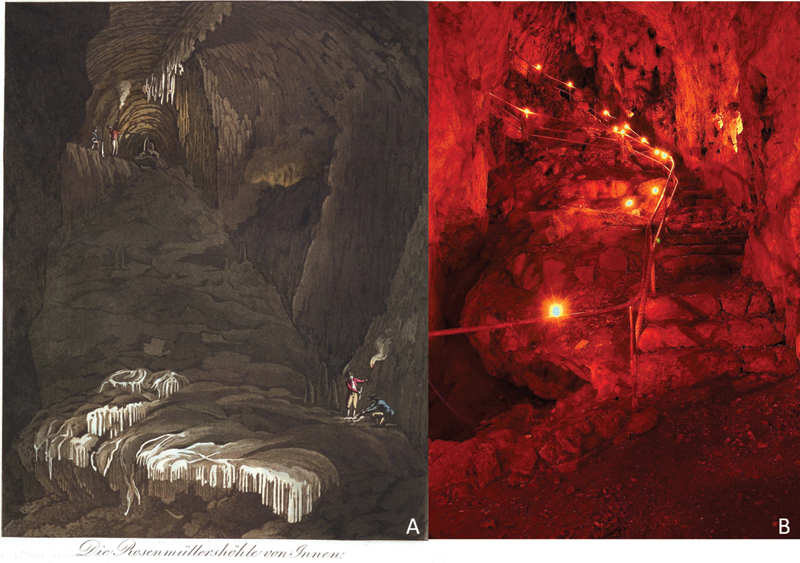
(A) Drawing of Rosenmüllerhöhle (public domain). (B) The candle-lit Rosenmüllerhöhle (by Molzberger, L: Licensed under Wikimedia Commons: Creative Commons License BY-SA 3.0. Available at: http://de.wikipedia.org/w/index.php?title=Datei:Rosenmuellerhoehle_01.jpg&filetimestamp=20081008120406. Accessed September 2012)
Fig. 4.
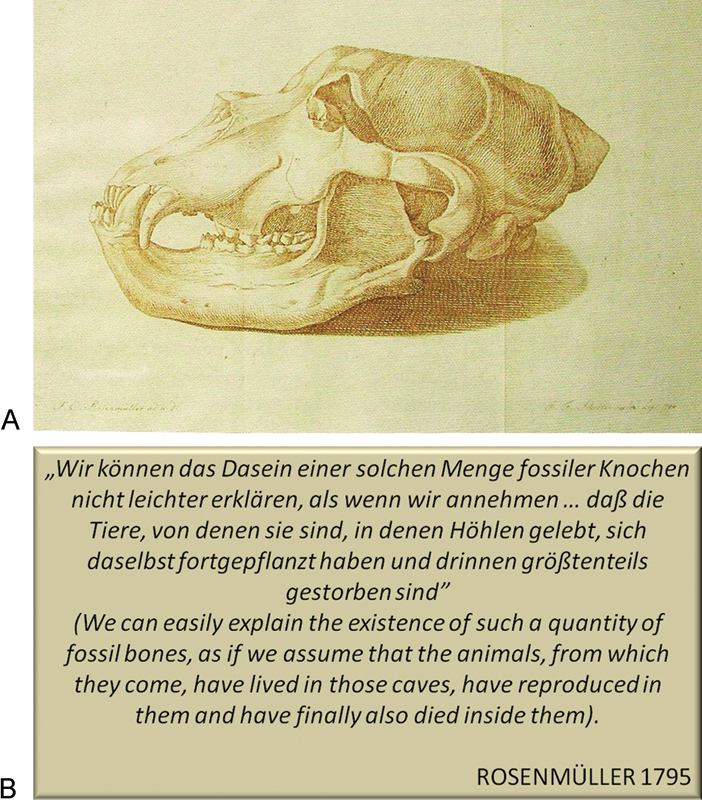
(A) The illustration of the holotype skull for the species Ursus spelaeus in the work of Rosenmüller 1795 from the “Zoolithenhöhle” near Burggaillenreuth (Franconian Alb). The specimen was thought to be lost but has been rediscovered and now resides in the Museum of Humboldt University in Berlin. (Public Domain). (B) Excerpt from Rosenmüller, 1795.
Fig. 5.
Reconstruction of a European cave bear (Ursus spelaeus). (by Sergiodlarosa. Licensed under Creative Commons License BY-SA 3.0. Available at: http://en.wikipedia.org/wiki/File:Ursus_spelaeus_Sergiodlarosa.jpg. Accessed September 2012).
JCR was the author of many dissertations, articles, and books (see select publications listed below), his crucial publication being a handbook of anatomy first published in 1808 and since edited multiple times (Fig. 6).2 It was almost 700 pages in length and contained detailed descriptions of parts of the human body, including the brain, nervous system, lungs, and reproductive tract. This was where the pharyngeal recess was first described. He was considered an expert in various anatomic topics, giving lectures and leading discussion on the olfactory nerve, the obturator nerve, and even aortic aneurysms. In addition to the fossa of Rosenmüller, he also had the palpebral portion of the lacrimal gland and the caudal remnant of the mesonephric duct named after him (Rosenmüller gland and organ of Rosenmüller, respectively). Selected works of JCR are listed in Table 1.
Fig. 6.
Cover page of one of the earlier editions of Rosenmüller's “Handbuch der Anatomie.”
Table 1. Selected works of Johann Christian Rosenmüller.
| Selected works of Johann Christian Rosenmüller |
|---|
| Quaedam de ossibus fossilibus animalis cuiusdam, historiam eius et cognitionem accuratiorem illustrantia. Dissertation in October 1794.(Roughly translated: Fossil bones of an animal, its history and detailed knowledge for the Library) |
| Illustrations and descriptions of strange caves around Muggendorf in Bayreutherischen highlands 1, Description of the cave bey Mockas [Texte imprimé]: for lovers of nature and art. Erlangen: Palm, 1796. |
| Partium externarum oculi humani inprimis lacrymalium descriptio anatomica iconibus illustrata. Leipzig 1797. (Roughly translated: A description of the external anatomy of the human eyes and lacrimation) |
| Beiträge für die Zergliederungskunst. Tauchnitz, Leipzig 1800/02 (3 Bde.; zusammen mit Heinrich Friedrich Isensenflamm). (Roughly translated: Contributions to Anatomy) |
| Quaedam de ovariis Embryonum et foetuum humanorum. Leipzig 1802. (Roughly translated: Development of the human fetal embryo) |
| Abbildungen Und Beschreibungen Der Fossilen Knochen Des Höhlenbären 1804. (Roughly translated: Illustrations and descriptions of fossil bones of the cave bear) |
| Chirurgisch-anatomische Abbildungen für Aerzte und Wundärzte. Weimar 1804-1812 (3 Bde.) (Roughly translated: Surgical and anatomical illustrations for doctors and surgeons) |
| Beschreibung merkwürdiger Höhlen: Ein Beitrag zur physikalischen Geschichte der Erde / herausgegeben Dr. Rosenmüller und Dr. Tilesius. 1805. (Roughly translated: Description remarkable caves: a contribution to the physical description of the earth) |
| Handbuch der Anatomie. Nach Lebers Umriss der Zergliederungskuns zum Gebrauch der Vorlesungen. 1815, 3. Aufl. Leipzig 1819. (Roughly translated: Handbook of Anatomy: After Leber's outline of anatomy to use in lectures) |
| Programma de Auatomicovum terminis technicis. Leipzig 1811. (Roughly translated: Technical terms in Anatomy) |
| Programma Nervi obturatorii monographia. Leipzig 1814. (Roughly translated: Obturator nerve monographs) |
He also edited works by other notable anatomists including Alexander Monro's (of Monro-Kellie Doctrine) Pictures and Descriptions of All the Bursae Mucosae of the Human Body (1799),9 John Bell's Anatomy and Physiology of the Human Body (1806),10 and works by Bell's younger brother, Sir Charles Bell (of Bell palsy, Bell-Magendie law).
Fossa of Rosenmüller
The lateral pharyngeal recess, or the fossa of Rosenmüller, is located behind the torus tubarius, a prominence caused by the medial cartilaginous end of the Eustachian tube (Fig. 7A, B).11 The torus is larger on the superior and posterior lips of the Eustachian tube, effectively hiding the fossa. The fossa is covered by nasopharyngeal mucosa and essentially extends through a defect between the fibers of the superior constrictor muscle and the base of the skull. The fibers of the superior constrictor muscle project from multiple parts of the lower oropharynx to the skull base, but the fibers only reach the skull base at the midline. The lateral defect, called the sinus of Morgagni, is covered by a fibrous band known as the nasopharyngeal aponeurosis. Therefore, the boundaries of the fossa of Rosenmüller are defined anteriorly by the Eustachian tube and levator palatini muscle, posteriorly by the posterior wall of the nasopharynx and the retropharyngeal space, laterally by the parapharyngeal space and the tensor veli palatini muscle, and inferiorly by the upper edge of the superior constrictor muscle. The fossa's superior boundary is the skull base with its various openings and prominences, including the foramen spinosum medially, the carotid canal, and the foramina spinosum and ovale. From its opening in the lateral nasopharynx, the fossa projects laterally behind the pharyngeal opening of the Eustachian tube ~1.5 cm in adults (Fig. 8). At the apex of the fossa of Rosenmüller, only a thin layer of fibroconnective tissue separates the mucosa from the cervical internal carotid artery.
Fig. 7.
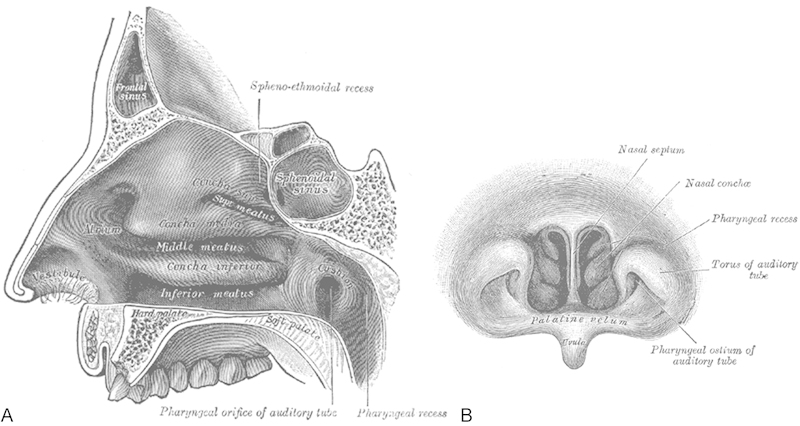
(A) Lateral wall of the nasopharynx. (B) Front of the nasopharynx as seen with a laryngoscope, depicting the pharyngeal recess (or fossa of Rosenmüller). (Gray, H. Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918. Public domain).
Fig. 8.
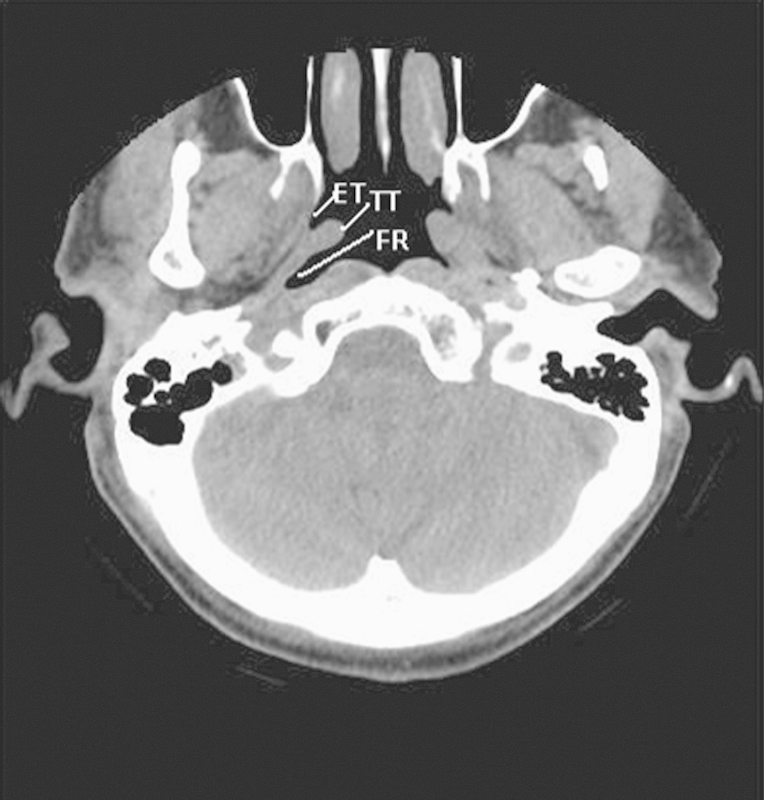
Axial computed tomography scan showing relationship between the Eustachian tube (ET), torus tubarius (TT), and fossa of Rosenmüller (FR).
Since Rosenmüller's description, much has been learned about the lateral pharyngeal recess. It was determined to be the most common site of origin of nasopharyngeal carcinoma (NPC). Hoe confirmed this in his review of computed tomography (CT) scans in ~60 patients with NPC and also found that the earliest sign on CT imaging of NPC was asymmetry and blunting of the fossa.12,13 Loh et al attempted to study the anatomy of the fossa on 23 CT scans. They found that the fossa projects at about a 45-degree angle from the sagittal plane and ranges in length from 1.7 mm to 18.8 mm with a relatively narrow orifice.14 This led them to conclude that the fossa was often too deep and narrow for clinical inspection with a nasopharyngoscope and could constitute a blind spot in the postnasal space, especially the floor of the fossa, which had clinical implications in the early detection of nasopharyngeal carcinoma. Hoe also found that deep infiltration of NPC was most commonly to the intracranial region, usually through the foramen lacerum and the foramen ovale.12 Usually, intracranial infiltration suggests very advanced disease with obliteration of what would be considered normal anatomy. Therefore, it would seem that knowledge of the anatomy of the fossa plays a more significant role during the early stages of the disease and in biopsy confirmation. However, in recent years, with the advent of and escalating use of the endoscope, reports of transnasal endoscopic resection of recurrent NPC has brought the focus back on basic anatomy.15,16,17
Secondary to the close relationship of the Eustachian tube, the fossa of Rosenmüller, and the internal carotid artery, there have been reports of serious complications where the fossa may have been mistaken for the Eustachian tube during treatment of some diseases of the Eustachian tube. For example, the injection of Teflon for treatment of a patulous Eustachian tube was discontinued secondary to complications of cerebral thrombosis and death when the paste was inadvertently injected into the internal carotid artery (ICA), likely because the injections were performed through the fossa instead of the Eustachian tube.18 Bergin et al went on study various distances in the area and found that the distance between the fossa and the ICA could be as small as 0.2 mm.18 This cements the importance of an intimate knowledge of the anatomy prior to any surgical interventions.
Conclusion
The fossa of Rosenmüller is the origin of nasopharyngeal carcinoma. This article provides a brief look into the interesting life of its discoverer, Johann Christian Rosenmüller, who made many noteworthy contributions to the academic world.
References
- 1.Yu M C, Yuan J M. Epidemiology of nasopharyngeal carcinoma. Semin Cancer Biol. 2002;12(6):421–429. doi: 10.1016/s1044579x02000858. [DOI] [PubMed] [Google Scholar]
- 2.Rosenmüller J C. Leipzig: Koehler; 1808. Handbuch der Anatomie: nach Lebers Umriss der Zergliederungskunst zum Gebrauch der Vorlesungen. [Google Scholar]
- 3.Siegfried C GA. “Rosenmüller, Johann George”, in: General German Biography. Historical Commission of the Bavarian Academy of Sciences 188929219–221. [Google Scholar]
- 4.Pagel J L. “Rosenmüller, Johann Christian”, in: General German Biography. Historical Commission of the Bavarian Academy of Sciences 188929221–222. [Google Scholar]
- 5.Rosenmüller J C, Tilesius von Tilenau W G. Erlangen: Palm; 1796. Illustrations and descriptions of strange caves around Muggendorf in Bayreutherischen highlands 1, Description of the cave bey Mockas [Texte imprimé]: for lovers of nature and art. [Google Scholar]
- 6.Rosenmüller J C. Quedam de ossibus fossilibus animalis cuiusdam, historiam eius et cognitionem accuratiorem illustrantia, dissertatio, quam d. 22. Octob. 1794 ad disputandum proposuit Ioannes Christ. Rosenmuller Hesberga-Francus, LL.AA.M. in Theatro anatomico Lipsiensi Prosector assumto socio Io. Chr. Aug. Heinroth Lips. Med. Stud. Cum tabula aenea. [Dissertation]. Leipzig, 17941–34.
- 7.Rosenmüller J C. Leipzig: Georg Emil Beer; 1795. Beiträge zur Geschichte und näheren Kenntniß fossiler Knochen. [Google Scholar]
- 8.Diedrich C G. The rediscovered cave bear “Ursus spelaeus Rosenmüller 1794” holotype of the Zoolithen Cave (Germany) from the historic Rosenmüller collection. Slovensky Kras acta carsologica slovaca. 2009;47:25–32. [Google Scholar]
- 9.Monro A. Liepzig: Breitkopf and Härtel; 1799. Abbildungen und beschreibungen der schleimsäcke des menschlichen körpers. [Google Scholar]
- 10.Bell J. Leipzig: Weidmannsche Buchhandlung; 1806. Zergliederung des menschlichen Körpers: Zum Behuf des Selbststudiums und akademischer Vorlesungen. [Google Scholar]
- 11.Gray H Anatomy of the Human Body. Philadelphia: Lea & Febiger, 1918; Bartleby.com, 2000 Available at: http://www.bartleby.com/107/. Accessed September 2012
- 12.Hoe J. CT of nasopharyngeal carcinoma: significance of widening of the preoccipital soft tissue on axial scans. AJR Am J Roentgenol. 1989;153(4):867–872. doi: 10.2214/ajr.153.4.867. [DOI] [PubMed] [Google Scholar]
- 13.Hoe J W. Computed tomography of nasopharyngeal carcinoma. A review of CT appearances in 56 patients. Eur J Radiol. 1989;9(2):83–90. [PubMed] [Google Scholar]
- 14.Loh L E, Chee T S, John A B. The anatomy of the Fossa of Rosenmuller—its possible influence on the detection of occult nasopharyngeal carcinoma. Singapore Med J. 1991;32(3):154–155. [PubMed] [Google Scholar]
- 15.Chen M Y, Wen W P, Guo X. et al. Endoscopic nasopharyngectomy for locally recurrent nasopharyngeal carcinoma. Laryngoscope. 2009;119(3):516–522. doi: 10.1002/lary.20133. [DOI] [PubMed] [Google Scholar]
- 16.Wen Y H, Wen W P, Chen H X, Li J, Zeng Y H, Xu G. Endoscopic nasopharyngectomy for salvage in nasopharyngeal carcinoma: a novel anatomic orientation. Laryngoscope. 2010;120(7):1298–1302. doi: 10.1002/lary.20958. [DOI] [PubMed] [Google Scholar]
- 17.Yoshizaki T, Wakisaka N, Murono S, Shimizu Y, Furukawa M. Endoscopic nasopharyngectomy for patients with recurrent nasopharyngeal carcinoma at the primary site. Laryngoscope. 2005;115(8):1517–1519. doi: 10.1097/01.MLG.0000165383.35100.17. [DOI] [PubMed] [Google Scholar]
- 18.Bergin M, Bird P, Cowan I, Pearson J F. Exploring the critical distance and position relationships between the Eustachian tube and the internal carotid artery. Otol Neurotol. 2010;31(9):1511–1515. doi: 10.1097/MAO.0b013e3181f6c880. [DOI] [PubMed] [Google Scholar]