

Abstract
There are several options for long head of the biceps (LHB) tenodesis and yet no standard of care. This technical note describes a cortical button technique for LHB tenodesis. We have taken the BicepsButton (Arthrex, Naples, FL) for distal biceps acute primary repair and applied it to the LHB. The biceps tenotomy is completed arthroscopically, and a standard subpectoral approach is used. The biceps is pulled out and whipstitched starting at the myotendinous junction and moving proximally. The humerus is drilled in a unicortical manner slightly larger than the tendon, and the button is passed through a small hole to the posterior cortex. A suture through the tendon provides additional fixation strength to the construct. This is an elegant and effective method of tenodesis that uses a smaller-diameter drill hole in the humerus. The goals of LHB tenodesis are to restore function, reduce pain, and improve cosmesis. This technique offers comparable function and cosmesis with the potential advantage of improving postoperative pain outcomes and lowering the rate of complications.
The indications for long head of the biceps (LHB) tenodesis include severe tendinitis/tendinosis, fraying/tearing of the proximal biceps tendon, or biceps instability usually associated with a rotator cuff tear.1 Many techniques have been described in the literature for proximal biceps tenodesis, including interference screws, suture anchors, soft-tissue fixation, bone tunnel, and many more.1-6 However, there is still no standard of care. The important outcomes remain pain, function, and cosmesis.1,3,6 The role of the LHB as a pain generator, in particular, demands the development of new methods of biceps fixation to minimize postoperative pain. This technical note describes a cortical button fixation technique for LHB tenodesis. To our knowledge, this technique has not yet been described in the literature. It is a safe, elegant, and effective method that uses a small drill hole, conserving bone, minimizing trauma to the tendon, and decreasing postoperative complications.
Surgical Technique
The cortical button used in this technique is the BicepsButton (Arthrex, Naples, FL). Although this product was designed for acute primary repair of distal biceps ruptures, it has a parallel application in LHB tenodesis. The patient is positioned in the lateral decubitus or beach-chair position. The surgery begins with a diagnostic shoulder arthroscopy. Two arthroscopic portals are used, anterior and posterior. Next, a tenotomy of the LHB is completed at its juncture with the biceps anchor, with an arthroscopic cutting instrument or a thermal ablator (Video 1, minute 0:31). A shaver may be used to debride the proximal stump.
Once the biceps tenotomy is confirmed arthroscopically, the portals are closed. If the patient is in the lateral decubitus position, the patient's bed is tilted slightly toward the operated shoulder. The arm is positioned along the patient's body, extended, and externally rotated to optimize the view for the subpectoral approach.
A standard subpectoral approach is used.4 A mini-incision measuring roughly 3.5 cm is centered over the inferior border of the pectoralis major tendon. A scalpel is used to cut down to the subcutaneous layer. Superficial soft tissue is dissected to expose the fascia covering the anteromedial border of the deltoid and inferior border of the pectoralis major muscle. The fascia is incised from the lower border of the pectoralis muscle distally along the coracobrachialis and biceps muscles. A blunt finger dissection under the junction of the inferior edge of the pectoralis muscle and deltoid muscle is performed, and an Army-Navy retractor is used to retract the pectoralis-deltoid complex superiorly and laterally. Therein should lay the LHB after tenotomy (Video 1, minute 1:15). The longitudinal, white tendon of the biceps tendon is identified and pulled out of the incision by use of a right-angle clamp. The myotendinous junction is identified. The long head tendon is whipstitched with No. 2 FiberWire (Arthrex) beginning at the junction and proceeding 1.5 cm proximally (Video 1, minute 1:31). The excess tendon is cut, and the tendon diameter is sized (this case measured slightly <5 mm in diameter). The free suture ends are passed through the cortical button (Fig 1). Lastly, the free suture ends are clamped and safely put aside as attention is turned to the humeral drilling.
Fig 1.
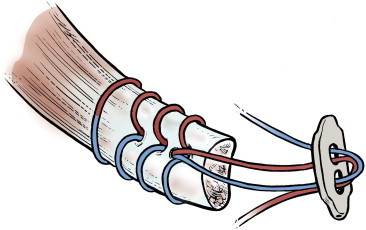
The cortical button is loaded after whipstitching of the tendon by passing a free suture end through the ipsilateral button hole away from the tendon and back through the contralateral hole toward the tendon. This is repeated with the other free suture end.
Adequate visualization of the distal part of the biceps groove is paramount. To accomplish this, the deltoid-pectoralis complex is retracted superolaterally with a Hohmann retractor while the short head of the biceps brachii and coracobrachialis muscles are retracted medially with an Army-Navy retractor (Fig 2A). One should avoid vigorous medial retraction to protect the musculocutaneous nerve. The site for drilling is identified at the distal-most aspect of the biceps groove. First, a 3.2-mm guidewire is drilled through the anterior cortex as far as the posterior cortex. This is followed by a cannulated drill slightly larger in diameter than the tendon (in our case, a 5-mm drill for a 4.5-mm tendon). Care is taken to only drill up to the posterior cortex without engaging the cortex or plunging through. The hole should be lined up at the base of the biceps groove (Fig 2B) and cleared of soft tissue. Finally, the second (posterior) cortex is drilled through with the 3.2-mm drill to allow for the passage of the cortical button.
Fig 2.
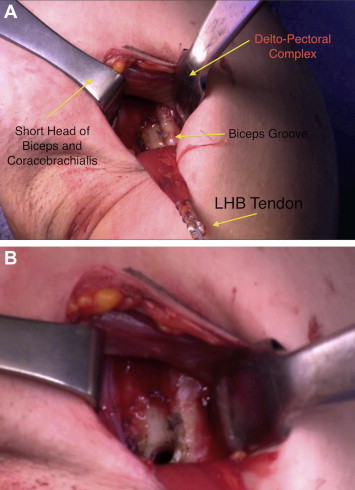
(A) The exposure of the biceps groove involves retraction of the deltoid and pectoralis muscle superolaterally with a Hohmann retractor and retraction of the short head of the biceps brachii and coracobrachialis muscle medially with an Army-Navy retractor. Vigorous retraction should be avoided with this retractor medially to protect the musculocutaneous nerve. (B) A unicortical drill hole is drilled at the distal biceps groove measuring slightly larger than the LHB tendon diameter.
The button is loaded onto the BicepsButton deployment device. Once the button clears the second cortex, the deployment instrument can be removed while the button deploys itself, locking into place on the posterior cortex (Fig 3). Pulling on the sutures shuttles the LHB tendon into the humerus. The sutures are tensioned until the tendon is in contact with the posterior cortex. Finally, we advocate using a free needle to pass one suture through the tendon and tie down to the second suture to reinforce the fixation (Video 1, minute 3:12). The wound is copiously irrigated and closed in a routine manner. The key steps of this technique are outlined in Table 1.
Fig 3.
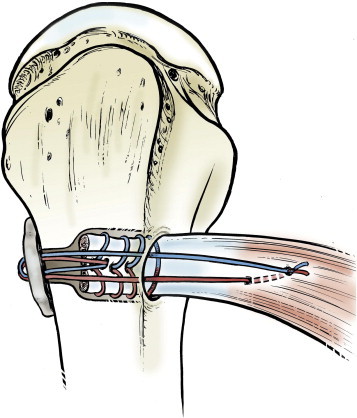
Final fixation with the cortical button on the posterior humerus and the whipstitched LHB tendon shuttled through the humerus and then tied down with suture.
Table 1.
Key Points of LHB Tenodesis With Cortical Button Technique
| The mini-incision should be centered over the inferior border of the pectoralis major tendon. |
| The LHB should be whipstitched beginning at the myotendinous junction and proceeding 15 mm proximally. |
| The unicortical humeral drill hole of the anterior cortex should be slightly larger than the tendon size. |
| The tension-slide technique is used to shuttle the tendon into the humerus. |
| The construct is reinforced by passing a single suture through the tendon adjacent to the anterior humerus drill hole. |
Discussion
The LHB tendon has an important, though imperfectly understood, role in the shoulder. It contributes to dynamic stabilization of the glenohumeral joint and adds supination and elbow flexion strength and endurance. Originally described as a vestigial structure, the biceps tendon has come to be known as a major “pain generator” of the shoulder.1 A range of open and arthroscopic procedures for biceps tenodesis have been described to address function, pain, and cosmesis. Our technique applies an established distal biceps cortical button to LHB tenodesis.
Distal biceps tenodesis with the BicepsButton has been adapted for LHB tenodesis. It lends itself to this application, with the humerus at the distal biceps groove replacing the radial tuberosity. Its anatomic placement at the distal-most aspect of the biceps groove is consistent with current literature.6 Unlike the use of the BicepsButton in the elbow, an additional interference screw is not required to achieve adequate fixation of the tendon. Rather, we advocate an additional suture passed through the tendon of the LHB once it is shuttled through the humerus. This provides additional fixation strength to withstand physiologic loads. This note describes a new technique for subpectoral proximal biceps tenodesis with a bone-conserving, smaller-diameter humerus drill hole; less biceps tendon trauma; and the potential to be performed in an arthroscopically assisted manner. Drill-hole size has been associated with risk of fracture. A small increase in diameter results in a square increase in surface area (π × r2). This technique minimizes the drill hole size by using a slightly larger drill-hole than the LHB tendon size, thereby potentially reducing the risk of fracture.7 Other techniques, such as interference screws, use compression to achieve fixation. Conversely, the cortical button technique uses a “sling and tensioning” that may be less traumatic to the tendon fibers at the time of fixation, thus decreasing the risk of failure. Though rare, there are reports of interference screws failing at the tendon-screw interface.8 We believe that this technique restores biceps contour and function adequately with a low risk of complications. LHB tenodesis with a cortical button is a viable treatment option. However, long-term clinical outcomes studies are still needed.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Step-by-step breakdown of LHB tenodesis with cortical button. (1) Tenotomy of the LHB tendon is completed arthroscopically. (2) A subpectoral approach (mini-incision centered over the inferior border of the pectoralis major tendon) is made. (3) The LHB tendon is pulled out of the incision and whipstitched from the myotendinous junction proximally (15 mm). (4) Excess tendon is cut, the tendon diameter is sized, and the cortical button is dressed. (5) The distal aspect of the biceps groove is exposed (avoiding vigorous medial retraction). (6) At the base of the biceps groove, the anterior cortex is drilled up to the posterior cortex (drill diameter slightly larger than tendon); the posterior cortex is drilled with the guidewire only. (7) The button is deployed posteriorly to the posterior cortex; pulling on the sutures shuttles the LHB tendon into the humerus. (8) Using a suture with a free needle through the tendon to reinforce fixation is advocated.
References
- 1.Mazzocca A.D., Bicos J., Santangelo S., Romeo A.A., Arciero R.A. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21:1296–1306. doi: 10.1016/j.arthro.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 2.Gartsman G., Hammerman S. Arthroscopic biceps tenodesis: Operative technique. Arthroscopy. 2000;16:550–552. doi: 10.1053/jars.2000.4386. [DOI] [PubMed] [Google Scholar]
- 3.Froimson A.I., Oh I. Keyhole tenodesis of biceps origin at the shoulder. Clin Orthop Relat Res. 1975;112:245–249. [PubMed] [Google Scholar]
- 4.Mazzocca A.D., Rios C.G., Romeo A.A., Arciero R.A. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21:896. doi: 10.1016/j.arthro.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 5.Boileau P., Krishnan S.G., Coste J.S., Walch G. Arthroscopic biceps tenodesis: A new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18:1002–1012. doi: 10.1053/jars.2002.36488. [DOI] [PubMed] [Google Scholar]
- 6.Busconi B.B., DeAngelis N., Guerrero P.E. The proximal biceps tendon: Tricks and pearls. Sports Med Arthrosc Rev. 2008;16:187–194. doi: 10.1097/JSA.0b013e318183c134. [DOI] [PubMed] [Google Scholar]
- 7.Edgerton B.C., An K.N., Morrey B.F. Torsional strength reduction due to cortical defects in bone. J Orthop Res. 1990;8:851–855. doi: 10.1002/jor.1100080610. [DOI] [PubMed] [Google Scholar]
- 8.Koch B.S., Burks R.T. Failure of biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28:735–740. doi: 10.1016/j.arthro.2012.02.019. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Step-by-step breakdown of LHB tenodesis with cortical button. (1) Tenotomy of the LHB tendon is completed arthroscopically. (2) A subpectoral approach (mini-incision centered over the inferior border of the pectoralis major tendon) is made. (3) The LHB tendon is pulled out of the incision and whipstitched from the myotendinous junction proximally (15 mm). (4) Excess tendon is cut, the tendon diameter is sized, and the cortical button is dressed. (5) The distal aspect of the biceps groove is exposed (avoiding vigorous medial retraction). (6) At the base of the biceps groove, the anterior cortex is drilled up to the posterior cortex (drill diameter slightly larger than tendon); the posterior cortex is drilled with the guidewire only. (7) The button is deployed posteriorly to the posterior cortex; pulling on the sutures shuttles the LHB tendon into the humerus. (8) Using a suture with a free needle through the tendon to reinforce fixation is advocated.