

Abstract
Exertional compartment syndrome of the leg is a condition that can cause chronic debilitating pain in active persons during a variety of aerobic activities. Nonoperative treatments using stretching protocols and activity modifications are often unsuccessful, and thus several operative strategies have been used to treat this condition. A novel technique for endoscopically assisted fasciotomy for chronic exertional compartment syndrome is described. By use of a small laterally based incision and an arthroscope, polydioxanone sutures are passed percutaneously along the anterior and lateral compartments with the Spectrum suture-shuttling device (ConMed Linvatec, Largo, FL). These sutures are used to retract the skin and subcutaneous tissues over the respective compartments. This method allows excellent visualization of the intercompartmental septum, the superficial peroneal nerve, and all perforating vessels. The anterior and lateral compartments can be safely and completely released with this minimally invasive approach. The patient is allowed to return to full activity at 6 weeks postoperatively, because of the decreased soft-tissue disruption.
Exertional compartment syndrome is an activity-related condition that typically affects young active persons. Clinical signs include pain in the lower leg musculature that worsens with activity. The pathophysiology is somewhat unclear, but a temporary relative ischemia in the lower leg appears to be involved. This induces swelling and results in increased intracompartmental pressure.1
Treatment for this condition has undergone an evolution as newer techniques have been developed. Nonoperative management including stretching and activity modification is the initial treatment of choice. Though still an appropriate first step, the long-term results of this treatment have been unimpressive.2 Surgical management has typically used fasciotomies.3 Techniques have ranged from open to endoscopic.4 A literature review of recent endoscopic techniques is shown in Table 1.4-8 The endoscopic technique allows for smaller incisions, thus reducing both surgical morbidity and healing times. This article describes a novel technique for endoscopic compartment release in the lower leg that provides for improved soft-tissue retraction and visualization.
Table 1.
Literature Review of In Vivo Endoscopic Compartment Release Techniques
| Year Published | No. of Patients | Compartment | Incision | Instrument for Fasciotomy | Complication | |
|---|---|---|---|---|---|---|
| Ota et al.5 | 1999 | 1 | Anterior | 3 | Retrograde knife | None |
| Kitajima et al.6 | 2003 | 1 | Anterior | 1 | Retrograde knife | None |
| Stein and Sennett4 | 2005 | 4 | Anterior, lateral | 1 | Metzenbaum scissors | None |
| Lohrer and Nauck7 | 2007 | 17 | Anterior, lateral, deep posterior | 1 (per compartment) | Metzenbaum scissors (anterior/lateral), custom scissors (deep posterior) | Revision open surgery for hemorrhage in 2 deep posterior compartment releases |
| Wittstein et al.8 | 2010 | 9 | Anterior, lateral, superficial and deep posterior | 1 for anterior/lateral compartment, 1 for superficial/deep posterior compartment | Endoscopic scissors | Hematoma development in 2 patients |
Technique
The bilateral lower extremities are prepared and draped in the standard sterile fashion. The initial leg is exsanguinated, and the tourniquet is inflated to 250 mm Hg. The initial incision is made in such a fashion as to center it on the superficial peroneal nerve. An incision (4 to 6 cm in length) is made at a point 12 cm proximal to the tip of the lateral malleolus and 5 cm lateral to the crest of the tibia.4 This is carried down through subcutaneous tissues, and the superficial peroneal nerve is identified. It is critical to protect this nerve throughout the case.
A switching stick and long thoracic scissors are used to bluntly develop a space between the subcutaneous tissue and the fascia of the anterior and lateral compartments. A 30° dry arthroscope is inserted through the incision and advanced proximally along the anterior compartment fascia. The light from the arthroscope illuminates the skin and allows one to localize its tip. While the surgeon is visualizing with the arthroscope, a Spectrum suture-passing device (ConMed Linvatec, Largo, FL) loaded with a No. 1 polydioxanone suture (PDS) is percutaneously inserted at the proximal aspect of the anterior compartment (Fig 1). By triangulating, one uses the Spectrum to aim for the tip of the arthroscope (Fig 2). Once this is performed, the arthroscope can be withdrawn, with the Spectrum in tow. The suture can then be advanced with the Spectrum wheel and retrieved through the incision with an arthroscopic grasper. These steps are then repeated for the lateral compartment, leaving 2 sutures percutaneously entering the skin proximally and exiting distally through the incision. A snap is applied to each end of the suture, and tension can be applied to retract the subcutaneous tissue from the underlying compartmental fascia (Fig 3).
Fig 1.

Clinical photograph of the right leg of a patient in the supine position. A 30° arthroscope is placed through a small distal incision. The Spectrum suture passer is then placed through a proximal incision to introduce a No. 1 PDS. The technique used for the anterior compartment is depicted.
Fig 2.
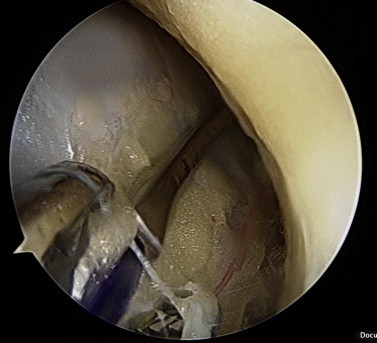
Arthroscopic photograph showing the Spectrum suture-passing device introducing a No. 1 PDS under direct visualization through the arthroscope. The spectrum is then visualized along its course to the distal incision, where an arthroscopic grasper is used to retrieve the suture.
Fig 3.

The No. 1 PDS is used for retraction of the skin. This ensures excellent visualization of the fascia and the superficial peroneal nerve with the arthroscope. A similar technique is used for the lateral compartment using the proximal incision that is marked in this clinical photograph.
With the superficial peroneal nerve protected, small incisions are made in the anterior and lateral compartment fascia. Long scissors are inserted under the respective fascia to develop a plane between it and the underlying muscle. Using the arthroscope for direct visualization, the surgeon then splits the anterior compartment fascia proximally using scissors with the tips barely spread. These steps are repeated to release the proximal portion of the lateral compartment. This technique can be repeated distally, but often an arthroscopic grasper is long enough to provide adequate retraction of the subcutaneous tissues over the distal anterior and lateral compartments. The key points of the technique are listed in Table 2.
Table 2.
Key Points of Surgical Technique for Endoscopic Compartment Release
| Incision made 12 cm proximal to lateral malleolus and 5 cm lateral to tibial crest |
| Switching stick used to develop plane |
| Percutaneous placement of Spectrum suture passer under arthroscopic visualization |
| No. 1 PDS used for retraction of skin overlying anterior and lateral compartments |
| Compartment release using scissors under arthroscopic visualization |
Exertional compartment syndrome commonly involves both lower extremities. If so, the contralateral leg anterior and lateral compartments are released in the same fashion. The tourniquet is deflated after both compartments in the respective leg are released, and care is taken to assess for bleeding. The wounds are irrigated, and the skin is closed with No. 2-0 Vicryl (Ethicon, Somerville, NJ) and a running subcutaneous No. 2-0 Prolene suture (Ethicon). Steri-Strips (3M, St Paul, MN) are placed over the Spectrum insertion sites. Cotton is wrapped around the calf, and an ACE wrap (3M) is applied from the foot to the distal thigh to provide compression and reduce the risk of hematoma formation. Dressings are removed on the second postoperative day. Elevation is encouraged to prevent swelling. In bilateral release situations, crutches are used for 2 weeks in an effort to restrict activity and allow wound healing. At 2 weeks, the sutures are removed and the patient is weaned off crutches. Patients are cautioned to limit their activity until their wounds are completely healed. They can gradually return to full activity in 6 weeks. Our technique is demonstrated in Video 1.
Discussion
Acute compartment syndrome can be debilitating to patients, because it often has neurologic, vascular, and muscular effects.9 Chronic exertional compartment syndrome differs in presentation and time course from that seen in trauma, but the eventual sequelae can be the same. Nonoperative management using stretching and activity modification has been found to have poor results.10
Surgical techniques for acute compartment syndrome have been used for many years. The original open 2-incision technique has been performed since World War II.11 Chronic exertional compartment syndrome was initially treated in such a fashion, but management has evolved toward less invasive techniques. In 1956 Mavor12 published the first description of surgical treatment for exertion compartment syndrome. Due and Nordstrand13 in 1987 described a minimally invasive subcutaneous fasciotomy using several small incisions to blindly divide the fascia. In recent years, multiple endoscopic techniques have been described.5,8,11,14
Overall, surgical outcomes have been favorable with subcutaneous and endoscopic techniques. Fronek et al.10 noted good results in 92% of patients in a small series involving a subcutaneous technique. A larger study of 78 female patients noted satisfactory results in 76%.15 Complications include postoperative hematoma, wound infection and healing issues, nerve injury, and recurrence. Poor outcomes can typically be traced to one of several causes, including an inadequate release, neurovascular injury, muscular injury, incomplete rehabilitation, or incorrect preoperative diagnosis.4 The endoscopic technique seeks to improve on more conventional techniques to limit the risk of inadequate release, neurovascular injury, soft-tissue disruption, and wound complications.
Although we believe that the described technique improves visualization substantially, it is not without limitations. The risk still exists for an inadequate release particularly if the starting incisions are inappropriately placed. This could lead to recurrence. As with any procedure, there is risk to adjacent neurovascular structures if they are not identified and protected. In addition, Wittstein et al.8 described 2 cases of hematoma formation in their series, which led them to begin to incorporate Hemovac drain use into their technique.
Many previously described endoscopic techniques require larger incisions or special equipment (i.e., long or inflatable retractors) to adequately and safely visualize the anterior and lateral compartment fascia.4,8,16 To do so, one is challenged to fit an arthroscope, scissors, and a retractor into a small incision. Our method builds on the previously described techniques but uses a suture-passing device that most arthroscopic surgeons have at their disposal. In addition, the blue Prolene suture provides an internal visual guide and an external aiming point and allows more space for the scissors and arthroscope during the compartment release. This retraction allows for optimal visualization of the anterior and lateral compartments, as well as the superficial peroneal nerve, thus allowing for a safe and effective compartment release. Soft-tissue damage is minimized, and the patient is allowed to resume full activity at 6 weeks.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Our technique for endoscopic compartment release method is outlined.
References
- 1.Reneman R.S. The anterior and the lateral compartmental syndrome of the leg due to intensive use of muscles. Clin Orthop Relat Res. 1975;113:69–80. doi: 10.1097/00003086-197511000-00011. [DOI] [PubMed] [Google Scholar]
- 2.Detmer D.E., Sharpe K., Sufit R.L. Chronic compartment syndrome: Diagnosis, management, and outcomes. Am J Sports Med. 1985;13:162–170. doi: 10.1177/036354658501300304. [DOI] [PubMed] [Google Scholar]
- 3.Mubarak S.J., Owen C.A. Double-incision fasciotomy of the leg for decompression in compartment syndromes. J Bone Joint Surg Am. 1977;59:184–187. [PubMed] [Google Scholar]
- 4.Stein D.A., Sennett B.J. One-portal endoscopically assisted fasciotomy for exertional compartment syndrome. Arthroscopy. 2005;21:108–112. doi: 10.1016/j.arthro.2004.09.023. [DOI] [PubMed] [Google Scholar]
- 5.Ota Y., Senda M., Hashizume H., Inoue M. Chronic compartment syndrome of the lower leg: A new diagnostic method using near-infrared spectroscopy and a new technique of endoscopic fasciotomy. Arthroscopy. 1999;15:439–443. doi: 10.1016/s0749-8063(99)70063-0. [DOI] [PubMed] [Google Scholar]
- 6.Kitajima I., Tachibana S., Hirota Y., Nakamichi K., Miura K. One-portal technique of endoscopic fasciotomy: Chronic compartment syndrome of the lower leg. Arthroscopy. 2003;17:E33. doi: 10.1053/jars.2001.25261. [DOI] [PubMed] [Google Scholar]
- 7.Lohrer H., Nauck T. Endoscopically assisted release for exertional compartment syndromes of the lower leg. Arch Orthop Trauma Surg. 2007;127:827–834. doi: 10.1007/s00402-006-0269-4. [DOI] [PubMed] [Google Scholar]
- 8.Wittstein J., Moorman C.T., III, Levin L.S. Endoscopic compartment release for chronic exertional compartment syndrome: Surgical technique and results. Am J Sports Med. 2010;38:1661–1666. doi: 10.1177/0363546510363415. [DOI] [PubMed] [Google Scholar]
- 9.Rorabeck C.H., Clarke K.M. The pathophysiology of the anterior tibial compartment syndrome: An experimental investigation. J Trauma. 1978;18:299–304. doi: 10.1097/00005373-197805000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Fronek J., Mubarak S.J., Hargens A.R. Management of chronic exertional anterior compartment syndrome of the lower extremity. Clin Orthop Relat Res. 1987;220:217–227. [PubMed] [Google Scholar]
- 11.DeBakey M.E., Simeone F.A. Battle injuries of the arteries in World War II: An analysis of 2,471 cases. Ann Surg. 1946;123:534–579. [PubMed] [Google Scholar]
- 12.Mavor G.E. The anterior tibial syndrome. J Bone Joint Surg Br. 1956;38:513–517. doi: 10.1302/0301-620X.38B2.513. [DOI] [PubMed] [Google Scholar]
- 13.Due J., Jr., Nordstrand K. A simple technique for subcutaneous fasciotomy. Acta Chir Scand. 1987;153:521–522. [PubMed] [Google Scholar]
- 14.Leversedge F.J., Casey P.J., Seiler J.G., Xerogeanes J.W. Endoscopically assisted fasciotomy: Description of technique and in vitro assessment of lower-leg compartment decompression. Am J Sports Med. 2002;30:272–278. doi: 10.1177/03635465020300022101. [DOI] [PubMed] [Google Scholar]
- 15.Micheli L.J., Solomon R., Solomon J., Plasschaert V., Mitchell R. Surgical treatment for chronic lower-leg compartment syndrome in young female athletes. Am J Sports Med. 1999;27:197–201. doi: 10.1177/03635465990270021401. [DOI] [PubMed] [Google Scholar]
- 16.Sebik A., Dogan A. A technique for arthroscopic fasciotomy for the chronic exertional tibialis anterior compartment syndrome. Knee Surg Sports Traumatol Arthrosc. 2008;16:531–534. doi: 10.1007/s00167-007-0454-1. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Our technique for endoscopic compartment release method is outlined.