

Abstract
Human movement such as sit-to-stand (STS) is one of the most fundamental and essential movement among daily living activities. Elderly who are unable to stand are severely limited in daily activities and rely on others for their care. In the coming next two decades about 20% of US population will be above the age of 65 years, and considering ever-increasing elderly population and health care expenses, the rehabilitation of functionally limited elderly is becoming a topic of greater concern. Clinically STS movement is looked upon with great interest, such as its analysis is meaningful in order to evaluate motor control and stability in elderly patients with functional limitations and may be more helpful than traditional medical evaluations in diagnosing and treating mobility problems in elderly. A few previous research studies describe controlled STS movements with constrains in laboratory environments and have established STS standardized events. A comparative study is presented in this work using and inertial measurement unit (IMU) and existing laboratory based sit-to-stand phases and events. The aims of this study are (1) to define phases and identify events of STS movement based on those previously described, using wireless IMU (2) to test the consistency of these events and phases in total of seven young healthy subjects (ages 25–35 years). We found significant differences in peak flexion angular velocities (p<0.001), peak extension angular velocities (p<0.01) and accelerations at seat-off (p<0.01) between participants when using chair arm rest versus knee as support during rising. Also, we have found significant differences in time events for pre seat off flexion decelerations and post seat off extension angular accelerations with the two different rising supports. Thus these distinct and consistent phases of STS movement using IMU can help identify individuals at fall risk in non-laboratory environments.
Keywords: Sit-to-Stand using arm-rest (STSA), Sit-to-stand using knee support (STSK), Inertial measurement unit (IMU)
INTRODUCTION
Sit-to-Stand (STS) is one of the most fundamental and essential movement among daily living activities and its analysis is meaningful in order to evaluate motor control and stability in elderly patients with functional limitations [1, 2]. Nearly 8% of non-institutionalized persons aged 65 and above have difficulty in getting in and out of chair [3] and about 3% need assistance in these transferring tasks. Performance of transition from sitting to standing requires ability to maintain balance along with production of enough muscle force to raise the body’s center of mass (COM) from a seated to a standing position [4, 5]. With aging, there is deterioration of the muscle strength, joint range of motion[3], balance performance and ability to rise from a chair and these accentuate the risk of falling [6–9]. Several studies have determined STS performance and its correlation with falls in stroke patients [10–12] and few studies also suggest the risk of falling increases in those elderly who have difficulty in rising from chair [3, 13, 14]. In 2009, about 2.2 million nonfatal fall injuries were reported among older adults and were treated in emergency departments and more than 581,000 of these patients were hospitalized[15]. Also, in the year 2007, over 18,000 older adults died from fall injuries [15]. The association between falls and chair rise performance difficulty is not arguable as both appear to indicate deficits in postural control ability.
Although human gait has been extensively studied and gait cycle has been very well established, only a few research studies are there which describe controlled STS movements with constrains in laboratory environments and have established STS standardized events [16–18]. It is quite evident from previous studies that it is critical to control the initial position of subjects who are rising from a chair before comparisons can be made within or between subjects[19–21]. Several determinants of sit-to-stand such as chair related determinants (height of chair, armrests), subject related determinants (foot position) have been defined to influence the performance of STS movement[22]. However, failing to account for these determinants may lead to erroneous measurements of changes in STS performance. But, by controlling the variability of STS movement, some important components of variability may be lost. Thus lack of single method for delineating STS events and differences in experimental methods in earlier STS studies has made comparisons difficult or impossible.
Kralj et al. [18] presented a paper aimed to provide normative data in order to analyze STS and to describe and define phases, events, and their specific time of occurrence. But all these definitions are completely based on ground reaction forces (GRF) from the force plate. This effectively limits the application. Although the events defined are sequential but some kinematic events do not appropriately coincide with those defined by GRF. Kerr et al. [17] have defined events using tethered customized vector stereograph at the back of participants which hinders normal STS movement reduce applicability. They used an accelerometer for sagittal and vertical acceleration, but no efforts have been done in denoising the data and consequently the peak detection for event detection must be viewed with caution. Whole body movements during STS rising were studied by Schenkman et al. [5] and the authors described four phases of STS activity as flexion momentum, momentum transfer, extension and stabilization but this work is prone to human errors due to involved intense manual expertise and experience in event identification. The use of seat switches/or force plate under chair by authors could have reduced human source of error in timing events. The study is also based on motion capture data, thus is limited by application perspective to laboratory environment. This study also lacks generalizability as the studied population is only females. Recently, easily identifiable STS events and standardization method was presented by Etnyre et al. [16] to assess and compare patient functionality and allow comparisons among STS research with different arm-use conditions. This standardization method is highly robust but these identified kinetic events and associated phases do not demonstrate any physiological measure of motor functioning in STS movement. Thus almost all previous STS event standardization using force plate and seat switch [16], tethered accelerometer and vector stereograph [17, 23, 24], force plates and optoelectronic cameras [5] are limited in application. There remains a clinical need for a non-laboratory based well standardized experimental and analysis set-up in which subjects are allowed to rise under uncontrolled conditions which is highly suitable for elderly patients with motor disabilities for fall risk evaluation.
Recently, body fixed sensors are used to measure aspects of human performance under real life conditions as they can be carried on the body without interfering with normal behavior [25]. Although stand still body sway measures using accelerometers is still being discussed for validity and sensitivity of sway parameters to describe balance control [26, 27], accuracy and sensitivity of accelerometers to assess balance control during sit-to-stand movement has been well validated [17, 24, 28, 29].
The aims of this study are (1) to define phases and identify events of STS movement based on those previously described for STS using wireless IMU (2) to test the consistency of these events and phases in group of healthy subjects. The experimental hypothesis is that distinct and consistent phases of STS movement can help detect variability in postural transitions and furthermore identify fall prone individuals. This paper further addresses the potential relevance of wireless IMU in measuring the aspects of human STS performance using a well-established denoising technique for non-stationary signals. Our work demonstrate that obtaining measures of motor functioning by IMU can provide a significant contribution to estimating fall risk and the evaluation of fall intervention effects.
METHODS
Participants
Data was collected by seven young participants (5 males, 2 females) of age (29±4 years) and STS task using arm-rest support and knee support were performed by them in Locomotion Research Laboratory, Virginia Tech. All participants were healthy, and did not require the use of any assistive devices. They were able to rise from chair without assistance and were free of orthopedic injury. All participants in the study provided written consent prior to participation.
Instrumentation
The inertial measurement unit (IMU) used is TEMPO (Technology-Enabled Medical Precision Observation) 3.1 which is manufactured in collaborative research with inertia team in UVA [30]. It consist of MMA7261QT tri-axial accelerometers and IDG-300 (x and y plane gyroscope) and ADXRS300 as z-plane uniaxial gyroscope. The data acquisition was carried using a bluetooth adapter and Laptop through a custom built LabView VI [30]. Data are acquired with sampling frequency of 128Hz. This frequency is largely sufficient for human movement analysis in daily activities which occurs in bandwith [0.8–5Hz][31]. The collected data is stored in custom xml file using the custom built LabView VI. Two instrumented force platform (AMTI BP400600 SN 6780/6782) was used to measure ground reaction forces (GRF) under subject’s feet and the chair during STS. The sampling frequency was 128Hz for forceplate and camera system.
Procedure
TEMPO node is an IMU with three accelerometers and three gyroscopes in combination. Participants wore two TEMPO nodes (one on trunk at sternum level, one on right wrist) but only the nodes on trunk is used here for sit-to-stand analysis whereas wrist nodes were used to synchronize the IMU data with force plate and camera system in this experiment. Participants were asked to tap quickly near the right wrist before performing STS. This was conducted in order to synchronize the TEMPO signals with the Ulnar stylus infra-red marker which were temporally synchronized with Force plates by a custom built LabView VI. The participants sat comfortably on chair with backrest and arm-rest. The subjects had to keep their thighs and feet parallel and were instructed to use arm-rest/knee for support while performing STS task. The chair was kept on one force plate and the feet of participants rested on another. The spacing between feet was maintained at 15 cm. Chair popliteal height was 45 cm and knee angle was maintained from 85°–90° using Styrofoam. Participants were instructed to sit such that thigh did not rest on seat and only buttocks rested on it. Participants were asked to wait for an auditory signal before initiating movement. The data was recorded for 12 seconds in total. The participants were given the auditory signal to stand after at least 3 seconds of data collection in order to ensure sitting, postural transition and stabilized standing is collected in all trials. Each participant performed three STS task using arm rest (STSA) and three STS using knee support (STSK) for rising. The co-investigator demonstrated the STS task prior to data collection.
Data Processing Technique
The data was post processed using custom software written in Matlab (the Mathworks, Inc.). Empirical Mode Decomposition (EMD) [32, 33] is an adaptive time-frequency data analysis method and can adaptively divide the IMU signals into different intrinsic mode function (IMF) components according to different time scale, and noise which mainly concentrates in the high-frequency component. IMU noisy signals are decomposed adaptively into oscillatory components called intrinsic mode functions (IMFs) by means of a process called sifting. The sifting process has two effects: (a) to eliminate riding waves and (b) to smooth uneven amplitudes. The traditional EMD involves the decomposition of a given signal x(t) into a series of IMFs, through the sifting process, each with distinct time scale [33]. Unlike wavelet decompositions the major advantage of the EMD is that the basis functions are derived from the signal x(t) itself. Each IMF replaces then the detail signals of at a certain scale or frequency band [34]. The EMD picks out the highest frequency of oscillation that remains in the signal. An IMF has to follow two requirements: (R1) the number of extrema and the number of zero crossings are either equal or differ at most by one; (R2) at any point, the mean value of the envelope defined by the local maxima and the envelope defined by the local minima is zero. The sifting is repeated several times in order to get to be a true IMF that fulfils the requirements (R1) and (R2) mentioned above. The result of the sifting procedure is that x(t) is decomposed into IMFs, IMj(t)=j=1,2,….N and residual rN(t).
| (1) |
Let Cj(t) be a deterministic IMF with the finite length L and IMj the corrupted IMF with additive noise bj(t) with variance σj2(t): Let
| (2) |
We have used EEMD-Golay denoising on signals from trunk. The number of ensembles chosen is 100 with ratio of standard deviation of the added noise to that of signal as 0.2. First half of the IMF’s containing high frequency noise are filtered using savitzky-golay filter (polynomial order 3 and number of frames as 41) and then reconstructed to get the denoised signals. The signals from force plate were filtered using dual pass Butterworth filter with cut-off frequency of 6Hz.
RESULTS
STS standardization method proposed by Etnyre and Thomas [16] is used for comparison in our laboratory and results are compared with those of wireless IMU. The seat-off event is defined as the instant where the rate of change in vertical force is maximum for the force plate below chair. The six events identified are 1) Initiation, 2) Counter, 3) Seat-Off, 4) Peak Vertical Force, 5) Rebound, 6) Steady standing and are shown in figure 1.
Figure 1.
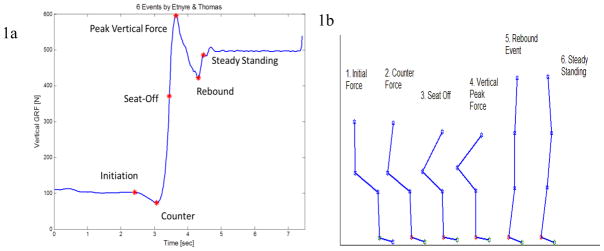
a) Identification of six events using vertical reaction force [16]. 1b) Five reflective markers on right heel, right toe, right lateral condyle, right trochanter and right acromio-clavicular positions to produce stick figure at the six events.
The normalized vertical forces at the six events were compared for the two conditions STSA and STSK. Paired t-test was used for finding effects of the two conditions (STSA versus STSK). Initiation force, force at seat off, and vertical peak force in STSK is found to be significantly different than that at STSA (Table 1). The mean vertical force at seat off in STSK condition is 82% of body weight (BW) while that in STSA condition it is nearly 60% of BW.
Table 1.
BW Normalized Forces in STSA and STSK conditions
| Events | STSA Forces | STSK Forces | p-value |
|---|---|---|---|
| Initiation* | 23.12±2.84 | 24.55±3.23 | 0.024 |
| Counter | 14.94±4.74 | 14.67±3.88 | 0.8307 |
| Seat-Off* | 59.89±7.70 | 82.52±6.67 | 0.022 |
| Vertical Peak* | 109.52±5.26 | 121.32±6.11 | 0.0084 |
| Rebound | 85.93±6.11 | 83.50±7.41 | 0.3928 |
| Steady Standing | 100 | 100 |
Gyroscope data from the axis perpendicular to sagittal plane has been used to determine trunk flexion and extension angular velocities. Accelerometer data from the axis perpendicular to the coronal plane determines anterio-posterior accelerations. In total five events are identified, a) STS Initiation, b) Peak flexion angular velocity, c) Peak extension angular velocity and d) STS termination from gyroscope data (figure 3b upper section) and seat off (event f) is determined by accelerometer data (figure 3b lower section). Also peak-to-peak (P2P) acceleration is determined as the absolute acceleration in STS, which is either from anterio-posterior (AP) acceleration initiation (event e) to seat off (event f)(figure 3b lower section) or from seat off (event f) to AP acceleration termination(event g). P2P flex./extn. Angular velocity is absolute value from (event b) to (event c). Peak flexion angular velocity (event b) is the maxima, and peak extension angular velocity (event c) is the minima as shown in figure 3b upper section.
Figure 3.
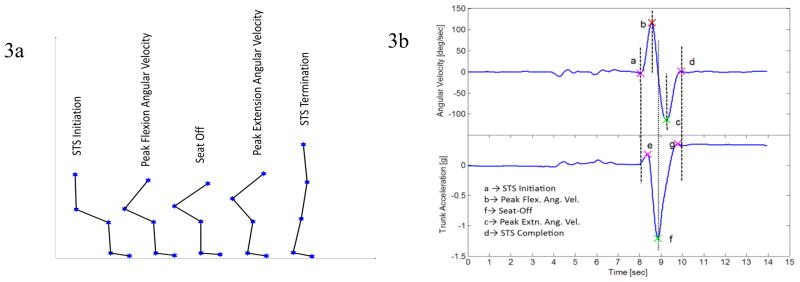
Figure 3a) STS Events identified by IMU data. 3b) upper section of the figure is trunk angular velocity with events (a. STS Initiation, b. Peak flexion angular velocity, c. Peak extension angular velocity, d. STS termination) and lower section of 3b is trunk anterio-posterior acceleration (where f is seat off event)
Initial flexion angular acceleration (slope from event a to event b), late extension angular acceleration (slope from event c to event d) can be computed by fitting the section in-between events of gyroscope signal by a straight line. Similarly, Pre-seat off flexion angular deceleration (slope from event b to the time at which seat off event f occurs), post-seat off extension angular acceleration (slope from event c to the time at which seat off event f had occurred) can be computed. Paired t-test was used for finding effects of the two STS conditions. Table 2 shows higher peak-peak anterio-posterior acceleration and higher flexion and extension angular velocities are generated in STSK condition. Table 3 shows us that as higher flexion momentum is generated, as a postural control strategy a quicker deceleration is followed afterwards, which is seen by the time spent from event b to event f.
Table 2.
STS Parameters defined using IMU
| IMU Parameters | STSA | STSK | p-value |
|---|---|---|---|
| P2P AP Acceleration * [g] | 0.90±0.175 | 1.32±0.122 | <0.0001 |
| P2P Flex./Ext. Ang. Vel. * [deg/sec] | 151.42±21.587 | 193.27±18.876 | 0.0012 |
| Peak Flex. Ang. Vel. * [deg/sec] | 70.44±13.567 | 106.37±13.741 | 0.0003 |
| Peak Ext. Ang. Vel. * [deg/sec] | 75.71±13.501 | 86.40±13.767 | 0.0091 |
| Init. Flex. Ang. Acc. * [deg/sec2] | 2.18±0.587 | 3.21±0.579 | 0.0155 |
| Late Ext. Ang. Acc. [deg/sec2] | 2.13±0.732 | 2.21±0.535 | 0.3254 |
| Pre_SeatOff Flex. Ang. Dece. * [deg/sec2] | 4.16±1.170 | 5.38±1.111 | 0.0098 |
| Post_SeatOff Extn. Ang. Acc. * [deg/sec2] | 3.07±1.110 | 3.78±1.295 | 0.0176 |
| Trunk Forward Jerk * [g2] | 0.02±0.008 | 0.04±0.009 | <0.0001 |
| Trunk Backward Jerk * [g2] | 0.01±0.004 | 0.02±0.007 | 0.0085 |
Table 3.
Time taken in-between events by STSA and STSK conditions
| Time of transition | STS Arm Rest [seconds] | STS Knee Support [seconds] | p-value |
|---|---|---|---|
| a–b | 0.65±0.142 | 0.66±0.132 | 0.4455 |
| b–f * | 0.39±0.046 | 0.30±0.036 | 0.001 |
| f–c * | 0.36±0.099 | 0.47±0.114 | 0.0024 |
| c–d | 0.82±0.196 | 0.84±0.108 | 0.3442 |
DISCUSSION
Body worn sensors can be used to determine STS kinematic parameters in non-laboratory environments. Young adults generate high flexion and extension momentums in STSK condition as compared to STSA. As high Pre-seat off flexion angular accelerations are created in STSK, just before seat off and followed by high deceleration of angular velocity after seat off, this is to counter the already self-generated momentum. Thus, rising up using knee support may present an extra challenge at seat off to elderly people. Also, elderly people may fail to generate or counter momentum at seat off due to weak muscles and may result in fall.
IMU signals are typically non-stationary signals, and difficult to be dealt with by the traditional filtering methods. We have denoised IMU signal based on the Ensemble Empirical mode decomposition (EEMD) framework with Savitzky-Golay filter. A similar denoising method combining EMD with the Savitzky-Golay has been used for denoising lidar signals, referred to as EMD-Golay algorithm has already been proposed by Zhang et. al [35]. One of the drawbacks of the EMD for denoising is the frequent appearance of mode mixing, which is defined as a single Intrinsic Mode Function (IMF) either consisting of signals of widely disparate scales, or a signal of a similar scale residing in different IMF components. Mode mixing is a consequence of signal intermittency and can cause aliasing in the time-frequency distribution, and also make the individual IMF devoid of physical meaning of the signal. To overcome this scale separation problem, Ensemble Empirical Mode Decomposition (EEMD) which is a noise assisted data analysis (NADA) method is used in signal denoising.
As the participants in this study are young and healthy, we may find a different strategy with older adults to lift their body from sitting position. But the use of wireless IMU systems and EEMD framework can help identify postural pathology in adults even in clinical environments. It is not feasible to compare actual values of parameter from force plate (kinetic data) and the kinematic data because different data are being measured by sensors with different sensing principles, bandwidths and geometric references and different variables are obtained by the two systems, each making a number of assumptions and approximations. Since the sensitivity of accelerometers is much larger a higher parameter value is expected. However, the analogous parameters found by either system in general follow the same behavior numerically and statistically.
CONCLUSIONS
A new wireless experimental set-up has been defined in this study to address the clinical need of performing STS and STW evaluation using a well-established method. This study provides a means of kinematic and temporal subcomponent analysis of rising from a chair in a sensitive and quantifiable manner. This data can be further applied to the development of appropriate screening, therapeutic, or clinical research techniques.
Figure 2.

Normalized forces at the six events for STSA and STSK
Acknowledgments
We are thankful to Dr. John Lach for providing IMU system.
References
- 1.Galli M, Cimolin V, Crivellini M, Campanini I. Quantitative analysis of sit to stand movement: experimental set-up definition and application to healthy and hemiplegic adults. Gait Posture. 2008 Jul;28:80–5. doi: 10.1016/j.gaitpost.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 2.Magnan A. Modification of the sit-to-stand task with the addition of gait initiation. Gait & Posture. 1996;4:232–241. [Google Scholar]
- 3.Alexander NB, Schultz AB, Warwick DN. Rising from a chair: effects of age and functional ability on performance biomechanics. J Gerontol. 1991 May;46:M91–8. doi: 10.1093/geronj/46.3.m91. [DOI] [PubMed] [Google Scholar]
- 4.Lord SR, Murray SM, Chapman K, Munro B, Tiedemann A. Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J Gerontol A Biol Sci Med Sci. 2002 Aug;57:M539–43. doi: 10.1093/gerona/57.8.m539. [DOI] [PubMed] [Google Scholar]
- 5.Schenkman M, Berger RA, Riley PO, Mann RW, Hodge WA. Whole-body movements during rising to standing from sitting. Phys Ther. 70:638–48. doi: 10.1093/ptj/70.10.638. discussion 648–51, Oct 1990. [DOI] [PubMed] [Google Scholar]
- 6.Goulart FR, Valls-Sole J. Patterned electromyographic activity in the sit-to-stand movement. Clin Neurophysiol. 1999 Sep;110:1634–40. doi: 10.1016/s1388-2457(99)00109-1. [DOI] [PubMed] [Google Scholar]
- 7.Gross MM, Stevenson PJ, Charette SL, Pyka G, Marcus R. Effect of muscle strength and movement speed on the biomechanics of rising from a chair in healthy elderly and young women. Gait Posture. 1998 Dec 1;8:175–185. doi: 10.1016/s0966-6362(98)00033-2. [DOI] [PubMed] [Google Scholar]
- 8.Dehail P, Bestaven E, Muller F, Mallet A, Robert B, Bourdel-Marchasson I, Petit J. Kinematic and electromyographic analysis of rising from a chair during a “Sit-to-Walk” task in elderly subjects: role of strength. Clin Biomech (Bristol, Avon) 2007 Dec;22:1096–103. doi: 10.1016/j.clinbiomech.2007.07.015. [DOI] [PubMed] [Google Scholar]
- 9.Lockhart TE, Smith JL, Woldstad JC. Effects of aging on the biomechanics of slips and falls. Hum Factors. 2005 Winter;47:708–29. doi: 10.1518/001872005775571014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cheng PT, Liaw MY, Wong MK, Tang FT, Lee MY, Lin PS. The sit-to-stand movement in stroke patients and its correlation with falling. Arch Phys Med Rehabil. 1998 Sep;79:1043–6. doi: 10.1016/s0003-9993(98)90168-x. [DOI] [PubMed] [Google Scholar]
- 11.Cheng PT, Wu SH, Liaw MY, Wong AM, Tang FT. Symmetrical body-weight distribution training in stroke patients and its effect on fall prevention. Arch Phys Med Rehabil. 2001 Dec;82:1650–4. doi: 10.1053/apmr.2001.26256. [DOI] [PubMed] [Google Scholar]
- 12.Chou SW, Wong AM, Leong CP, Hong WS, Tang FT, Lin TH. Postural control during sit-to stand and gait in stroke patients. Am J Phys Med Rehabil. 2003 Jan;82:42–7. doi: 10.1097/00002060-200301000-00007. [DOI] [PubMed] [Google Scholar]
- 13.Nevitt MC, Cummings SR, Kidd S, Black D. Risk factors for recurrent nonsyncopal falls. A prospective study. JAMA. 1989 May 12;261:2663–8. [PubMed] [Google Scholar]
- 14.Campbell AJ, Borrie MJ, Spears GF. Risk factors for falls in a community-based prospective study of people 70 years and older. J Gerontol. 1989 Jul;44:M112–7. doi: 10.1093/geronj/44.4.m112. [DOI] [PubMed] [Google Scholar]
- 15.CDC, Centers for Disease Control and Prevention. Center for Injury Prevention and Control. 2010. [Google Scholar]
- 16.Etnyre B, Thomas DQ. Event standardization of sit-to-stand movements. Phys Ther. 2007 Dec;87:1651–66. doi: 10.2522/ptj.20060378. [DOI] [PubMed] [Google Scholar]
- 17.Kerr KM, White JA, Barr DA, Mollan RAB. Standardization and definitions of the sit-stand-sit movement cycle. Gait & Posture. 1994;2:182–190. [Google Scholar]
- 18.Kralj A, Jaeger RJ, Munih M. Analysis of standing up and sitting down in humans: definitions and normative data presentation. J Biomech. 1990;23:1123–38. doi: 10.1016/0021-9290(90)90005-n. [DOI] [PubMed] [Google Scholar]
- 19.Rodosky MW, Andriacchi TP, Andersson GB. The influence of chair height on lower limb mechanics during rising. J Orthop Res. 1989;7:266–71. doi: 10.1002/jor.1100070215. [DOI] [PubMed] [Google Scholar]
- 20.Burdett RG, Habasevich R, Pisciotta J, Simon SR. Biomechanical comparison of rising from two types of chairs. Phys Ther. 1985 Aug;65:1177–83. doi: 10.1093/ptj/65.8.1177. [DOI] [PubMed] [Google Scholar]
- 21.Pai YC, Rogers MW. Control of body mass transfer as a function of speed of ascent in sit-to-stand. Med Sci Sports Exerc. 1990 Jun;22:378–84. [PubMed] [Google Scholar]
- 22.Janssen WG, Bussmann HB, Stam HJ. Determinants of the sit-to-stand movement: a review. Phys Ther. 2002 Sep;82:866–79. [PubMed] [Google Scholar]
- 23.Kerr KM, White JA, Barr DA, Mollan RA. Analysis of the sit-stand-sit movement cycle in normal subjects. Clin Biomech (Bristol, Avon) 1997 Jun;12:236–245. doi: 10.1016/s0268-0033(96)00077-0. [DOI] [PubMed] [Google Scholar]
- 24.Kerr KM, White JA, Barr DA, Mollan RAB. Analysis of the sit-stand-sit movement cycle: development of a measurement system. Gait & Posture. 1994;2:173–181. [Google Scholar]
- 25.Zijlstra W, Aminian K. Mobility assessment in older people: new possibilities and challenges. European Journal of Ageing. 2007;4:3–12. doi: 10.1007/s10433-007-0041-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mayagoitia RE, Lotters JC, Veltink PH, Hermens H. Standing balance evaluation using a triaxial accelerometer. Gait & Posture. 2002 Aug;16:55–59. doi: 10.1016/s0966-6362(01)00199-0. [DOI] [PubMed] [Google Scholar]
- 27.Moe-Nilssen R, Helbostad JL. Trunk accelerometry as a measure of balance control during quiet standing. Gait & Posture. 2002 Aug;16:60–68. doi: 10.1016/s0966-6362(01)00200-4. [DOI] [PubMed] [Google Scholar]
- 28.Janssen WGM, Kulcu DG, Horernans HLD, Stam HJ, Bussmann JBJ. Sensitivity of Accelerometry to Assess Balance Control During Sit-to-Stand Movement. Ieee Transactions on Neural Systems and Rehabilitation Engineering. 2008 Oct;16:479–484. doi: 10.1109/TNSRE.2008.2003386. [DOI] [PubMed] [Google Scholar]
- 29.Boonstra MC, van der Slikke RMA, Keijsers NLW, van Lummel RC, de Waal Malefijt MC, Verdonschot N. The accuracy of measuring the kinematics of rising from a chair with accelerometers and gyroscopes. Journal of Biomechanics. 2006;39:354–358. doi: 10.1016/j.jbiomech.2004.11.021. [DOI] [PubMed] [Google Scholar]
- 30.Barth AT, Hanson MA, Powell HC, Jr, Lach J. TEMPO 3.1: A Body Area Sensor Network Platform for Continuous Movement Assessment. 2009:71–76.
- 31.Bouten CV, Koekkoek KT, Verduin M, Kodde R, Janssen JD. A triaxial accelerometer and portable data processing unit for the assessment of daily physical activity. IEEE Trans Biomed Eng. 1997 Mar;44:136–47. doi: 10.1109/10.554760. [DOI] [PubMed] [Google Scholar]
- 32.Huang NE, Shen Z, Long SR. A new view of nonlinear water waves: The Hilbert spectrum. Annual Review of Fluid Mechanics. 1999;31:417–457. [Google Scholar]
- 33.Huang NE, Shen Z, Long SR, Wu MC, Shih HH, Zheng Q, Yen NC, Tung CC, Liu HH. The empirical mode decomposition and the Hilbert spectrum for nonlinear and non-stationary time series analysis. Proceedings of the Royal Society A: Mathematical, Physical and Engineering Sciences. 1998;454:903–995. [Google Scholar]
- 34.Flandrin P, Rilling G, Goncalves P. Empirical mode decomposition as a filter bank. Ieee Signal Processing Letters. 2004 Feb;11:112–114. [Google Scholar]
- 35.YiKun Z, XiaoChang M, DengXin H, YingAn C, LianSheng S. An EMD-based denoising method for lidar signal; Image and Signal Processing (CISP), 2010 3rd International Congress on; 2010. pp. 4016–4019. [Google Scholar]