

Abstract
The objective of the current study was to investigate the effects of aging on 3D lower extremity joint moments during successful reactive-recovery from unexpected slips. Unexpected slips were induced by having participants walk over a slippery floor surface. Successful reactive-recovery trials from nine young and nine elderly participants were identified and analyzed. Three-dimensional inverse dynamics were implemented to calculate reactive joint moments at the ankle, knee, and hip joints. Peak joint moment magnitude and the speed of peak joint moment generation were used to describe the balance recovery strategies from unexpected slips. Results indicated significantly higher peak joint moments in recovery than in normal walking for both the young and elderly. Meanwhile, during reactive-recovery, the elderly were found to utilize both frontal and sagittal joint moments while the younger adults relied primarily on sagittal joint moment. It was concluded that the ankle and knee joints were critical in controlling sagittal plane motion disturbance, while the hip joint was mainly responsible for stabilizing upper body balance in the frontal plane. This study confirmed age-related differences in joint moment generation during unexpected slips. Additionally, implementing 3D analysis is recommended in future slips and falls research.
Keywords: Slips and falls, Joint moment, Inverse dynamics, Locomotion, Aging Falls
1. Introduction
Falls are among the most serious problems facing the elderly and the second leading cause of accidental death for 45–75 year olds [1]. More than 25% of fall-related injuries in the elderly result from slip-induced falls and 66% of fall-related hip fractures occur on wet or slippery floor surfaces [2]. Additionally, falls and hip fractures among the elderly rank as one of the most serious public health problems in the U.S., with medical costs more than $19 billion each year [3].
While relevant gait kinematics and friction demand characteristics during ambulation are important in terms of description and categorization of slip-induced fall accidents [4–7], joint kinetic studies are necessary to provide further understanding of the causes of slip-induced fall accidents. Do et al. [8] suggested that explosive strength generation and the ability to attenuate fast, large-scale lower extremity motions are critical in determining whether or not a person can respond appropriately to balance perturbation. When we experience a perturbation from a slip, the body is set in motion and there is a change in momentum. This momentum is ultimately constrained by the generation of joint moment to reduce segmental motion and, hence, the linear momentum of the whole body. One hypothesis for the increased incidence of slip and falls among the elderly is that elderly adults may be unable to generate the necessary counterbalancing joint moments either in magnitude or in rate of development to control the body’s horizontal and vertical momentum during recovery from slips and falls. Evidence in support of this hypothesis comes from a number of investigations indicating an age-related decline in voluntary muscle strength and rate of muscle force production, and increased likelihood of slips and falls [9–11].
Recently, studies have assessed the role of aging in balance recovery from postural perturbations. For example, by mimicking tripping using a treadmill, the elderly were able to make successful adaptations after an initial failed recovery [12]. However, the ability to successfully avoid obstacles during walking did deteriorate with advancing age due to longer reaction time [13]. Additionally, insufficient knee extensor support [14] was found to contribute to failed recovery for the elderly. Nearly maximal joint moment was required for balance recovery of elderly females during protective stepping [15]. These findings emphasize the importance of gaining better understanding of the age-related joint moment responses during unexpected postural perturbations such as a slip.
The purpose of the current study was to investigate age-related joint moment characteristics during normal gait and successful reactive-recovery from unexpected slips to determine age-related balance recovery strategies associated with slip-induced falls. In order to objectively assess the characteristics of reactive responses of the lower extremities (the ankle, knee and hip joints), 3D joint moments were calculated during normal gait and during recovery phase of the slip-induced falls between the elderly and their younger counterparts. We hypothesized that the peak joint moment and the speed of peak moment generation would be significantly different between the age groups (young and the elderly) and walking conditions (normal gait and reactive-recovery from slip-induced falls) in all three planes of reference.
2. Methods
2.1. Subjects
Nine healthy young (mean age: 23.6 (SD 4.8) years; height: 1.67 (SD 0.10) m; weight: 65.5 (SD 8.4) kg) and nine healthy elderly adults (mean age: 73.6 (SD 4.4) years; height: 1.66 (SD 0.07) m; weight: 74.6 (SD 12.6) kg), who came from a large-scale slip-fall experiment [16], were selected to be analyzed in the current study. Informed consent was approved by the IRB of Virginia Polytechnic Institute and State University and was obtained from all of the participants. Self-reported medical histories indicated that all participants were physically healthy.
2.2. Instruments and procedures
Detailed experimental settings and protocols have been documented elsewhere [16,17]. Briefly, walking trials were conducted on a linear walkway (1.5 m × 15.5 m) embedded with two force-plates (BERTEC, Type 4550-08, Bertec Corporation, OH, USA), one of which was movable. Three-dimensional motion was captured by a six-camera motion analysis system (ProReflex MCU 120, Qualisys Medical AB, Sweden) with the marker configuration described by Lockhart et al. [18]. Participants were protected by an overhead fall-arresting harness system. Soundproof earmuffs were provided to the participants to block possible noise (e.g., the experimenter moving and the sliding the floor). Participants were instructed to look straight forward during walking to avoid visual cues from the floor surfaces. A clear slippery mixture (soap:water = 2:3) was applied to the movable force-plate to reduce the surface coefficient of friction (COF) (dynamic COF was tested to be 0.07).
Participants were instructed to walk back and forth along the walkway for 15 min. During the 15 min walking session, a normal walking trial was collected for each participant. Afterwards, without the subject’s knowledge, a slippery condition was induced to each participant to collect the slip-recovery data with few exceptions (i.e., if the participant completely missed the slippery surface during the first slip trial without apparent gait modification, a second slippery trial was induced following a few more normal walking cycles). At the most, two slippery trials were collected for each participant.
2.3. Data reduction
Participants with successful reactive-recovery trials were selected using the screening criteria. As previously stated, human reactive responses while walking across slippery floor surfaces can be categorized into a recovery or a fall. To be considered a fall, the slip distance must exceed 10 cm, peak sliding heel velocity must exceed the whole body COM velocity while slipping, and the participant’s body must drop toward the floor after slipping and be arrested by the harness before impact (assessed by visual inspections of video recordings of the actual slip trials) [6]. All other slip trials were identified as reactive-recovery. Furthermore, those participants who successfully recovered with two feet (i.e., stance foot and swing foot) on one force-plate were excluded from the current study due to the difficulty in performing inverse dynamics analyses.
Three-dimensional joint moments were calculated via the inverse dynamics approach [19]. The detailed procedure can be found in a previous publication [16]. Joint moments were normalized to the participant’s body mass, unless specified otherwise.
Characteristics of reactive joint moments were quantified by two variables: peak magnitude (JMM) and rate of development (JMR). JMM was defined as the maximum moment magnitude from heel-contact (HC) to toe-off of the perturbed (slipping) foot in each reference plane. JMR was defined as the ratio between the JMM and the time from HC to instance of peak joint moment, representing the speed of peak moment generation. Higher JMR suggested faster peak joint moment generation. Note that JMR can only apply to reactive-recovery trials.
2.4. Statistical analysis
A three-way mixed-factor MANCOVA test was performed on JMM measures at the ankle, knee, and hip joints. There were three independent variables: age groups (young and elderly), walking conditions (normal and reactive-recovery), and plane of reference (frontal, sagittal, and transverse). Due to the focus of the study, post hoc univariate ANCOVAs of aging effect were performed as needed.
For JMR measures, two-way mixed-factor ANCOVA tests were performed with age group (young and elderly) and plane of reference (frontal, sagittal, and transverse) being the independent variables. Post hoc univariate ANCOVA tests of aging effect were performed as needed.
For the above tests, walking velocity was considered as a covariate. All of the statistical analyses were performed in SAS 11.0 (SAS Institute Inc., USA). A significance level of p ≤ 0.05 was used throughout the tests.
3. Result
General joint moment patterns associated with normal walking trials and reactive-recovery trials of the young and the elderly are illustrated in Figs. 1–3. At the ankle joint, the sagittal joint moments generated after an initial silent phase (~20–25% of stance) were dominated by the dorsiflexor net moment during reactive-recovery trials (Figs. 1 and 2) contrary to the plantar-flexor-dominated net moment generated during normal walking trials (Fig. 3). At the knee joint, the sagittal joint moments generated after an initial silent phase were governed by knee extensors (Figs. 1 and 2). At the hip joint, the sagittal joint moments generated were characterized by two major extensor phases separated by a brief gap (Figs. 1 and 2). In the frontal and transverse planes of the ankle, knee, and hip joints, joint moments generated after an initial silent phase rapidly reached peak joint moment. For ease of comparison, ensemble average profiles of joint moments during normal walking and reactive-recovery are presented in Fig. 3.
Fig. 1.

Joint moment profiles generated by the younger adults during reactive-recovery (shaded areas represent ±1SD; joint moments were normalized with body mass; time was scaled relative to the stance time during normal walking).
Fig. 3.

Comparison of mean joint moment generated by the elderly and young during normal walking and reactive-recovery (bold solid curve: young/reactive-recovery; solid curve: young/normal; bold dash curve: elderly/reactive-recovery; dash curve: elderly/normal); joint moments were normalized with body mass; time was scaled relative to the stance time during normal walking.
Fig. 2.

Joint moment profiles generated by the elderly during reactive-recovery (shaded areas represent ±1SD; joint moments were normalized with body mass; time was scaled relative to the stance time during normal walking).
Statistically, the MANCOVA test on JMM indicated significant three-way interaction effect (Wilk’s Lambda = 0.0003) among age, condition, and plane of reference. Thus, a post hoc univariate ANCOVA was performed at each location (joint by plane of reference) during recovery condition. As illustrated in Fig. 4, significant aging effects on JMM were present in the ankle sagittal (p = 0.0084), knee sagittal (p = 0.0016), knee transverse (p = 0.0003), and hip transverse (p = 0.0120) planes. Specifically, compared to the elderly, the younger adults generated significantly higher peak joint moments at the ankle sagittal, knee sagittal, and hip transverse planes, but lower moments at the knee transverse plane.
Fig. 4.

Mean peak joint moments between young and elderly during recovery; error bar indicates 1SD; *indicates significant aging effect.
It should be noted that at both the ankle and hip joints, the moments were generated in a similar way between the young and the elderly. For example, at the ankle joint, JMM was highest in the sagittal plane and smallest in the transverse plane (Fig. 4). Nevertheless, at the knee joint, the way that the JMMs were generated was found to be quite different between the young and the elderly. For the younger adults, the peak joint moments were highest in the sagittal plane, while for the elderly, the peak joint moment were highest in the frontal plane (Fig. 4).
Two-way ANCOVA tests on the JMR found a significant interaction effect between age and plane of reference at the ankle (p = 0.0037), knee (p = 0.0011), and hip (p < 0.0001) joint. Post hoc univariate ANCOVA further indicated significant aging effects on JMR in the ankle sagittal (p = 0.0109), knee sagittal (p = 0.0033), knee transverse (p = 0.0030), and hip transverse (p = 0.0115) planes (Fig. 5). Specifically, compared to the elderly, the young adults were found to generate reactive joint moments significantly faster in the ankle sagittal, knee sagittal and hip transverse planes, though slower in the knee transverse plane. JMR was defined to measure the rate of joint moment increase during recovery. However, the hip sagittal joint moment exhibited a decreased pattern (i.e., the peak occurred in the beginning of the recovery phase and transitioned afterwards) (Figs. 1 and 2). Thus, JMR was not calculated in the hip sagittal plane.
Fig. 5.
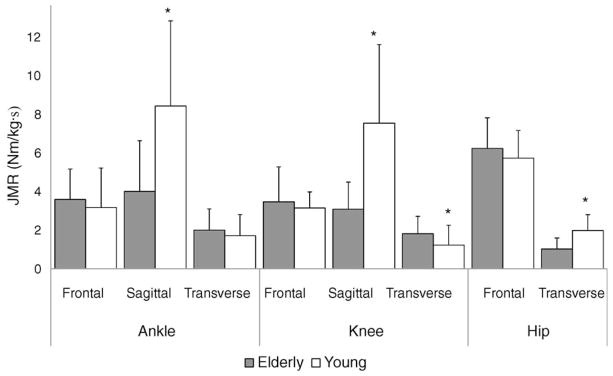
Mean rate of moment generation between young and elderly during recovery; error bar indicates 1SD; *indicates significant aging effect.
Similar to JMM, the way that JMR was generated by the young and the elderly was similar at the ankle and hip joints, but different at the knee joint. At the knee joint, the rate of moment generation was highest in the sagittal plane for the young but in the frontal plane for the elderly (Fig. 5).
4. Discussion
Characteristic joint moment patterns were observed in both normal walking and reactive-recovery conditions. The average joint moment profiles in normal walking obtained from the study were in general agreement with previous literature [20–22]. During reactive-recovery, consistent joint moment profiles described a dorsiflexor-dominant ankle joint moment, an extensor-dominant knee joint moment, and an M-shaped extensor-dominant hip joint moment in the sagittal plane for all of the participants. These recovery joint moment profiles were considerably different from previous literature [23], which quantified joint moments in normal gait, reactive-recovery and fall trials. Furthermore, the peak joint moments obtained in the current study reached, on average, as high as 3.66, 3.33, and 1.28 Nm/kg for the ankle, knee, and hip joints, respectively, for the younger group. These moment peaks were higher than the previous findings, which were less than 1 Nm/kg on average.
The discrepancies in recovery joint moment profiles between the current study and the literature can be attributed to the different time scales adopted in different studies. In a previous study, the time scale was limited to 55% of the stance phase. In the current study, however, the time scale was extended to 85% of the stance phase. As shown in Fig. 3, major reactive joint moments were developed during second half of the time scale. Both Rogers et al. [24] and Do et al. [25] identified two phases of balance recovery during protective stepping: (1) an initial voluntary reaction phase and (2) a controlled reactive action phase. It can then be plausibly assumed that the first half of the time scale (up to 55% of the stance phase) corresponds to the voluntary reaction phase, while the second half, which was elaborated in the current study, reflects the controlled reactive-recovery strategy. Thus, it is reasonable that the time scale for studying slip-and-fall studies should be extended if the controlled recovery process rather than voluntary initiation process is desired. Additionally, the current results were also different from those obtained by Ferber et al. [26]. Such differences can be explained by the differences in the adopted experimental protocols. In the current study, unexpected slips were created by a slippery floor surface, rather than a simulated floor movement as in the previous study [26].
Based on the differences in magnitude of peak joint moments between normal gait and slip-recovery trials, lower extremity joints assumed different functional roles in response to unexpected slips (i.e., normal gait vs. reactive-recovery): the ankle and knee joints actively served as the major actuator for balance recovery by producing considerably larger sagittal joint moments while the hip joint passively maintained upright posture of the upper body by increasing the frontal joint moment. In the current study, both age groups developed significantly higher peak joint moments in reactive-recovery than in normal walking, which was in favor of the proposed hypothesis about peak joint moment. Supported by other postural control studies [27,28], inability to generate required joint moments can contribute to slip-induced fall accidents. Instead of increasing peak joint moments to compensate for balance recovery (ankle and knee joints), the hip sagittal joint moments were found to be significantly reduced and the hip frontal joint moment was increased. It has been documented that one of the two major functions of the hip joint is to balance the upper body, which is accomplished mainly by frontal plane joint moment [29]. Thus, it can be speculated that during reactive-recovery, the hip joint was mainly involved in maintaining balance of the upper body.
Despite adopting a similar joint moment generation strategy, the elderly and young individuals distributed peak joint moments across the lower extremities differently during reactive-recovery. During normal walking, the sagittal joint moments were dominant compared to the frontal and transverse moments for both young adults and the elderly. During reactive-recovery, the younger group still relied on the ankle and knee sagittal joint moments to achieve balance recovery. For the elderly, however, the joint moments generated at the frontal plane increased to a level comparable to those at the sagittal plane (Fig. 4). In other words, the importance of the frontal moment generation was elevated for the elderly during reactive-recovery. This phenomenon may be plausibly explained by the limitation in available muscle strength of the elderly [9–11]. This limitation may force the elderly to activate adjacent muscle groups to assist in balance recovery, given the fact that peak joint moment observed in ankle and knee joints were no more than 2 Nm/kg in reactive-recovery conditions. These pronounced out-of-plane kinetics also justified the importance of implementing 3D analysis in the current study.
From the perspective of speed of peak joint moment generation, the elderly may be exposed to a higher risk of falling than their younger counterparts, even though both age groups achieved successful recovery in the current study. Although implicated, joint moment capacity assessments are needed to validate the above statement. The proposed hypothesis about JMR was confirmed by the significantly lower JMR found for the elderly than the younger individuals in several anatomical reference planes (the ankle sagittal, knee sagittal and hip transverse planes). JMR produced at the ankle and knee sagittal planes by the younger group were on average two times higher than those produced by the elderly. These deficits in moment generation speed can be another facet of age-related musculoskeletal degradation. Previous studies considered the rate of lower extremity joint moment development as an important variable that governs our ability to recover balance [27,28,30]. In this regard, although all of the individuals in the current study were able to maintain balance, the age-related limitation in lower extremity muscle strength may impose a greater risk of falls.
In summary, during successful reactive-recovery from an unexpected slip, the roles of different joints were similar for both age groups. The ankle and knee joints were critical in correcting sagittal plane motion disturbance, while the hip joint was mainly responsible for stabilizing upper body balance in the frontal plane. However, the out-of-plane moment generation strategy varied considerably between the young and the elderly.
Acknowledgments
This publication was partly supported by Cooperative Agreement Number UR6/CCU617968 from Centers for Disease Control and Prevention (CDC/NIOSH, K01-OH07450), and Whitaker Foundation Biomedical Engineering Research Grant. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC/NIOSH and Whitaker Foundation.
Footnotes
Conflict of interest
No conflict of interest for this manuscript.
References
- 1.National Safety Council. Accidents Facts 1998 edition. Itasca, IL: 1998. [Google Scholar]
- 2.Center for Disease Control. CDC Facts Book 2000/2001. 2000 [Google Scholar]
- 3.Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non-fatal falls among older adults. Injury Prevention. 2006;12(5):290–5. doi: 10.1136/ip.2005.011015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Perkins PJ. Measurement of slip between the shoe and ground during walking. American Society of Testing and Materials: Special Technical Publication. 1978;649:71–87. [Google Scholar]
- 5.Strandberg L, Lanshammar H. The dynamics of slipping accidents. Journal of Occupational Accidents. 1981;3(3):153–62. [Google Scholar]
- 6.Lockhart TE, Woldstad JC, Smith JL. Assessment of Slip Severity Among Different Age Groups. ASTM STP 1424, Metrology of Pedestrian Locomotion and Slip Resistance. 2002 [Google Scholar]
- 7.Lockhart TE, Woldstad JC, Smith JL. Effects of age-related gait changes on the biomechanics of slips and falls. Ergonomics. 2003;46(12):1136–60. doi: 10.1080/0014013031000139491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Do MC, Schneider C, Chong RKY. Factors influencing the quick onset of stepping following postural perturbation. Journal of Biomechanics. 1999;32(8):795–802. doi: 10.1016/s0021-9290(99)00067-6. [DOI] [PubMed] [Google Scholar]
- 9.Bonder B, Wagner MB. Functional performance in older adults. Philadelphia: F.A. Davis; 1994. [Google Scholar]
- 10.Larsson L, Grimby G, Karlsson J. Muscle strength and speed of movement in relation to age and muscle morphology. Journal of Applied Physiology. 1979;46(3):451–6. doi: 10.1152/jappl.1979.46.3.451. [DOI] [PubMed] [Google Scholar]
- 11.Campbell AJ, Borrie MJ, Spears GF. Risk-factors for falls in a community-based prospective-study of people 70 years and older. Journals of Gerontology. 1989;44(4):M112–7. doi: 10.1093/geronj/44.4.m112. [DOI] [PubMed] [Google Scholar]
- 12.Owings TM, Pavol MJ, Grabiner MD. Mechanisms of failed recovery following postural perturbations on a motorized treadmill mimic those associated with an actual forward trip. Clinical Biomechanics. 2001;16(9):813–9. doi: 10.1016/s0268-0033(01)00077-8. [DOI] [PubMed] [Google Scholar]
- 13.Weerdesteyn V, Nienhuis B, Duysens J. Advancing age progressively affects obstacle avoidance skills in the elderly. Human Movement Science. 2005;24(5–6):865–80. doi: 10.1016/j.humov.2005.10.013. [DOI] [PubMed] [Google Scholar]
- 14.Pai YC, Yang F, Wening JD, Pavol MJ. Mechanisms of limb collapse following a slip among young and older adults. Journal of Biomechanics. 2006;39(12):2194–204. doi: 10.1016/j.jbiomech.2005.07.004. [DOI] [PubMed] [Google Scholar]
- 15.Wojcik LA, Thelen DG, Schultz AB, Ashton-Miller JA, Alexander NB. Age and gender differences in peak lower extremity joint torques and ranges of motion used during single-step balance recovery from a forward fall. Journal of Biomechanics. 2001;34(1):67–73. doi: 10.1016/s0021-9290(00)00152-4. [DOI] [PubMed] [Google Scholar]
- 16.Liu J, Lockhart TE. Comparison of 3D joint moments using local and global inverse dynamics approaches among three different age groups. Gait & Posture. 2006;23(4):480–5. doi: 10.1016/j.gaitpost.2005.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu J, Lockhart TE. Role of ankle joint in successful reactive-recovery: a 3D joint moment analysis. Human Factors and Ergonomics Society 48th Annual Meeting; 2004. [Google Scholar]
- 18.Lockhart TE, Woldstad JC, Smith JL, Ramsey JD. Effects of age related sensory degradation on perception of floor slipperiness and associated slip parameters. Safety Science. 2002;40(7–8):689–703. doi: 10.1016/S0925-7535(01)00067-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bresler B, Frankel JP. The forces and moments in the leg during level walking. Transactions of American Society of Mechanical Engineers. 1950;72:27–36. [Google Scholar]
- 20.Eng JJ, Winter DA. Kinetic analysis of the lower limbs during walking: what information can be gained from a three-dimensional model? Journal of Biomechanics. 1995;28(6):753–8. doi: 10.1016/0021-9290(94)00124-m. [DOI] [PubMed] [Google Scholar]
- 21.Allard P, Lachance R, Aissaoui R, Duhaime M. Simultaneous bilateral 3-D able-bodied gait. Human Movement Science. 1996;15(3):327–46. [Google Scholar]
- 22.Glitsch U, Baumann W. The three-dimensional determination of internal loads in the lower extremity. Journal of Biomechanics. 1997;30(11–12):1123–31. doi: 10.1016/s0021-9290(97)00089-4. [DOI] [PubMed] [Google Scholar]
- 23.Cham R, Redfern MS. Lower extremity corrective reactions to slip events. Journal of Biomechanics. 2001;34(11):1439–45. doi: 10.1016/s0021-9290(01)00116-6. [DOI] [PubMed] [Google Scholar]
- 24.Rogers MW, Hedman LD, Johnson ME, Martinez KM, Mille ML. Triggering of protective stepping for the control of human balance: age and contextual dependence. Cognitive Brain Research. 2003;16(2):192–8. doi: 10.1016/s0926-6410(02)00273-2. [DOI] [PubMed] [Google Scholar]
- 25.Do MC, Breniere Y, Brenguier P. A biomechanical study of balance recovery during the fall forward. Journal of Biomechanics. 1982;15:933–9. doi: 10.1016/0021-9290(82)90011-2. [DOI] [PubMed] [Google Scholar]
- 26.Ferber R, Osternig LR, Woollacott MH, Wasielewski NJ, Lee JH. Reactive balance adjustments to unexpected perturbations during human walking. Gait & Posture. 2002;16(3):238–48. doi: 10.1016/s0966-6362(02)00010-3. [DOI] [PubMed] [Google Scholar]
- 27.Chandler JM, Duncan PW, Studenski SA. Balance performance on the postural stress test: comparison of young adults, healthy elderly, and fallers. Physical Therapy. 1990;70:410–5. doi: 10.1093/ptj/70.7.410. [DOI] [PubMed] [Google Scholar]
- 28.Wojcik LA, Thelen DG, Schultz AB, Ashton-Miller JA, Alexander NB. Age and gender differences in single-step recovery from a forward fall. Journal of Gerontology. 1999;54:44–50. doi: 10.1093/gerona/54.1.m44. [DOI] [PubMed] [Google Scholar]
- 29.Winter DA. Moments of force and mechanical power in jogging. Journal of Biomechanics. 1983;16(1):91–7. doi: 10.1016/0021-9290(83)90050-7. [DOI] [PubMed] [Google Scholar]
- 30.Robinovitch SN, Heller B, Lui A, Cortez J. Effect of strength and speed of torque development on balance recovery with the ankle strategy. Journal of Neurophysiology. 2002;88(2):613–20. doi: 10.1152/jn.2002.88.2.613. [DOI] [PubMed] [Google Scholar]