

Abstract
Objective
Compare feedback strategies in three versions of an educational game.
Participants
Study abroad students (N = 482) participated by playing the game and completing pre-game/post-game surveys January-March 2010.
Methods
This study employed an experimental design. Primary outcome measures were knowledge gain, player-satisfaction, and risk perception.
Results
One-third had previously traveled to a malaria-risk region and two-thirds planned to do so. Baseline malaria knowledge was low. Post-game knowledge and risk perception were significantly higher than pre-game, irrespective of past travel status. The group that automatically received explanatory feedback following game decisions scored higher for mean knowledge gain, without differences in player-satisfaction.
Conclusions
The challenges of designing a feedback strategy to support Web-based learning make these results highly relevant to health educators developing interactive multimedia interventions. The increasing number of students traveling to higher-risk destinations demands attention. Both malaria-naive and malaria-experienced students would benefit from this approach to travel health education.
Keywords: college, feedback, game design, malaria, risk reduction, study abroad, Web-based
Study abroad participation by U.S. college students has increased four-fold over the past twenty years, with a rapid expansion of programs in destinations that present unfamiliar health threats.1 Although there is evidence that students are putting themselves at risk by failing to engage in travel health prevention behaviors,2-8 the number of U.S. students who acquire malaria each year while studying abroad is unknown. First, there is no systematic reporting of how many U.S. study abroad students are diagnosed with malaria while abroad. Second, students diagnosed after returning to the U.S may be under-reported if they are categorized as something other than Student/Teacher on the Centers for Disease Control and Prevention (CDC) surveillance report (e.g., Tourism, Business, Visiting Friends/Relatives, Other or Unknown). Third, the merged CDC category of Student/Teacher makes it impossible to extract data for students alone. In light of these limitations and the possibility of missed diagnoses, there were 28 reports submitted in 2009 for individuals diagnosed and treated in the U.S. and categorized as Student/Teacher. This represents 4.2% of all U.S. cases, which includes Peace Corps volunteers, military personnel, and foreign-born nationals traveling to or emigrating to the U.S.9
Malaria was chosen as an exemplar for a travel health intervention because of fluctuating transmission intensity (by season and other factors) and the vital need for consistent use of prevention measures and for timely diagnosis and treatment.10 Malaria symptoms can be challenging to recognize because they are non-specific and may develop as early as seven days after initial exposure or as late as several months or more after returning to the US.10(p132) Because life-threatening malaria complications can develop quickly, travelers must recognize when to seek evaluation for symptoms and the importance of disclosing travel dates, destinations, and types of housing and activities while abroad.10(p131)
This study responds to an increasing need to educate study abroad students about health threats that may be encountered in other regions of the world. A Web-based game was developed by the authors and digital media specialists using a highly iterative build/test/revise process.11 User testing was conducted on four different approaches before arriving at a prototype that students indicated they would be willing to play online for ~20 minutes without incentive or classroom coercion. One important user test finding was that most students are unwilling to use a pre-game tutorial, so intuitive gameplay is essential, i.e., learning ‘how’ to play while playing the game. The final prototype was designed to be used as a stand-alone learning exercise or as an instructor-guided activity to prepare students for travel to malaria-risk regions.
Theoretical Frameworks
The self-regulation model (SRM)12 and the cognitive theory of multimedia learning (CTML)13 are the theoretical frameworks that guided the development and evaluation of this interactive educational tool. Both the SRM and the CTML address human cognition and learning.
The SRM focuses on the personal understandings of health threats that influence associated health behavior.12(p42) The organizational structure for the development of the malaria content in the game and pre/post instruments could have been provided by a number of health behavior theories. One widely used framework is the health belief model,14 which is a value expectancy approach for understanding health behaviors that are motivated by a person’s mental calculations about their susceptibility to a health threat, the severity of a health threat, and the benefits and barriers associated with taking an action. In contrast, the SRM is an information-processing model in which both cognitive and emotional representations influence how a person responds to a health threat. Information about health threats is obtained from external (abstract/conceptual) sources and from experiential (concrete/perceptual) sources.12(p44)
The dimensions of an SRM cognitive representation are identity (labels and symptoms), cause, timeline, consequences, control/cure, and coherence. An SRM emotional representation is characterized by fear-related responses such as the degree of anxiety or worry associated with the specific health threat.12 (p48) In general, beliefs and behaviors are more likely to change in response to informational exposures that elicit a heightened emotional response.12(p45),15,16 Because malaria is a relatively unknown yet serious health threat for this population, the representational dimensions of the SRM were most appropriate for structuring the malaria knowledge test items (Table 1) and the game content.
Table 1.
SRM Dimensions Used to Measure Malaria Knowledge and Risk Perception
| Dimensions | Cognitive Exemplars for Knowledge Test Items—18 items 3 items per dimension (5 response options per item) |
|---|---|
| Identity | Which of the following symptoms are most common with malaria infection? |
| Cause | How is malaria usually spread from person to person? |
| Timeline | What is the shortest amount of time between being infected and noticing symptoms? |
| Consequences | Which action is best to minimize the negative consequences of malaria? |
| Control/Cure | Why might travelers going to malaria-risk regions be advised to take anti-malarial medication? |
| Coherence | While in Kenya, Michael takes an anti-malarial drug daily, but his roommate does not. His roommate is diagnosed with malaria and receives medication to treat it. What should Michael do to protect himself? |
|
| |
| Emotion | Risk Perception − 2 items (5-point scale) |
| Worry | How worried are you that you might contract malaria if you traveled to a malaria-risk destination? |
| Likelihood | If you traveled to a malaria-risk destination, how likely do you think it is that you would be infected? |
The impact of health games on knowledge, and on personal motivation to engage in risk reduction behaviors, is a promising area for research because of the potential that simulated experiences hold for tapping into core beliefs and emotions.17 Games invite learners to test assumptions without actual risk to their health, while offering interactive challenges and just-in-time information that can enhance higher-order thinking skills.18,19 The CTML builds upon prior theory and evidence focused on learner achievement, engagement, control, and cognitive load while extending this body of research to instructional technology.20-25
The CTML is based on the assertion that people learn more deeply from words and pictures than from words alone, although this does not imply that all multimedia presentations are equally effective. 13(p31,32) The emphasis is on approaches that are learner-centered, while technology is considered to be one of many tools to support well-designed learning experiences. A central assumption is that visual/pictorial and auditory/verbal information are processed using distinct channels to organize incoming information into mental representations that individuals respond to and store in memory.26 This dual-coding theory posits that individuals transfer back and forth between channels depending on whether incoming communications are visual or auditory or both. There is evidence that memory is enhanced when information is obtained using both channels, with the exception of exposures that produce cognitive overload, i.e., when the processing capacity available in the visual and auditory channels is exceeded.27 Cognitive overload is more likely when learners encounter high redundancy between channels, complex learning tasks (especially for novices), or extraneous words, pictures or sounds that diminish learner-focus.28 Similar to the assumptions of the SRM, meaningful learning occurs when the learner actively engages in cognitive activity, selects the most salient information, organizes it into a logical mental picture, and integrates the new information into memory.29
In summary, both the SRM and CTML guided the study design, game development, construction of the pre/post instruments, and choice of outcome measures. Two hypotheses were used to test CTML assumptions about how different approaches to explanatory feedback impact knowledge gain and player-satisfaction. The SRM was used to explore the impact of game condition on risk perception. Future work will use a longitudinal design to examine the relationship between risk perception and behavior for students going to malaria-risk regions.
Elements of Game Design
In the travel game developed by the authors, Life and Death in the Age of Malaria,30 players sequentially assume the identity of study abroad students departing for Brazil, Uganda, and India. Players have ample opportunity to experiment with different choices in each travel trajectory to see how decision patterns affect consequences, including the game characters’ final outcomes of healthy, disabled, or dead. The primary data sources for risk determination were the CDC Health Information for International Travel10 and the World Health Organization (WHO) publication International Travel and Health.31 The game objective is for players to make decisions that apply accurate malaria knowledge to game scenarios, thereby increasing the probability of the three characters remaining healthy during and after travel. However, this learning tool was designed to increase malaria knowledge among players who are motivated to preserve life as well as those who prefer to disable or kill the characters in the spirit of exploration of game rules and consequences.
To provide players with directional information about decision consequences, each decision was tracked using decision labels displayed in the Your Decisions panel. These labels were color-coded green or red to indicate the type of impact, with a corresponding symbol to aid players with colorblindness (green √ for positive and red X for negative). A malaria knowledge meter and a numeric game score additionally reflected the points being gained or lost in response to gameplay decisions. Optional resources include a travel health specialist character with action-specific advice, and a library from which static information could be accessed at all times (Figure 1).
Figure 1.
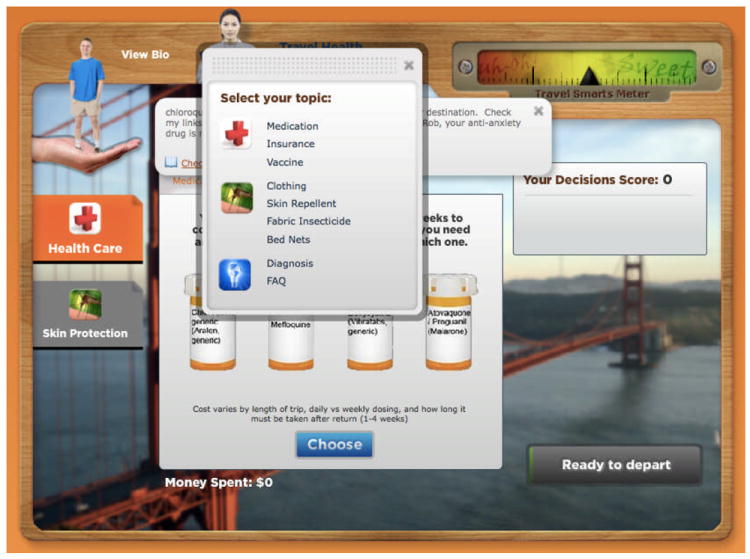
Library resources were available at all times. The travel health specialist, if consulted, offered tailored advice for each action (see upper text box behind library options in this screen shot).
It was imperative that players not leave the game with mistaken beliefs that could later lead to serious consequences during actual travel. Yet delivering timely explanatory feedback without disrupting gameplay presents a significant challenge. Feedback was therefore selected as a variable of interest. While its importance in promoting learning is well established, in-game feedback can lead to diminished player-satisfaction if the mode of delivery is perceived as confusing, intrusive or beyond player control.22(p100) The CTML assumption that learners have limits on their working memory suggests that it is counterproductive to provide educational content beyond what can be realistically processed for long-term retention and transfer. The timing, amount, and type of feedback can be structured to promote retention, for example, by drawing connections through ‘just-in-time’ and chunked presentation of information.13(p46)
Two of the game’s feedback conditions provided a pop-up text box with explanatory feedback; either automatically with each decision (automated) or when a player chose to click on a decision label to access feedback (player-controlled) (Figure 2). The third condition lacked the pop-up text box (no explanatory feedback). In order to determine why a decision had a positive or negative impact, players in the no explanatory feedback group had to rely on baseline directional information (positive/green versus negative/red in the Your Decisions panel and on the knowledge meter), the specialist advice, and resource library information.
Figure 2.
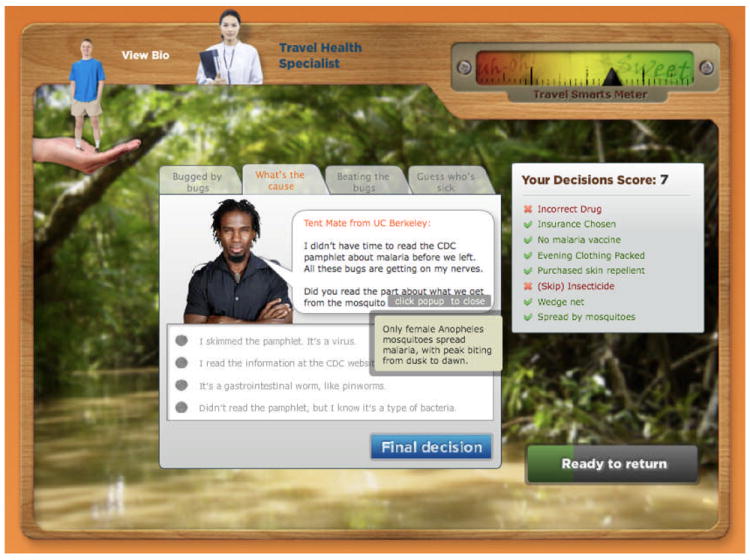
The feedback pop-up box was accessible to players in the automated and player-controlled explanatory feedback conditions.
Study Objective
We compared three versions of a malaria game to determine the most advantageous approach for the delivery of feedback in response to player decisions and for providing in-game resource information. The primary outcome measures were knowledge gain, player-satisfaction, and risk perception. Two research hypotheses were derived from theory to explore the optimization of the delivery of explanatory feedback.
For the first hypothesis, it was expected that participants exposed to explanatory feedback automatically with each game decision would have a significantly higher mean knowledge gain compared with the other feedback strategies due to the role of explanatory feedback as a just-in-time aid to conceptual understanding.22(p 110) It was anticipated that participants exposed to the player-controlled game version would only occasionally choose to view additional explanatory feedback due to limited insight into the degree of effort needed to maximize their own learning.20(p 100) Participants receiving no explanatory feedback were expected to have a lower knowledge gain due to a greater likelihood for misunderstanding why an action caused a particular consequence (i.e., incorrect attribution), unless mitigated by use of the travel health specialist, the library, or both. 22(p 110,111)
For the second hypothesis, it was expected that participants who could access explanatory feedback when desired (player-controlled version) would have a significantly higher mean player-satisfaction rating compared with the other feedback strategies. Participants exposed to explanatory feedback automatically with each game decision were expected to have a lower satisfaction rating because the pop-up text could be perceived as force-fed information (reduced content control).25(p 289,301) Participants who received no explanatory feedback were also expected to have a lower satisfaction rating due to the time and effort required to access explanatory information through the travel health specialist character and resource library, and the potential frustration or confusion among those participants who never or rarely chose to access this explanatory information.
METHODS
Design and Sample
This study used an experimental design to compare three versions of an educational game (Figure 3). Study abroad students were recruited from the University of Minnesota Twin Cities campus and six University of Wisconsin System four-year campuses. Inclusion criteria consisted of current enrollment status as a student or within one-year post-graduation, and being included on campus e-mail distribution lists for study abroad students. Campus administrative collaborators managed all protocol mailings; study investigators had no direct contact with these e-mail distribution lists. The game and pre/post surveys were accessed by computer, and all elements of participation were anonymous. Movement through the protocol was digitally tracked and time-stamped after participants linked to the study protocol.
Figure 3.
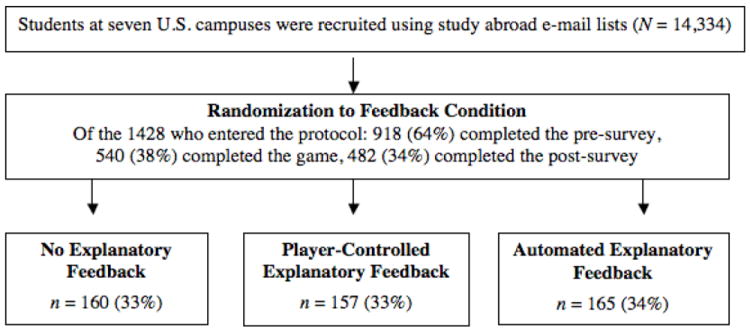
Participant recruitment and randomization to condition.
A recruitment message was sent within a seven-day window prior to the letter of invitation to explicitly state that a broad representation of students was being sought. Next, the invitation was distributed to the same list, followed by a reminder message a week later. All messages contained a personal note from the campus administrative collaborator and contact information for the study’s principal investigator. Data were collected using a phased schedule for campus deployment in January and February 2010. There was no incentive for participation, and students were informed that they should participate only once. Based on a review of the literature and a 32% participation rate from a prior e-mail survey of study abroad students without incentive (N = 318), 7 it was predicted that approximately 30% of participants who began the study protocol would complete it.
Procedure
Approval was obtained from each campus Institutional Review Board prior to study deployment. An assigned study abroad program administrator on each campus distributed the study information. After participants read the informed consent information, consent was implied when a link within the invitation letter was used to access the pre-game survey, with sequential links to the game and then to the post-game survey. Random assignment to one of three game conditions was accomplished upon entry to the study protocol through a computer-generated program that was not apparent to participants. Once the post-game survey was submitted, participants were directed to a summary site where they were thanked for their participation and provided with their pre/post knowledge scores along with additional travel health links and a brochure titled Preventing Malaria in Travelers.32
Measurement: Game
Each game action was reflected in a numeric score and in a color-coded knowledge meter as a scaled item with point anchors of -24 to +24 for the first two characters, and -26 to +26 for the third. Players began at zero (0), and points were gained and lost in 1- and 2-point increments as players made game decisions related to malaria knowledge and risk reduction. Once a game character developed symptoms, a game rubric determined whether that character had acquired malaria or had symptoms for another reason. Characters were more likely to be infected with malaria when players failed to select effective prevention measures before departure and when actions demonstrated less accurate malaria knowledge. If infected, secondary outcomes included recovery, disability, or death. This rubric (game logic) utilized both a cumulative decision score and the specific action taken once the character becomes symptomatic. The activities captured digitally for analysis were duration of gameplay, character outcomes (healthy, disabled, or dead), and mouse-click frequency counts for accessing the travel health specialist, resource library, and explanatory feedback in the player-controlled condition (frequency counts were not relevant for the other two conditions since explanatory feedback was delivered ‘always’ or ‘never’).
Measurement: Pre-game and Post-game Surveys
The pre-game survey consisted of a malaria knowledge test (MKT), an 18-item multiple-choice instrument with five response options, and two additional risk perception items.33 The multiple-choice items were scored on a 2-point scale (0 = incorrect and 1 = correct). The post-game survey included all pre-survey items plus nine demographic items, one player-satisfaction item, and an open-ended text box for comments. The demographic items were sex, race/ethnicity, age, academic status (grad/undergrad) and campus of origin, study abroad student status (interested, planning, abroad, returned), past travel to a malaria-endemic area, plans to travel to a malaria-endemic area, and frequency of playing computer or video games. A 5-point scale (0 = not at all, 4 = extremely) was used for the two pre-game and post-game risk perception items about malaria infection (How likely/How worried) and one post-game player-satisfaction item (Overall, how satisfied were you with the game experience?).
The pilot test of the initial MKT instrument was conducted with 13 students who were close to departure for a field experience at a malaria-endemic destination. A second pilot test was conducted with 36 pre-nursing students who had no prior classroom exposure to malaria information. Revisions were made, such as simplification of wording and refinement of distracter responses, based on these pilot tests and three cognitive interviews with students about the survey items. Face validity of the revised MKT was then tested with five study abroad student reviewers. Five travel health specialists reviewed the MKT for content validity, and a specialist from the UW Survey Center suggested formatting edits to increase online comprehension. Instrument reliability was established as part of the summative game evaluation. Kuder-Richardson formula 20 (KR-20) was used to assess internal consistency for the MKT dichotomous items scored as correct/incorrect. The pre/post results of 0.82 and 0.72 respectively demonstrate the reliability of these items as measures of malaria knowledge.
Data Analysis
The de-identified data from the pre/post surveys and from in-game tracking were exported into SPSS 16.0 (SPSS Inc., Chicago, IL, USA) and first analyzed using descriptive statistics. Examination of demographic characteristics and pre-test measures of knowledge and risk perception for equal distribution across game conditions (homogeneity of variance) met the assumptions of further statistical tests. Analysis of variance was used for three-way comparisons such as feedback conditions; Tukey-B was used for post-hoc comparisons. For two-way comparisons such as pre/post scores and ratings, t-tests were used. The level of significance was set at p < .05. Uniform codes were used for missing data, and no data were imputed for missing responses. For analysis of the open-text comments, initial themes were identified and codes were developed. Two additional researchers assigned codes to each comment. There was initial agreement on 222 (85%) of 260 items. The team resolved the 38 discrepancies by merging, renaming, or creating new categories until 100% consensus was reached.
RESULTS
Demographic data are summarized in Table 2. The MKT mean score for 18 items was 6.6 pre-game and 13.8 post-game (t = 39.38, df = 481, p < 0.001) with a large partial eta squared effect size (0.767) demonstrating a strong overall learning effect. The automated condition yielded a significantly higher mean knowledge gain F(2,482) = 6.5, p < 0.005 with a small partial eta squared effect size (0.026) for differences in knowledge gain between the three feedback conditions. There were no significant differences between conditions for satisfaction, which was rated as very to extremely satisfying by 65% of participants. Risk perception ratings for malaria increased significantly from pre- to post- (likelihood t = 3.08, p < 0.005; worry t = 3.54, p < 0.001) without significant differences between feedback conditions.
Table 2.
Participant Characteristics
| Mean age in years = 21 (SD 4.6) | ||
|---|---|---|
| n* | % | |
|
|
||
| Sex: female | 352 | 73 |
| Student status | ||
| Undergraduate | 421 | 92 |
| Graduate | 29 | 6 |
| Professional (Medicine and Law) | 6 | 1 |
| Racial/ethnic background | ||
| Asian | 30 | 7 |
| Black or African American | 12 | 3 |
| Hispanic or Latino/a | 10 | 2 |
| Native American or Alaskan Native | 10 | 2 |
| Native Hawaiian or Pacific Islander | 2 | 0.4 |
| White | 393 | 86 |
| Study abroad status | ||
| Interested, but no specific plans | 36 | 8 |
| Planning | 152 | 34 |
| Currently abroad | 76 | 17 |
| Returned | 187 | 35 |
| Prior travel to a malaria-risk region | ||
| Yes | 155 | 32 |
| No | 299 | 63 |
| Don’t know | 24 | 5 |
| Future travel to a malaria-risk region | ||
| Yes | 309 | 64 |
| No | 129 | 27 |
| Don’t know | 40 | 8 |
n may vary due to missing cases
The mean time duration to complete three travel trajectories was 18.5 minutes. The automated explanatory feedback group took significantly longer to complete the game (M = 20.3 min.) compared with the player-controlled group (17 min.) and the no explanatory feedback group (18 min.) F(2,482) = 5.9, p < 0.003. Most players (76%) made decisions that averted disability and death for all three game characters. The travel health specialist resource was accessed at least once by 77% of players, with a mean of 5.2 clicks out of 40 total decisions. The library resource was used by 44% of players, with a mean of 2.5 clicks. There were no significant differences between feedback conditions for mean use of these optional game resources. A decision label to access explanatory feedback in the player-controlled (discretionary) feedback group was clicked on by 62% of players, with a mean of 4.6 clicks out of 40 total decisions.
An SRM dimensional analysis was secondarily conducted. Significant knowledge gains occurred across all cognitive representational dimensions. The pre-test identified important misperceptions, such as not knowing that: the peak biting time for the mosquito vector is nighttime (82%); travelers can die within days of symptom onset (80%); the infectious agent is a parasite (68%); and there is no malaria vaccine currently available (49%). Participants who reported past travel to a malaria-risk region achieved higher percentages correct on the MKT (49% pre- and 80% post-) than those without this travel history (31% pre- and 76% post-).
Student feedback was analyzed using 260 comments provided in an open-ended text box on the post-game survey. Positive text comments (60%) described the experience as informative, fun, and engaging. The negative comments (32%) addressed game features (e.g., too long, repetitive), but also technical problems encountered with hardware/software functions (n = 10) and text legibility/readability issues (n = 10). The remaining comments (8%) were rated as neutral (e.g., sharing a personal experience with malaria infection or encouragement for pursuing this line of inquiry).
COMMENT
This comparison of three versions of a risk reduction game revealed low baseline malaria knowledge and a substantial short-term learning effect in all feedback conditions and travel groups (pre- and post-travel to a malaria-risk region). Hypothesis 1 was upheld: participants exposed to the automated explanatory feedback game version had the highest mean knowledge gain. Hypothesis 2 was not upheld: there were no significant differences in player-satisfaction between game versions. This suggests that learning may be supported by automatically providing explanatory feedback for each decision without diminishing player-satisfaction, despite a greater mean completion time. The satisfaction rating was high overall for an initial testable prototype.
Satisfaction with this delivery mode for health education is consistent with earlier work which found that the Internet was the most common source of health-related information in a collegiate population (N = 1202),34 and that college students (N = 743) want to find health information on the Internet.35 An acknowledged limitation of the Internet is confusion about the believability of information,34 (p560) but this can be countered on campus study abroad Websites by providing links to travel health content at authoritative sites such as the World Health Organization and the U.S. CDC, Department of State, and Central Intelligence Agency World Factbook. Interestingly, 17% of the students who completed the study protocol were abroad at the time of participation, including students in Africa and other destinations with less consistent Internet access.
The finding that risk perception ratings increased significantly following the game intervention is important in light of a 2007 survey of U.S. study abroad students (N = 318) that revealed an overall low perceived risk related to travel, with malaria rated in the bottom half of 18 travel health threats.7(p341) The value of increasing students’ perception of risk is that greater awareness of threat has been shown to be positively associated with risk reduction behaviors.36,37
Study findings further suggest that important concepts in brief-exposure educational games should not be embedded exclusively in resources located on the periphery of the user interface for the player to discover. For example, 23% of participants did not access the travel health specialist even once despite a flashing orange arrow displayed at the start of gameplay directing players to click on this icon. Further, the group with no access to the pop-up explanatory feedback text boxes used resources no more frequently than the other groups to support their comprehension of game content. Participants in the player-controlled group who chose to access explanatory feedback (62%) did so only 11% of the time. Therefore, providing explanatory feedback as part of the central action of the game, without relying on player initiative to seek information, may yield greater learning dividends for this population and purpose (i.e., education about a topic with serious health ramifications).
The number of participants reporting prior travel to malaria-endemic regions (32%) represents a significant departure from travel destinations of a generation ago.1 Even more significant from a risk reduction perspective is the finding that 64% of respondents plan to travel to a malaria-endemic region in the future, while 5% did not know whether they had ever visited a malaria-endemic location. These data underscore a growing hazard for student travelers by documenting the low pre-test levels of malaria knowledge for both novice learners and those reporting prior travel to malaria-risk regions. The average pre-test score for the latter group (49% correct) demonstrates both the complexity of malaria as an infectious disease and how cognitive representations can be resistant to change.
Overall, our findings are highly relevant to health educators who design interactive risk reduction interventions because providing the appropriate amount of guidance is a balancing act that involves the content domain, the instructional approach, individual knowledge acquisition processes, and multimedia features.25(p302) There is a threat of overloading students’ cognitive capacity with excessive, confusing, or distracting feedback. There is also a threat of providing insufficient feedback, which can result in missing important learning points and leaving the intervention with erroneous assumptions.27(p78,79)
Limitations
This research is limited because it tested only one content domain (malaria), one kind of learner (college students), and one region of the United States (Midwest). It also lacked the longitudinal data necessary to measure the long-term impact of a gaming intervention on knowledge and behavior. Participants who were female (73%) and white (86%) were over-represented, although this is consistent with national demographic data for study abroad students (on average 65% female and 82% white over the past decade).38 The response rate was low from a pool of 14,334 e-mail addresses, with 1428 students (10%) clicking on the digital link after reading the informed consent information in the e-mail letter of invitation. Of those students who entered the protocol, 482 (34%) completed it, versus a prediction of 30% based primarily on a prior online survey in this population.7 A low response rate was anticipated for a number of reasons: length of the study protocol (~30 minutes for pre/post surveys plus game) in the context of academic demands on time and focus, the lack of an incentive, and an indeterminate number of students who no longer used the e-mail address provided to the study abroad program or for any reason did not open the e-mail. Additionally, the e-mail invitations were distributed to all outgoing study abroad students and not just those traveling to malaria-risk regions. Sixty-four percent of participants indicated that they planned to travel to a malaria-risk region, reflecting the relevance of the game to this population.
Conclusions
Our results may enhance college health risk reduction efforts by providing evidence about the impact of a brief exposure educational game on student understanding of malaria risk and prevention measures. A one-time exposure to a Web-based game of 18-20 minutes duration significantly increased malaria knowledge and risk perception in both malaria-naive and malaria-experienced populations. This is important because accurate knowledge and awareness of risk are key precursors for motivating students to engage in risk reduction activities. Findings further suggest that providing explanatory feedback automatically following player decisions supports learning, and that this can be done without diminishing satisfaction with the game experience. These data also reveal patterns of in-game information-seeking behavior and contribute to the literature examining learner control in multimedia environments. Next steps are to use formative (user-testing) and summative evaluation data to make game revisions, and to conduct a randomized controlled trial to examine the associations between knowledge, risk perception, and risk reduction behavior before, during, and after travel to a malaria-risk region.
With a greater understanding of evidence-based design principles for interactive educational tools, this prototype can be adapted for delivery on phones and tablets and expanded to address other health threats encountered by student travelers. These additional health threats would ideally be tailored to the world region of most interest to the player, and might include other infectious diseases, motor vehicle accidents, drowning, falls, and personal security. This approach might also be adapted to meet the learning needs of other groups, such as U.S. healthcare providers, or residents of world regions who chronically face the same health risks that impact U.S. travelers.
Supplementary Material
Acknowledgments
This work was supported in part by the University of Wisconsin-Madison through an Academic Technology Engage Project award and School of Nursing Eckburg and Shapiro research awards; a Sigma Theta Tau/Beta Eta Chapter research award; a 2009 Sigma Theta Tau/Hugoton Foundation/American Nurses Foundation scholar award; and an NIH/NINR fellowship [F31 NR010425-01A2]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research or the National Institutes of Health.
Footnotes
An appendix to the article is featured as an online supplement at the publisher’s Web site.
References
- 1.Institute of International Education. Open Doors 2010: Report on International Educational Exchange. New York: IIE; 2010. [Google Scholar]
- 2.Abdullah AS, Hedley AJ, Fielding R. Prevalence of travel related illness amongst a group of Chinese undergraduate students in Hong Kong. J Travel Med. 2000;7:125–132. doi: 10.2310/7060.2000.00043. [DOI] [PubMed] [Google Scholar]
- 3.Aro AR, Vartti AM, Schreck M, Turtiainen, Uutela A. Willingness to take travel-related health risks—A study among Finnish tourists in Asia during the avian influenza outbreak. Int J Behav Med. 2009;16:68–73. doi: 10.1007/s12529-008-9003-7. [DOI] [PubMed] [Google Scholar]
- 4.Causer LM, Filler S, Wilson M, et al. Evaluation of reported malaria chemoprophylaxis failure among travelers in a US university exchange program. Clin Infect Dis. 2004;39:1583–1588. doi: 10.1086/425311. [DOI] [PubMed] [Google Scholar]
- 5.Hamer DH, Connor BA. Travel heath knowledge, attitudes and practices among United States travelers. J Travel Med. 2004;11:23–26. doi: 10.2310/7060.2004.13577. [DOI] [PubMed] [Google Scholar]
- 6.Han P, Balaban V, Marano C. Travel characteristics and risk-taking attitudes in youths traveling to nonindustrialized countries. J Travel Med. 2010;17:316–321. doi: 10.1111/j.1708-8305.2010.00444.x. [DOI] [PubMed] [Google Scholar]
- 7.Hartjes L, Baumann L, Henriques J. Travel health risk perceptions and prevention behaviors of U.S. study abroad students. J Travel Med. 2009;16:338–343. doi: 10.1111/j.1708-8305.2009.00322.x. [DOI] [PubMed] [Google Scholar]
- 8.Rodger AJ, Cooke GS, Ord R, et al. Cluster of falciparum malaria cases in UK Airport Emerg Infect Dis. 2008;14:1284–1286. doi: 10.3201/eid1408.080031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Centers for Disease Control and Prevention. Malaria Surveillance—United States, 2009. MMWR. 2011;60:1–15. [PubMed] [Google Scholar]
- 10.Centers for Disease Control and Prevention. CDC health information for international travel 2010. Atlanta: U.S. Department of Health and Human Services, Public Health Service; 2009. pp. 128–159. [Google Scholar]
- 11.Hartjes L. Dissertations and Theses. University of Wisconsin–Madison: CIC Institutions; 2010. The Development and Evaluation of a Malaria Risk Reduction Game for Travelers. [Google Scholar]
- 12.Leventhal H, Brisette I, Leventhal EA. The common-sense model of self-regulation of health and illness. In: Cameron LD, Leventhal H, editors. The Self-Regulation of Health and Illness Behavior. New York: Routledge; 2003. pp. 42–65. [Google Scholar]
- 13.Mayer RE. Cognitive theory of multimedia learning. In: Mayer RE, editor. The Cambridge Handbook of Multimedia Learning. Cambridge: Cambridge University Press; 2005. pp. 31–48. [Google Scholar]
- 14.Rimer BK. The health belief model. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior and Health Education. San Francisco: John Wiley & Sons; 2008. pp. 45–62. [Google Scholar]
- 15.Brownlee S, Leventhal H, Leventhal EA. Regulation, self-regulation, and construction of the self in the maintenance of physical health. In: Boekaerts M, Pintrich PR, Zeidner M, editors. Handbook of Self-Regulation. San Diego: Academic Press; 2000. pp. 369–416. [Google Scholar]
- 16.Epstein S. Integration of the cognitive and psychodynamic unconscious. Am Psychol. 1994;49:709–24. doi: 10.1037//0003-066x.49.8.709. [DOI] [PubMed] [Google Scholar]
- 17.Squire K, Jenkins H. Harnessing the power of games in education. Insight. 2003;3:7–33. [Google Scholar]
- 18.de Freitas S, Neumann T. The use of ‘exploratory learning’ for supporting immersive learning in virtual environments. Computers and Educ. 2009;52:343–352. [Google Scholar]
- 19.Klopfer E, Osterweil S, Groff J, et al. Using the technology of today, in the classroom today. Educ Arcade/MIT. 2009:1–23. [Google Scholar]
- 20.Clark RE. Antagonism between achievement and enjoyment in ATI studies. Educ Psychol. 1982;17:92–101. [Google Scholar]
- 21.Mayer R, Moreno R. Nine ways to reduce cognitive load in multimedia learning. Educ Psychol. 2003;38:43–52. [Google Scholar]
- 22.Moreno R. Decreasing cognitive load for novice students: effects of explanatory versus corrective feedback in discovery–based multimedia. Instr Sci. 2004;2:99–113. [Google Scholar]
- 23.Moreno R, Mayer R. Role of guidance, reflection, and interactivity in an agent–based multimedia game. J Educ Psychol. 2005;97:117–128. [Google Scholar]
- 24.Moreno R, Mayer R. Interactive multimodal learning environments: contemporary issues and trends. Educ Psychol Rev. 2007;19:309–326. [Google Scholar]
- 25.Scheiter K, Gerjets P. Learner Control in Hypermedia. Educ Psychol Rev. 2007;19:285–307. [Google Scholar]
- 26.Paivio A. Mental Representations: A Dual Coding Approach. New York: Oxford University Press; 1990. [Google Scholar]
- 27.Plass J, Kalyuga S, Leutner D. Individual differences and cognitive load theory. In: Plass J, Moreno R, Brunken R, editors. Cognitive Load Theory. Cambridge: Cambridge University Press; 2010. [Google Scholar]
- 28.Patel V, Yoskowitz N, Arocha J, et al. Cognitive and learning sciences in biomedical and health instructional design: a review with lessons for biomedical informatics education. J Biomed Inform. 2009;42:176–197. doi: 10.1016/j.jbi.2008.12.002. [DOI] [PubMed] [Google Scholar]
- 29.Mayer R. Applying the science of learning: evidence–based principles for the design of multimedia instruction. Am Psychol. 2008;61:760–769. doi: 10.1037/0003-066X.63.8.760. [DOI] [PubMed] [Google Scholar]
- 30.Hartjes L, Baumann L. [February 10, 2012];Life and Death in the Age of Malaria. Available at: http://64.34.170.16/%7Emalaria/index.php?survey=0&mode=1 (automated explanatory feedback version)
- 31.World Health Organization. International Travel and Health. Geneva: WHO; 2011. [Google Scholar]
- 32.Centers for Disease Control and Prevention. [February 10, 2012];Preventing Malaria in Travelers. Available at: http://www.cdc.gov/malaria/travelers/
- 33.Hartjes L, Baumann L. [February 10, 2012];Malaria Knowledge Test. Available at: https://research.uwsc.wisc.edu/p9724/p9724.php.
- 34.Kwan MYW, Arbour-Nicitopoulos KP, Lowe D, Taman S, Faulkner GEJ. Student reception, sources, and believability of health-related information. J Am Coll Health. 2010;58:555–562. doi: 10.1080/07448481003705925. [DOI] [PubMed] [Google Scholar]
- 35.Escoffery C, Miner KR, Adame DD, Butler S, McCormick L, Mendell E. Internet use for health information among college students. J Am Coll Health. 2005;53:183–188. doi: 10.3200/JACH.53.4.183-188. [DOI] [PubMed] [Google Scholar]
- 36.Brewer NT, Chapman GB, Gibbons FX, Gerrard M, McCaul KD, Weinstein ND. Meta-analysis of the relationship between risk perception and health behavior: the example of vaccination. Health Psychol. 2007;26(2):136–145. doi: 10.1037/0278-6133.26.2.136. [DOI] [PubMed] [Google Scholar]
- 37.Weinstein ND, Kweital A, McCaul KD, Magnan RE, Gerrard M, Gibbons FX. Risk perceptions: assessment and relationship to influenza vaccination. Health Psychol. 2007;26(2):146–151. doi: 10.1037/0278-6133.26.2.146. [DOI] [PubMed] [Google Scholar]
- 38.Institute of International Education. [February 10, 2012];Profile of U.S. Study Abroad Students, 1999/00-2009/10. Available at: http://www.iie.org/Research-and-Publications/Open-Doors/Data/US-Study-Abroad/Student-Profile/2000-10.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.