

Abstract
Objective
To assess the safety and efficiency of cell therapy for pseudarthrosis. Implant of the bone marrow aspirate was compared to mononuclear cells purified extemporaneously using the Sepax® equipment.
Methods
Six patients with nonunion of the tibia or femur were treated. Four received a percutaneous infusion of autologous bone marrow aspirated from the iliac crest, and two received autologous bone marrow mononuclear cells separated from the aspirate with the Sepax®. The primary fixation method was unchanged, and the nonunion focus was not exposed. Physical examination and radiographies were performed 2, 4 and 6 months after the treatment by the same physician. After consolidation of the fracture the satisfaction of the patients was estimated using the adapted QALY scale.
Results
No complications occurred as a result of the referred procedures. Bone consolidation was obtained in all cases within 3 to 24 weeks. The degree of patient satisfaction before and after bone consolidation was assessed, with the average value increasing from two to nine (p=0.0156).
Conclusion
We conclude that the proposed method is effective and safe for the treatment of nonunion of long bones regardless of the stabilization method used. Level of Evidence II, Prospective Comparative Study
Keywords: Pseudarthrosis, Bone marrow cells, Stem cells, Tibia, Femur, Fracture healing
INTRODUCTION
Despite new technological advances in the field of traumatological surgery, it is still challenging to treat a group of fractures that present alterations in the consolidation process and culminate in pseudarthrosis. It is estimated that approximately 5% of long bone fractures evolve into this dysfunction of the consolidation process.1
Autologous bone graft has been the most commonly used surgical technique for the treatment of this pathology. Spongy bone is used due to its high osteoinductive and osteoconductive potential, is more often removed from the iliac crest2 and continues to be the gold standard in comparison with any other type of bone graft or substitute. In spite of this, other technologies have been developed, such as the use of the bone morphogenetic protein (BMP)3 for spinal fusion.4 The main disadvantage of the autologous bone graft is the morbidity of the donor site, with a risk of complications such as pain, neurovascular lesions, fractures, bruising, infection, hernias, gait disorder, esthetic alterations, sacroiliac instability and urethral lesions.5,6
The bone marrow supplies mesenchymal cells and growth factors necessary for bone consolidation. The osteogenic capacity of the bone marrow was first demonstrated in rabbits in 1869, by Goujon.7 Percutaneous bone marrow aspirate grafting is a minimally invasive treatment, with proven effectiveness for the treatment of atrophic pseudarthrosis, with few reported complications.8-12
The evolution of medical devices applied to cell therapy for chronic and traumatic diseases has been evident in recent years. An example is the automated and closed system for the separation and the concentration of the fraction of mononuclear cells obtained from peripheral blood, from umbilical cord blood or from the bone marrow aspirate (Sepax®).13-15 Such a device aims maximize the therapeutic potential of adult progenitor cells, minimizing the human factor and increasing the reproducibility of the hematopoietic and mesenchymal progenitor cell isolation process. The infusion of autologous bone marrow aspirate for the treatment of pathologies such as aseptic necrosis of the femoral head and pseudarthrosis cases is being performed with considerable success, and its efficacy appears to be related to the concentration of progenitor cells in the graft. It was demonstrated that the bone marrow graft infusion with less than 1000 progenitor cells/cm3 did not result in consolidation and that a total of more than 30,000 progenitor cells are required for the therapy to prove successful.16-20
However, these researchers declare that they are unable to discover, based on the conclusions of their studies, whether the same number of cells in a larger volume and without concentration would be equally effective. Accordingly, the objective of this study was to analyze the safety and the efficacy of the technique of percutaneous infusion in the nonunion focus of the simple autologous bone marrow aspirate and of the aspirate infusion treated with the Sepax® mononuclear cell separation and concentration system.
METHODS
This trial was approved by the Institutional Review Board of the School of Medicine of Universidade Federal Fluminense under number 64/00. The survey subjects signed the Free Consent Form, authorizing their participation in the study.
Individuals over 18 years of age, with uninfected long-bone pseudarthrosis with space between the fragments of up to 10 millimeters in the plain radiographs in two views (anteroposterior and lateral), treated or not treated with some form of fixation, were included in the study.
Individuals presenting bone loss or diastasis greater than 10 millimeters, absence of cutaneous coverage of the fracture focus, angular deformity or shortening that would require treatment, patients with infection at the site or other comorbidities that would contraindicate the surgical procedure were excluded from the study.
Characteristics of the sample
Individuals (n=6) with pseudarthrosis of the femur and of the tibia, stabilized with the use of plaster cast, intramedullary nail or external fixation, were treated at Hospital Antônio Pedro da Universidade Federal Fluminense in the period between June 2008 and February 2009. The patients' age ranged from 21 to 59 years.
Five patients were male and one female. Three had a history of smoking, while none were diabetic or were using a pharmacological agent that would affect the bone metabolism. Five had the tibia and one had the femur as the bone involved. Among the cases of tibial pseudarthrosis, two were stabilized with external fixator, two with plaster cast and one did not present any type of fixation. This patient was walking with two crutches and without bearing weight on the affected limb. The femoral pseudarthrosis was stabilized with an intramedullary nail. Five patients presented pseudarthrosis resulting from exposed fracture. These were treated surgically, in the first 24 hours after the trauma, with mechanic surgical scrub, debridement and fracture fixation. The pseudarthrosis time ranged between 24 and 136 weeks (Tables 1 and 2). Four patients selected at random were submitted to the procedure with total bone marrow aspirate and injection in the nonunion focus (group I). Group II was also formed randomly by two patients where the total aspirate was processed in the Sepax® for the separation and the concentration of the mononuclear cells and subsequent injection in the nonunion focus. None of the patients knew which procedure would be carried out either on the day of surgery or in the postoperative follow-up period.
Table 1.
Group I: Simple bone marrow aspirate - profile of the patients and treatment satisfaction evaluation (QALY).
| Patient | Bone affected | Time with pseudoarthrosis (weeks) | Consolidation time (weeks) | Degree of satisfaction before surgery | Degree of satisfaction after surgery |
| Means: | 62 | 13.75 | 2.75 | 9 | |
| I | Femur | 56 | 24 | 5 | 8 |
| II | Tibia | 24 | 03 | 3 | 10 |
| IV | Tibia | 136 | 16 | 3 | 9 |
| V | Tibia | 32 | 12 | 0 | 9 |
Table 2.
Group II: Sepax - profile of the patients and treatment satisfaction evaluation (QALY).
| Patient | Bone affected | Time with pseudoarthrosis (weeks) | Consolidation time (weeks) | Degree of satisfaction before surgery | Degree of satisfaction after surgery |
| Means: | 68 | 14 | 1 | 8.5 | |
| Ill | Tibia | 68 | 16 | 0 | 8 |
| VI | Tibia | 68 | 12 | 2 | 9 |
Surgical technique
The technique used to harvest the aspirate was similar to that described for oncological and hematological procedures for bone marrow transplants.11,12 The patients were positioned in prone position after spinal anesthesia. A 11G X 10 cm bone marrow aspiration needle was introduced manually in the posterior iliac crest. The marrow was aspirated with a heparinized syringe up to a volume between 2 and 4 ml. (Figure 1) The needle was repositioned after each puncture to avoid the aspiration of venous blood. The aspirations were continued, using the same penetration in the skin or changing the site when necessary. The aspirated material was placed in a heparinized container. A quantity between 100 and 110 ml was obtained for each patient.
Figure 1.
Bone marrow aspiration technique.
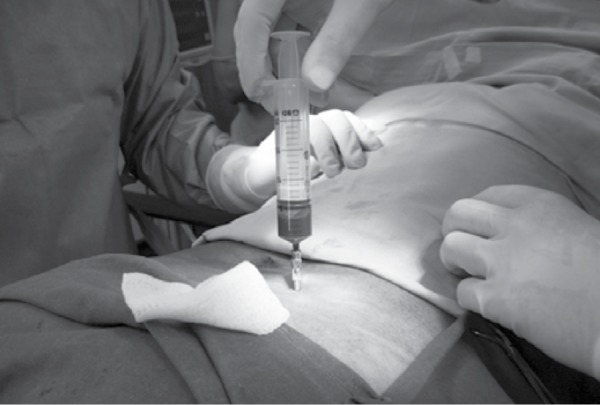
After the obtainment of the bone marrow material, a similar needle was positioned at the nonunion focus and its position was confirmed by image control. (Figure 2) The posterior region of the tibia and the lateral region of the femur were chosen for the grafting. In four patients the aspirate was injected in volumes of 15 to 20 ml at a time, until a total volume of 100 ml had been introduced into the nonunion focus. In another two patients, the total aspirate (100 ml) was processed in the Sepax® system for isolation and concentration of progenitor mononuclear cells and 20 ml was infused into the nonunion focus.
Figure 2.

Control by imaging of the bone marrow aspirate infusion.
The fracture focus was not exposed by access routes in any of the cases.
Evaluation of pseudarthrosis after the percutaneous grafting
All the patients were monitored using the same protocol during the postoperative period, through an interview, physical examination and radiographic evaluation performed 2, 4 and 6 months after the procedure by an orthopedic doctor who did not know which procedure had been executed (Groups I and II). The physical examination assessed pain, sensation of stability, and ability to walk with two, one or without crutches. The clinical criteria included full weight bearing tolerance and absence of pain upon palpation at the fracture site. The radiographic examination used anteroposterior, lateral and oblique views. Partial weight bearing was only allowed after the appearance of the bone callus and with signs of stability upon physical examination.
The treatment was considered successful when we observed the appearance of the bone callus upon radiographic examination, full stability upon clinical examination and absence of pain in walking with total load. Any side effects resulting from the procedure were assessed and recorded. The defined clinical protocol established that, if the patient did not present signs of bone consolidation six months after the procedure, a second intervention would be indicated, a situation considered a treatment failure.
In the interview held after the observation of bone consolidation, the patients were questioned about their level of satisfaction, comparing their affected limb before and after the procedure through numerical grading. We used a scale from 0 to 10, where 0 means minimum satisfaction and 10 represents maximum satisfaction. The means and standard deviations obtained, regardless of the treatment to which the patient was submitted, were submitted to the Wilcoxon matched-pairs signed-ranks test, considering the difference significant if p< 0.05.
RESULTS
None of the patients presented anesthetic complications. There was no drop in oxygen saturation, arrhythmia or change in blood pressure during the procedures. There were no cases of compartment syndrome after the injection of the bone marrow aspirate. None of the patients presented bruising or chronic pain at the injection site.
Bone consolidation was obtained in all the patients.
In Group I bone callus was observed in the radiographs between 3 and 24 weeks, averaging 13.8 weeks.
In Group II bone callus was observed in the radiographic examinations between 12 and 16 weeks averaging 14 weeks.
The mean patient satisfaction level rose from 2.75 to 9 in Group I and from 1 to 8.5 in Group II (Tables 1 and 2, p=0.0156 - Wilcoxon matched-pairs signed-ranks test).
DISCUSSION
The treatment of dysfunctions of the human skeleton consolidation mechanism constitutes an important challenge to the orthopedic surgeon. Bone marrow aspirated from the iliac crest and its infusion into the nonunion focus appears as a less invasive option for the treatment of this pathology. Healey, et al.,10 demonstrated pseudarthrosis remission in a previous study in 5 of 8 patients under critical circumstances (sarcoma resection and chemotherapy), after percutaneous infusion of bone marrow.
The present study confirms that the infusion of bone marrow aspirate, either total or processed in Sepax®, is a safe form of approach to the treatment of long bone pseudarthrosis, since no local or systemic complications were observed. A possible complication is allegedly pulmonary embolism during the injection of the crude bone marrow aspirate due to the injected volume and presence of fatty material. This complication was not observed when we injected larger volumes of bone marrow in the patients where the aspirate was not treated with Sepax®. This observation is also sustained by the observation of absence of fat embolism in cases of closed long bone fractures that have much greater potential for bleeding than the volume injected into the nonunion focus in the present study. Hernigou also demonstrated the safety of this procedure in the treatment of 60 atrophic tibial pseudarthroses in a previous study, not observing any cases of fat embolism.19 He attributes the absence of this complication to having filtered the bone marrow aspirate, separating and overlooking fat during the cell separation and concentration process. Of 60 patients treated, Hernigou obtained 53 cases of consolidation. He considers the correlation between the success of the treatment with the number of progenitor cells in the aspirate to be significant.20 It is worth mentioning that the mean obtained for the pure bone marrow aspirate ranges from 12 to 1224 progenitor cells/cm3. This variation depends essentially on the quantity of peripheral blood in the bone marrow aspirate, emphasizing the quality of aspiration procedure as critical for the success of the therapy.
In the present study we demonstrated the consolidation of pseudarthroses in all the cases, regardless of whether the Sepax® system was used or not. This result confirms the efficacy of the technique.9-12 The decrease in the volume injected by the Sepax® processing is important in procedures where the introduction of more than 100 ml of aspirate can be impeditive, as is the case of femoral neck necrosis therapy,21 in the bone repair of smaller patients or smaller size bones. Theoretically, as a disadvantage of this system, we encounter the fact that the injection of red blood cells with subsequent release of iron can be an adverse condition for cell proliferation, as observed in vitro.
In the pure bone marrow aspirate infusion method, the injection of granulocytes, eliminated in the Sepax® processing, can help in the prevention of osteomyelitis (preliminary observations, not published).
It is not yet possible to determine the exact mechanism of induction of bone callus formation by the aspirate infusion. Bone consolidation occurred even without the removal of the fibrous tissue interposed in the fracture, since no patient had the nonunion focus exposed by incision. In light of current knowledge it is possible to assume that the bone formation was due to the differentiation of the progenitor cells into active osteoblasts, resulting in the formation of bone matrix, and not to the differentiation of the fibrous tissue interposed at the nonunion focus in bone. Dense fibrous tissue can retain the injected cells and function as a three-dimensional framework for ossification. We also believe that the success of the treatment of the group I patients is due to the action of osteoinductive substances such as growth factors and to the inflammatory action caused by the red blood cells existing in the total bone marrow aspirate. This inflammatory action would have an influence on the biological reactivation of the bone consolidation process that was stagnated. We were also able to observe that the fracture stabilization method (plaster cast, intramedullary nail and external fixator) probably did not interfere in the end result, while the percutaneous infusion of the bone marrow aspirate was the only intervention performed. Hence the same fixation method, the infusion of autogenous cells, was maintained for each patient. Subsequent studies with a greater number of patients will be necessary to confirm this observation.
A very important aspect observed in this study was the considerable increase in the perception of the patients' quality of life, regardless of the treatment performed, reflecting the impact of this type of treatment on the quality of life of the individuals affected.
CONCLUSION
The percutaneous grafting of progenitor mesenchymal cells from the bone marrow is a safe and effective method for the treatment of long bone pseudarthrosis, capable of producing a significant improvement in the perception of the quality of life of affected patients. The results appear similar with the use of total aspirate and of the aspirate treated with Sepax® apparatus, regardless of the stabilization method used. It is a minimally invasive treatment option that presents an excellent alternative for the treatment of long bone pseudarthrosis.
Studies with a larger casuistry are the next step towards a better understanding of the limits and benefits of the techniques.
Acknowledgments
This study was partially funded by Grupo Vida, Belo Horizonte, Brazil, and Excellion Serviços Biomédicos, Petrópolis, Brazil, but without any influence on its execution and analysis. Drs. Radovan Borojevic and José Mauro Granjeiro were partially funded by the National Council for Scientific and Technological Development (CNPQ), Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (Cientista do Nosso Estado), the Department of Science and Technology of the Ministry of Health (DECIT/MS), Financiadora de Estudos e Projetos (FINEP).
We are especially grateful to Dr. Beatriz Guitton Renaud Baptista de Oliveira for her important contribution in this project.
Footnotes
All the authors declare that there is no potential conflict of interest referring to this article.
Study conducted at Hospital Universitário Antônio Pedro, UFF - Niterói, RJ. Brazil.
REFERENCES
- 1.Reis FB, Hubngria Neto JS, Pires RES. Pseudoartrose. Rev Bras Ortop. 2005;40(3):79–88. [Google Scholar]
- 2.Conway JD. Autograft and nonunions: morbidity with intramedullary bone graft versus iliac crest bone graft. Orthop Clin North Am. 2010;41(1):75–84. doi: 10.1016/j.ocl.2009.07.006. [DOI] [PubMed] [Google Scholar]
- 3.Granjeiro JM, Oliveira RC, Bustos-Valenzuela JC, Sogayar MC, Taga R. Bone morphogenetic proteins: from structure to clinical use. Braz J Med Biol Res. 2005;38(10):1463–73. doi: 10.1590/s0100-879x2005001000003. [DOI] [PubMed] [Google Scholar]
- 4.Papakostidis C, Kontakis G, Bhandari M, Giannoudis PV. Efficacy of autologous iliac crest bone graft and bone morphogenetic proteins for posterolateral fusion of lumbar spine: a meta-analysis of the results. Spine (Phila Pa 1976) 2008;33(19):E680–92. doi: 10.1097/BRS.0b013e3181844eca. [DOI] [PubMed] [Google Scholar]
- 5.Goulet JA, Senunas LE, DeSilva GL, Greenfield ML. Autogenous iliac crest bone graft. Complications and functional assessment. Clin Orthop Relat Res. 1997;(339):76–81. doi: 10.1097/00003086-199706000-00011. [DOI] [PubMed] [Google Scholar]
- 6.Kim DH, Rhim R, Li L, Martha J, Swaim BH, Banco RJ, et al. Prospective study of iliac crest bone graft harvest site pain and morbidity. Spine J. 2009;9(11):886–92. doi: 10.1016/j.spinee.2009.05.006. [DOI] [PubMed] [Google Scholar]
- 7.Goujon E. Recherches expérimentales sur lês propiétés physiologiques de La moelle des os. J Anat Physiol. 1869;6:399–412. (Fre). [Google Scholar]
- 8.Connolly J, Guse R, Lippiello L, Dehne R. Development of an osteogenic bone-marrow preparation. J Bone Joint Surg Am. 1989;71(5):684–91. [PubMed] [Google Scholar]
- 9.Connolly JF, Guse R, Tiedeman J, Dehne R. Autologous marrow injection as a substitute for operative grafting of tibial nonunions. Clin Orthop Relat Res. 1991;(266):259–70. [PubMed] [Google Scholar]
- 10.Healey JH, Zimmerman PA, McDonnell JM, Lane JM. Percutaneous bone marrow grafting of delayed union and nonunion in cancer patients. Clin Orthop Relat Res. 1990;(256):280–5. [PubMed] [Google Scholar]
- 11.Garg NK, Gaur S, Sharma S. Percutaneous autogenous bone marrow grafting in 20 cases of ununited fracture. Acta Orthop Scand. 1993;64(6):671–2. doi: 10.3109/17453679308994595. [DOI] [PubMed] [Google Scholar]
- 12.Paley D, Young MC, Wiley AM, Fornasier VL, Jackson RW. Percutaneous boné marrow grafting of fractures and bony defects. An experimental study in rabbits. Clin Orthop Relat Res. 1986;(208):300–12. [PubMed] [Google Scholar]
- 13.Aktas M, Radke TF, Strauer BE, Wernet P, Kogler G. Separation of adult bone marrow mononuclear cells using the automated closed separation system Sepax. Cytotherapy. 2008;10(2):203–11. doi: 10.1080/14653240701851324. [DOI] [PubMed] [Google Scholar]
- 14.Lapierre V, Pellegrini N, Bardey I, Malugani C, Saas P, Garnache F, et al. Maddens S. Cord blood volume reduction using an automated system (Sepax) vs. a semi-automated system (Optipress II) and a manual method (hydroxyethyl starch sedimentation) for routine cord blood banking: a comparative study. Cytotherapy. 2007;9(2):165–9. doi: 10.1080/14653240701196811. [DOI] [PubMed] [Google Scholar]
- 15.Rodríguez L, Azqueta C, Azzalin S, García J, Querol S. Washing of cord blood grafts after thawing: high cell recovery using an automated and closed system. Vox Sang. 2004;87(3):165–72. doi: 10.1111/j.1423-0410.2004.00550.x. [DOI] [PubMed] [Google Scholar]
- 16.Thomas ED. Bone marrow transplantation. In: Bach FJ, Good R, editors. Clinical immunobiology. New York: Academic Press; 1978. pp. 1–32. [Google Scholar]
- 17.Thomas ED, Storb R. Technique for human marrow grafting. Blood. 1970;36(4):507–15. [PubMed] [Google Scholar]
- 18.Faucett SC, Genuario JW, Tosteson AN, Koval KJ. Is prophylactic fixation a cost-effective method to prevent a future contralateral fragility hip fracture? J Orthop Trauma. 2010;24(2):65–74. doi: 10.1097/BOT.0b013e3181b01dce. [DOI] [PubMed] [Google Scholar]
- 19.Hernigou P, Mathieu G, Poignard A, Manicom O, Beaujean F, Rouard H. Percutaneous autologous bone-marrow grafting for nonunions. Surgical technique. Pt 2J Bone Joint Surg Am. 2006;88(Suppl 1):322–7. doi: 10.2106/JBJS.F.00203. [DOI] [PubMed] [Google Scholar]
- 20.Hernigou P, Poignard A, Beaujean F, Rouard H. Percutaneous autologous bone-marrow grafting for nonunions. Influence of the number and concentration of progenitor cells. J Bone Joint Surg Am. 2005;87(7):1430–7. doi: 10.2106/JBJS.D.02215. [DOI] [PubMed] [Google Scholar]
- 21.Daltro GC, Fortuna VA, Araujo MAS, Lessa PIF, Batista Sobrinho UA, Borojevic R. Tratamento de osteonecrose da cabeça femoral com células progenitoras autólogas em anemia falciforme. Acta Ortop Bras. 2008;16(1):23–8. [Google Scholar]