

Abstract
BACKGROUND/OBJECTIVES:
Coronary artery anomalies are present at birth, but relatively few are symptomatic. The majority are discovered incidentally. In the present study, coronary angiograms performed in the authors’ centre (Ondokuz Mayis University Hospital, Samsun, Turkey) were analyzed to determine the prevalence and types of coronary artery origin and course anomalies.
METHODS:
Coronary angiographic data of 16,573 patients were analyzed. Anomalous origins and courses of coronary arteries were assessed.
RESULTS:
Anomalous coronary arteries were detected in 48 (0.29%) of 16,573 patients. The origin of the circumflex (Cx) artery from the right coronary artery (RCA) or right sinus of Valsalva was the most common anomaly (28 patients [58.3%]). An anomalous RCA originating from the left anterior descending artery (LAD) or Cx artery was observed in six patients (12.5%). The left coronary artery originated from the right sinus of Valsalva in five patients, and the LAD originated from the RCA or the right sinus of Valsalva in five patients. The RCA originated from the left sinus of Valsalva in three patients and from an ectopic ostium in the ascending aorta in one patient.
CONCLUSIONS:
The most frequent anomaly observed in the present study was related to the Cx artery, which is consistent with previous reports. Although coronary artery anomalies are rare, they may cause difficulties during coronary interventions or cardiac surgery and may occasionally result in sudden cardiac death. Therefore, the recognition and diagnosis of these anomalies is important and requires specialization in coronary angiographic techniques and other imaging modalities.
Keywords: Coronary angiography, Coronary artery anomaly, Sinus of Valsalva
Coronary artery anomalies are a diverse group of congenital disorders, the manifestations and pathophysiological mechanisms of which are highly variable. They are present at birth, but relatively few are symptomatic. Although generally benign in character, some coronary artery anomalies are associated with more serious clinical outcomes such as congestive heart failure, arrhythmia, myocardial infarction, syncope and sudden death (1,2).
Coronary artery anomalies include abnormalities in the origin, course or structure of the epicardial coronary arteries. Most coronary artery anomalies are discovered incidentally during coronary angiography or autopsy. An anomalous origin of one or more coronary arteries has been detected in approximately 0.27% to 1.66% of patients undergoing coronary angiography, with a rate of 0.6% detected in autopsy series (2–11).
The recognition of these anomalies is of particular significance when a patient requires percutaneous coronary intervention or cardiac surgery. In the present study, we analyzed coronary angiograms to determine the frequency and types of coronary artery origination and course anomalies in our centre.
METHODS
All patients who underwent coronary angiography in the cardiac catheterization laboratories of Ondokuz Mayis University Hospital (Samsun, Turkey) from November 2001 to January 2011 were included. The coronary angiograms of 16,573 patients with symptomatic heart disease were analyzed and those with anomalous coronary arteries were selected for further assessment. Angiograms were reviewed by two independent experienced cardiologists who reached a consensus on the origin and course of the anomalous coronary arteries.
The anomalous origin and course of coronary arteries were assessed. The separate ostium of left anterior descending (LAD) and circumflex (Cx) arteries in the left sinus of Valsalva (LSV), separate origin of conus or right ventricular branch in the right sinus of Valsalva (RSV) and high ‘take-off’ of coronary arteries were not included in the anomalous coronary artery group. Patients with coronary anomalies occurring as a result of congenital heart disease were also not included in the present study.
RESULTS
Of the 16,573 patients (mean age 60 years; 11,273 male) who underwent coronary angiography, 48 patients (0.29%) had coronary arteries with anomalous origin and course (Table 1). The mean age of these 48 patients was 61.4 years and 33 (68%) were male. The indication for angiography was evaluation of coronary artery disease in all patients.
TABLE 1.
Prevalence of different coronary anomalies (n=48) in the patient population (n=16,573)
| Type of coronary anomaly | n | Anomaly prevalence, % | Prevalence among all patients, % |
|---|---|---|---|
| Anomalous origin of Cx artery from RCA/RSV | 28 | 58.3 | 0.169 |
| Anomalous origin of RCA from LAD or Cx artery | 6 | 12.5 | 0.036 |
| Anomalous origin of LCA from RSV | 5 | 10.4 | 0.030 |
| Anomalous origin of LAD from RCA/RSV | 5 | 10.4 | 0.030 |
| Anomalous origin of RCA from LSV | 3 | 6.3 | 0.018 |
| Anomalous origin of RCA from ectopic ostium in ascending aorta | 1 | 2.1 | 0.006 |
Cx Circumflex; LAD Left anterior descending; LSV Left sinus of Valsalva; RCA Right coronary artery; RSV Right sinus of Valsalva
The origin of the Cx artery from the right coronary artery (RCA) or RSV was the most common anomaly, present in 28 of 48 patients (58.3%), with an angiographic prevalence of 0.17% (Figure 1). The Cx artery originated from the RCA in 17 of these patients, and originated from a separate ostium in the RSV in 11 patients.
Figure 1).
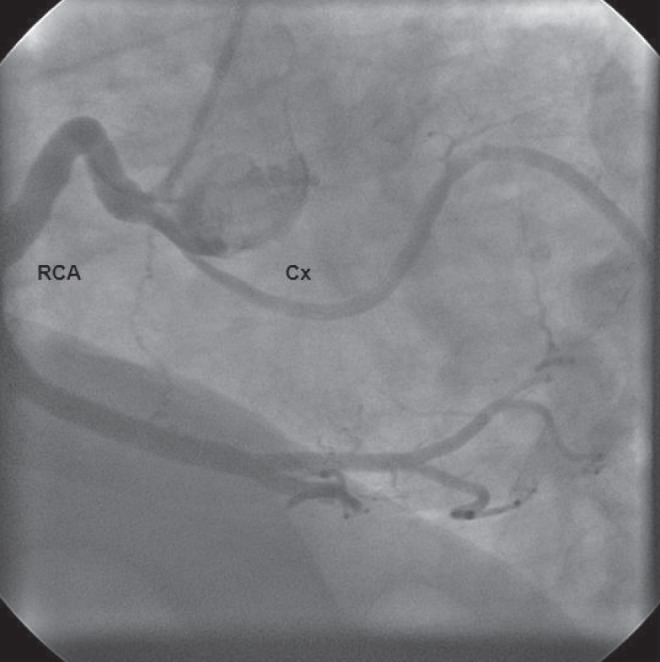
Left anterior oblique coronary angiographic view showing the circumflex (Cx) artery originating from the proximal portion of the right coronary artery (RCA)
An anomalous RCA originating from the LAD or Cx artery was observed in six of 48 patients (12.5%), with an angiographic prevalence of 0.04% (Figure 2). The RCA originated from the LAD in three patients (6.2%) and originated from the Cx artery in the remaining three patients (6.2%).
Figure 2).
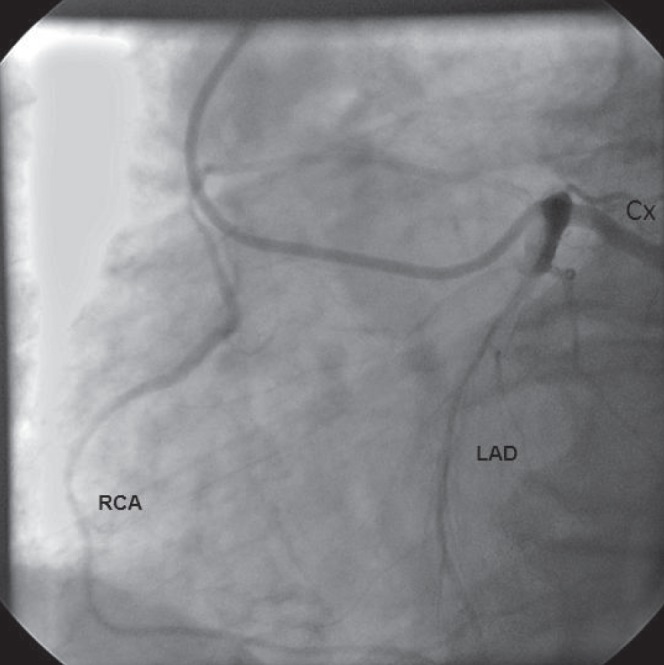
Left anterior oblique coronary angiographic view showing a single coronary artery in which the right coronary artery (RCA) originates from the proximal portion of the left anterior descending artery (LAD). Cx Circumflex
An anomalous left coronary artery (LCA) that originated from the RSV with a separate ostium was detected in five of 48 patients (10.4%), with an angiographic prevalence of 0.03%. The LAD originated from the RCA or RSV in five of 48 patients (10.4%) with an angiographic prevalence of 0.03%. The LAD originated from the RCA in four patients and originated from the RSV in only one patient.
The RCA originated from the LSV with a separate ostium in three of 48 patients (6.2%), with an angiographic prevalence of 0.01%. The RCA originated from an ectopic ostium in the ascending aorta in one patient (2.1%), with an angiographic prevalence of 0.006%.
DISCUSSION
In our series, coronary artery origin and course anomalies were found in 48 of 16,573 (0.29%) patients, which is consistent with the incidence of 0.27% to 1.66% reported in other series. The most common origin and course anomaly was the Cx artery originating from the RCA or RSV. This is also consistent with previously published series (2–10).
Different definitions have been proposed for coronary artery anomalies. Some authors prefer to categorize anomalies as ‘major’, ‘severe’, ‘important’ or ‘hemodynamically significant’ versus those that are ‘minor’. According to Angelini (1), the basic issue in the definition of a normal coronary artery is the normal spectrum of variation. Angelini proposed that, when possible, one should use quantifiable criteria such as “any form observed in more than 1% of an unselected general population is normal” (1). In accordance with this suggestion, we accepted the separate ostium of LAD and Cx arteries in the LSV and myocardial bridges as normal variants and did not include these entities in our list of coronary artery origin and course anomalies.
There are reports in the literature from different countries (Table 2). In some of these articles, the separate ostium of the LAD and Cx arteries in LSV was reported to be the most frequent coronary artery anomaly (3,4,7,8). We reviewed these reports and excluded this anomaly, and subsequently found that the most common coronary artery anomaly was the Cx artery originating from the RCA/RSV. According to the published data, of all coronary artery course and origin anomalies, the prevalence and angiographic prevalence of an anomalous origin of the Cx artery from the RCA/RSV were reported as 34.4% to 57.9% and 0.08% to 0.41%, respectively (3,4,8–10,12–15). In our report, we observed this anomaly in 58.3% of patients with anomalies and 0.17% of all angiographies. The RCA originating from the LSV or LAD was the second most common anomaly in the literature (4,5,7,16). Similarly, this anomaly was also the second most common coronary artery anomaly in our patients, present in 18.7% of patients with coronary anomalies.
TABLE 2.
The most frequent coronary artery origin and course anomalies reported in the literature, excluding a separate ostium of the left anterior descending artery (LAD) and circumflex (Cx) arteries in the left sinus of Valsalva (LSV)
| Author (reference), year | Type of coronary anomaly | n/n | Prevalence, % | Prevalence among all patients, % |
|---|---|---|---|---|
| Aydar et al (3), 2011 | Cx artery from RCS/RCA | 19/52 | 36.5 | 0.24 |
| Yildiz et al (4), 2010 | Cx artery from RCA/RSV or RCA from LSV | 10/29 | 34.4 | 0.08 |
| Ouali et al (5), 2009 | RCA from LSV/LAD | 10/20 | 50 | 0.13 |
| Aydinlar et al (7), 2005 | RCA from LSV/LAD | 22/57 | 38.5 | 0.18 |
| Correia et al (8), 2004 | Cx artery from RSV/RCA | 7/13 | 53.8 | 0.19 |
| Gol et al (9), 2002 | Cx artery from RSV/RCA | 99/173 | 57.2 | 0.17 |
| Pillai et al (10), 2000 | Cx artery from RSV/RCA | 34/53 | 64.1 | 0.29 |
| Click et al (12), 1989 | Cx artery from RSV/RCA | 44/76 | 57.9 | 0.17 |
| Eid et al (13), 2009 | Cx artery from RCS/RCA | 19/34 | 55.8 | 0.41 |
| Kardos et al (14),1997 | Cx artery from RSV/RCA | 28/44 | 63.6 | 0.36 |
| Tuccar and Elhan (15), 2002 | Cx artery from RSV/RCA | 12/25 | 48 | 0.24 |
| Garg et al (16), 2000 | RCA from LSV/NCSV | 19/35 | 54.2 | 0.46 |
NCSV Noncoronary sinus of Valsalva; RCS Right coronary sinus; RCA Right coronary artery; RSV Right sinus of Valsalva
There are reports of chest pain, myocardial infarction and sudden cardiac death related to coronary anomalies in the literature (17–21). Congenital coronary artery anomalies are frequently found to be responsible for sudden death in young athletes (in approximately 20% of cases) and represent the second most frequent disease responsible for athletic field deaths (22). The origin of the LCA from the contralateral sinus or artery with subsequent passage between the aorta and right ventricular outflow tract has been clearly shown to be a dangerous lesion. Other anomalies that can lead to these events include a single coronary artery, an anomalous coronary artery origin from a pulmonary artery, coronary artery fistula and atresia of the coronary ostium.
One of the clinically important coronary anomalies is the anomalous origin of the LCA from the RSV. The clinical fate of these patients depends on the course of LCA and its relation to the position of the aorta and pulmonary artery. An LCA that courses between the aorta and the pulmonary artery is associated with a high risk of sudden death in young men during exercise. The frequency of sudden death in patients with this anomaly is reported to be up to 80% (23).
Coronary angiography remains the gold standard in the diagnosis of coronary artery disease. However, advances in less invasive imaging techniques, especially those that can provide high resolution, such as computed tomography and cardiac magnetic resonance imaging, are becoming fundamental in the detection and diagnosis of coronary artery anomalies (24,25). In determining coronary artery origin and proximal course, cardiac magnetic resonance imaging may surpass conventional angiography and is the noninvasive method of choice, especially for patients with congenital defects (25). Therefore, the recognition and diagnosis of these anomalies is important and requires specialization in coronary angiographic techniques and other imaging modalities. Angiographic recognition of these vessels is critical because of their significance and clinical importance in patients undergoing coronary interventions or cardiac surgery.
CONCLUSION
We detected coronary artery origin and course anomalies in 48 of 16,573 patients (0.29%), with the most common anomaly being origin of the Cx artery from the RCA or RSV. Although coronary artery anomalies are rare, they may occasionally result in serious clinical situations such as sudden cardiac death. The recognition and diagnosis of these anomalies is important.
Acknowledgments
All authors appreciate the great effort of Mr Erdogan Yasar, the chief cardiac technician of the cardiac catheterization laboratories, in the conduction of this study.
REFERENCES
- 1.Angelini P. Coronary artery anomalies: An entity in search of an identity. Circulation. 2007;115:1296–305. doi: 10.1161/CIRCULATIONAHA.106.618082. [DOI] [PubMed] [Google Scholar]
- 2.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28–40. doi: 10.1002/ccd.1810210110. [DOI] [PubMed] [Google Scholar]
- 3.Aydar Y, Yazici HU, Birdane A, et al. Gender differences in the types and frequency of coronary artery anomalies. Tohoku J Exp Med. 2011;225:239–47. doi: 10.1620/tjem.225.239. [DOI] [PubMed] [Google Scholar]
- 4.Yildiz A, Okcun B, Peker T, Arslan C, Olcay A, Bulent VM. Prevalence of coronary artery anomalies in 12,457 adult patients who underwent coronary angiography. Clin Cardiol. 2010;33:E60–4. doi: 10.1002/clc.20588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ouali S, Neffeti E, Sendid K, Elghoul K, Remedi F, Boughzela E. Congenital anomalous aortic origins of the coronary arteries in adults: A Tunisian coronary arteriography study. Arch Cardiovasc Dis. 2009;102:201–8. doi: 10.1016/j.acvd.2009.01.001. [DOI] [PubMed] [Google Scholar]
- 6.Figueroa Y, Altieri PI, Banchs H, et al. Coronary artery abnormalities in Puerto Rico. P R Health Sci J. 2006;25:225–7. [PubMed] [Google Scholar]
- 7.Aydinlar A, Cicek D, Senturk T, et al. Primary congenital anomalies of the coronary arteries: A coronary arteriographic study in Western Turkey. Int Heart J. 2005;46:97–103. doi: 10.1536/ihj.46.97. [DOI] [PubMed] [Google Scholar]
- 8.Correia MJ, Faria JL, Cardoso PP, et al. Percentage of coronary anomalies in a population of patients undergoing coronary angiography: A retrospective study. Rev Port Cardiol. 2004;23:671–81. [PubMed] [Google Scholar]
- 9.Gol MK, Ozatik MA, Kunt A, et al. Coronary artery anomalies in adult patients. Med Sci Monit. 2002;8:CR636–CR641. [PubMed] [Google Scholar]
- 10.Pillai SB, Khan MM, Diamond A, McKeown PP. The prevalence and types of coronary artery anomalies in Northern Ireland. Ulster Med J. 2000;69:19–22. [PMC free article] [PubMed] [Google Scholar]
- 11.Drory Y, Turetz Y, Hiss Y, et al. Sudden unexpected death in persons less than 40 years of age. Am J Cardiol. 1991;68:1388–92. doi: 10.1016/0002-9149(91)90251-f. [DOI] [PubMed] [Google Scholar]
- 12.Click RL, Holmes DR, Jr, Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: Location, degree of atherosclerosis and effect on survival – a report from the Coronary Artery Surgery Study. J Am Coll Cardiol. 1989;13:531–7. doi: 10.1016/0735-1097(89)90588-3. [DOI] [PubMed] [Google Scholar]
- 13.Eid AH, Itani Z, Al-Tannir M, Sayegh S, Samaha A. Primary congenital anomalies of the coronary arteries and relation to atherosclerosis: An angiographic study in Lebanon. J Cardiothorac Surg. 2009;4:58. doi: 10.1186/1749-8090-4-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kardos A, Babai L, Rudas L, et al. Epidemiology of congenital coronary artery anomalies: A coronary arteriography study on a central European population. Cathet Cardiovasc Diagn. 1997;42:270–5. doi: 10.1002/(sici)1097-0304(199711)42:3<270::aid-ccd8>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 15.Tuccar E, Elhan A. Examination of coronary artery anomalies in an Adult Turkish population. Turk J Med Sci. 2002;32:309–12. [Google Scholar]
- 16.Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: A coronary arteriographic study. Int J Cardiol. 2000;74:39–46. doi: 10.1016/s0167-5273(00)00243-6. [DOI] [PubMed] [Google Scholar]
- 17.Prachar H, Muzika N, Dittel M, Kubiena K. Angina pectoris in coronary anomalies. Dtsch Med Wochenschr. 1991;116:496–8. doi: 10.1055/s-2008-1063639. [DOI] [PubMed] [Google Scholar]
- 18.Lipsett J, Byard RW, Carpenter BF, Jimenez CL, Bourne AJ. Anomalous coronary arteries arising from the aorta associated with sudden death in infancy and early childhood. An autopsy series. Arch Pathol Lab Med. 1991;115:770–3. [PubMed] [Google Scholar]
- 19.Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol. 1992;20:640–7. doi: 10.1016/0735-1097(92)90019-j. [DOI] [PubMed] [Google Scholar]
- 20.Kim HK, Choi YJ, Kang KW, Lee JA, Park SY, Zeon SJ. Successful primary percutaneous coronary intervention in a patient with acute myocardial infarction and single coronary artery ostium. Korean Circ J. 2012;42:284–7. doi: 10.4070/kcj.2012.42.4.284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Antunes N, Meireles A, Gomes C, et al. Anomalous origin of the right coronary artery and acute myocardial infarction: Cause or coincidence? Rev Port Cardiol. 2012;31:509–12. doi: 10.1016/j.repc.2011.11.013. [DOI] [PubMed] [Google Scholar]
- 22.Maron BJ, Shirani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO. Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA. 1996;276:199–204. [PubMed] [Google Scholar]
- 23.Andreini D, Mushtaq S, Pontone G, et al. Additional clinical role of 64-slice multidetector computed tomography in the evaluation of coronary artery variants and anomalies. Int J Cardiol. 2010;145:388–90. doi: 10.1016/j.ijcard.2010.02.057. [DOI] [PubMed] [Google Scholar]
- 24.Angelini P, Velasco JA, Flamm S. Coronary anomalies: Ancidence, pathophysiology, and clinical relevance. Circulation. 2002;105:2449–54. doi: 10.1161/01.cir.0000016175.49835.57. [DOI] [PubMed] [Google Scholar]
- 25.Post JC, van Rossum AC, Bronzwaer JG, et al. Magnetic resonance angiography of anomalous coronary arteries. A new gold standard for delineating the proximal course? Circulation. 1995;92:3163–71. doi: 10.1161/01.cir.92.11.3163. [DOI] [PubMed] [Google Scholar]