

Abstract
Keloids are benign growths characterized by excessive collagen formation. The treatment of keloid scars remains a challenging clinical dilemma for both patients and providers. Intralesional cryosurgery has emerged as a safe and effective new treatment by destroying the hypertrophic scar tissue with minimal damage to the skin surface.
Keloids are benign, dermal, fibroproliferative tumors characterized by excess collagen at the site of previous skin injury. Keloid scars extend beyond the borders of the original wound in contrast to hypertrophic scars, which are limited to the original wound site. Keloids often develop soon after injury, but can also occur up to several years following the initial traumatic insult.1
Keloid scars are well-demarcated, rubbery, mildly tender, bosselated tumors with a shiny surface, often marked by telangectasias and sometimes ulcerations. Lesions are pink to purple in color and may display hyperpigmentation. The most common anatomic sites include the anterior chest, shoulders, ear lobes, cheeks, and skin overlying joints. After development, keloid lesions continue to persist without spontaneous regression and have no malignant potential. Patients often complain of pruritis, pain, and hyperesthesia. These symptoms, along with the contractures from excessive scar formation, can be extremely uncomfortable for patients.2,3
A histological examination of a keloid reveals larger, thicker, and more disorganized collagen fibers than those seen in normal skin.1 They are pale-staining, hypocellular type I and III collagen bundles that lack nodules. Blood vessels are scattered and dilated, contributing to the poor vascularization in keloid scars. Special stains can detect the overproduction of fibronectin, an extracellular matrix protein.2
Excessive scar formation is due to abnormal wound healing following any injury to the deep dermis. Common causes include surgical procedures, piercings, vaccinations, lacerations, and burn injuries. Normal wound healing depends on the fine balance between extracellular matrix deposition and degradation.2 Over expression of fibroblast-specific growth factors has been implicated in the pathogenesis of keloids; these molecules include vascular endothelial growth factor (VEGF), transforming growth factor-beta (TGF-β), connective tissue growth factor (CTGF), and platelet-derived growth factor (PDGF). Additionally, keloid scars endure a longer inflammatory period compared to other scars, during which immune cells and pro-inflammatory cytokines continue to stimulate fibroblasts.2,3 Due to these aberrations and imbalances between the anabolic and catabolic phases of wound healing, there is exaggerated fibroblast activity and ultimately increased collagen synthesis.1,3
The likelihood of developing a keloid scar is multifactorial with a strong genetic component. There is potential for all individuals (except albinos) to develop keloid scars; however, the greatest incidence is observed in patients of darker skin color. Keloids are most common in the second to third decades of life, and susceptibility decreases with age.2,3
CURRENT THERAPIES
While multiple treatment modalities exist for treating keloid scars, no single method is proven to be widely effective. Intralesional corticosteroid injection (triamcinolone acetonide 10-40mg/mL) is the mainstay treatment method and is usually well tolerated by patients; however, approximately 50 percent of lesions recur after treatment.1,4 Another treatment, contact cryosurgery, has been demonstrated to be moderately effective as monotherapy, but patients may require up to 20 treatments.5-9 Contact cryosurgery, in combination with intralesional corticosteroid injections, is a common treatment regimen used in clinical practice.10
Scar revision procedures typically produce suboptimal results with recurrence rates between 45 to 100 percent.1 Laser and radiotherapy can be used with variable efficacy, in addition to intralesional injections with 5-fluorouracil (5-FU) or interferon-alfa-2b. Other minimally invasive regimens with limited efficacy include silicone gel sheets, silicone occlusive dressings, and pressure devices.4
INTRALESIONAL CRYOSURGERY AS A NOVEL TREATMENT
Intralesional cryosurgery, introduced in the early 1990s, is a treatment that allows for a focused destruction of keloid scar tissue with minimal surface damage to the epidermis.11 Delivery techniques and materials previously ranged from lumbar puncture needles to curved needles.12 Most recently, a uniquely designed intralesional cryosurgery needle probe has been developed. The probe is a long, uninsulated, double-lumen cryoneedle equipped with a sharp distal tip, cryogen vent, and adaptor to a cryogen source (Figures 1A and 1B).9
Figures 1A and 1B.


Intralesional cryosurgery device with probe and cryogen source. Photographs courtesy of Sascha Knopf
The entire procedure is conducted using universal sterile precautions. After obtaining adequate local anesthesia of the surgical site, the probe is inserted into the keloid scar by a gradual twisting motion until it penetrates the opposite end. A liquid nitrogen source is attached to the proximal end of the probe and the gas is passed through the needle until the keloid is sufficiently frozen by visual inspection, which typically takes 10 to 60 minutes, depending on scar volume (Figure 2). After allowing the scar to thaw for approximately 60 seconds, the probe is gently removed and the surgical site is dressed with an antibiotic ointment and sterile gauze.
Figure 2.

Intraoperative photograph of liquid nitrogen being passed through needle probe. Photograph courtesy of Z. Paul Lorenc, MD
The intralesional cryosurgery needle probe achieves destruction of keloid scars through direct cell anoxia due to the formation of intracellular ice crystals, which removes water from cells. In addition, the cold temperature damages endothelial cell junctions and causes blood stasis, thereby producing microthrombi, vascular injury, and ultimately, tissue necrosis.1 As liquid nitrogen passes through the needle, a lethal zone (<22°C) is created around the inserted probe in the dermis, thereby directly destroying the pathological cells.13 This is in contrast to traditional contact cryosurgery, which forms a lethal zone situated on the epidermis, often leading to unwarranted side effects and inadequate penetration to the deeper dermis (Figure 3).7,9
Figure 3.
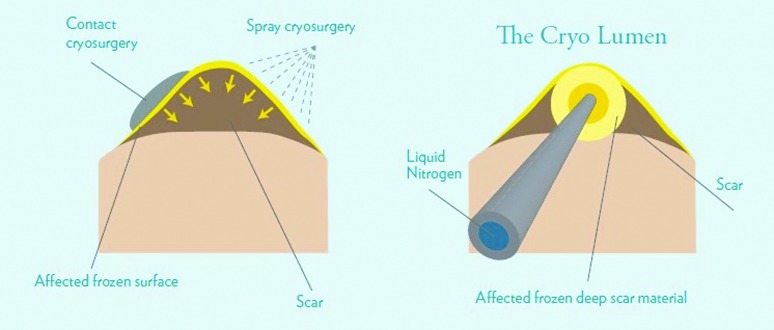
Illustration comparing mechanism of action of contact and intralesional cryosurgery. Photograph courtesy of Yaron Har-Shai, MD
Treating patients with intralesional cryosurgery transforms the scar architecture—the collagen fibers become more aligned in a parallel arrangement and the structure mimics normal, organized dermis.9 Treated keloids display a reduced number of proliferating cells, myofibroblasts, and mast cells.1
The typical clinical course after intralesional cryosurgery is initial peripheral erythema, followed by edema, bulla formation, exudation, crust formation, and subsequent healing with a flat, mildly atrophic scar after approximately one month. There are minimal side effects to the skin surface because the epidermis is spared from the freezing temperatures in the dermis. Hypopigmentation is the most common (91.7%) side effect after contact cryosurgery, but is rarely reported in intralesional methods because of increased melanocyte survival. Some patients report mild local edema and epidermolysis from the intralesional technique.9,13
Several studies9,14-17 have examined the safety and efficacy of intralesional cryosurgery as monotherapy for keloid scars. There is a significant reduction in objective parameters, such as scar volume, deformity, hardness, and redness, as well as subjective concerns including tenderness, itching, and aesthetic discomfort (Figures 4A-4D).15 Patients experience better results and shorter healing time compared to the contact cryosurgery technique.11
Figures 4A–4D.




Before and after photographs of patients treated with intralesional cryosurgery for keloid scars. Photographs courtesy of Yaron Har-Shai, MD
CONCLUSION
The treatment of keloid scars continues to be a challenging clinical scenario. Intralesional cryosurgery is shown to reduce the size of keloid scars and eliminate the symptoms associated with abnormal scar formation. Intralesional cryosurgery is a novel, safe, and highly efficacious technique recommended for clinicians and patients striving to minimize both the appearance and discomfort of these physically and psychologically damaging lesions.
Footnotes
DISCLOSURE:The authors report no relevant conflicts of interest.
REFERENCES
- 1.Har-Shai Y, Mettanes I, Zilberstein Y, et al. Keloid histopathology after intralesional cryosurgery treatment. J Eur Acad Dermatol Venereol. 2011;25(9):1027–1036. doi: 10.1111/j.1468-3083.2010.03911.x. [DOI] [PubMed] [Google Scholar]
- 2.Gauglitz GG, Korting HC, Pavicic T, et al. Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med. 2011;17(1-2):113–125. doi: 10.2119/molmed.2009.00153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Thomas DW, Hopkinson I, Harding KG, Shepherd JP. The pathogenesis of hypertrophic/keloid scarring. Int J Oral Maxillofac Surg. 1994;23(4):232–236. doi: 10.1016/s0901-5027(05)80377-7. [DOI] [PubMed] [Google Scholar]
- 4.Berman B, Zell D, Romagosa R. Keloid scarring. In: Lebwohl MG, Heymann WR, Berth-Jones J, Coulson I, editors. Treatment of Skin Disease Comprehensive Therapeutic Strategies. 2nd ed. Philadelphia, PA: Elsevier Limited; 2006. pp. 314–317. [Google Scholar]
- 5.Mende B. Treatment of keloids by cryotherapy. Z. Hautkr. 1987;62(18):1348,1351–1352,1355. [PubMed] [Google Scholar]
- 6.Zouboulis CC, Blume U, Buttner P, Orfanos CE. Outcomes of cryosurgery in keloids and hypertrophic scars: a prospective consecutive trial of case series. Arch Dermatol. 1993;129(9):1146–1151. [PubMed] [Google Scholar]
- 7.Rusciani L, Paradisi A, Alfano C, et al. Cryotherapy in the treatment of keloids. J Drugs Dermatol. 2006;5(7):591–595. [PubMed] [Google Scholar]
- 8.Rusciani L, Rossi G, Bono R. Use of cryotherapy in the treatment of keloids. J Dermatol Surg Oncol. 1993;19(6):529–534. doi: 10.1111/j.1524-4725.1993.tb00386.x. [DOI] [PubMed] [Google Scholar]
- 9.Har-Shai Y, Amar M, Sabo E. Intralesional cryotherapy for enhancing the involution of hypertrophic scars and keloids. PlastReconstrSurg. 2003;111(6):1841–1852. doi: 10.1097/01.PRS.0000056868.42679.05. [DOI] [PubMed] [Google Scholar]
- 10.Lawrence WT. In search of the optimal treatment of keloids: report of a series and a review of the literature. Ann Plast Surg. 1991;27(2):164–178. doi: 10.1097/00000637-199108000-00012. [DOI] [PubMed] [Google Scholar]
- 11.Weshahy AH. Intralesional cryosurgery. A new technique using cryoneedles. J Dermatol Surg Oncol. 1993;19(2):123–126. doi: 10.1111/j.1524-4725.1993.tb03440.x. [DOI] [PubMed] [Google Scholar]
- 12.Gupta S, Kumar B. Intralesional cryosurgery using lumbar puncture and/or hypodermic needles for large, bulky, recalcitrant keloids. Int J Dermatol. 2001;40(5):349–353. doi: 10.1046/j.1365-4362.2001.01117.x. [DOI] [PubMed] [Google Scholar]
- 13.Har-Shai Y, Dujovny E, Rohde E, Zouboulis CC. Effect of skin surface temperature on skin pigmentation during contact and intralesional cryosurgery of keloids. J Eur Acad Dermatol Venereol. 2007;21(2):191–198. doi: 10.1111/j.1468-3083.2006.01890.x. [DOI] [PubMed] [Google Scholar]
- 14.Har-Shai Y, Brown W, Pallua N, Zouboulis CC. Intralesional cryosurgery for the treatment of hypertrophic scars and keloids. Plast Reconstr Surg. 2010;126(5):1798–1800. doi: 10.1097/PRS.0b013e3181ef823d. [DOI] [PubMed] [Google Scholar]
- 15.Har-Shai Y, Brown W, Labbe D, et al. Intralesional cryosurgery for the treatment of hypertrophic scars and keloids following aesthetic surgery: the results of a prospective observational study. Int J Low Extrem Wounds. 2008;7(3):169–175. doi: 10.1177/1534734608322813. [DOI] [PubMed] [Google Scholar]
- 16.Har-Shai Y, Sabo E, Rohde E, et al. Intralesional cryosurgery enhances the involution of recalcitrant auricular keloids: a new clinical approach supported by experimental studies. Wound Repair Regen. 2006;14(1):18–27. doi: 10.1111/j.1743-6109.2005.00084.x. [DOI] [PubMed] [Google Scholar]
- 17.Mirmovich O, Gil T, Goldin I, et al. Pain evaluation and control during and following the treatment of hypertrophic scars and keloids by contact and intralesional cryosurgery—a preliminary study. J Eur Acad Dermatol Venereol. 2012;26(4):440–447. doi: 10.1111/j.1468-3083.2011.04092.x. [DOI] [PubMed] [Google Scholar]