

Abstract
Purpose
African American adolescent females tend to initiate participation in sexual activity at an earlier age than Caucasian adolescent females. Early initial participation in sexual activity is associated with increased HIV risk. However, limited prospective data are available on the rate at which African American adolescent females delay their initial participation in sexual activity. The purpose is to determine low-income inner city African American adolescent females' survival or continued non-participation in sexual activity over a 20-month period and to determine predictors associated with survival.
Methods
A longitudinal quasi-experimental research design with multiple data collection points was used. The convenience sample consisted of 396 African American females with a mean age of 12.4 years (SD = 1.1 years) and their mothers. The adolescents completed questionnaires assessing perceptions of maternal monitoring, HIV transmission knowledge, self-efficacy to refuse sex, intention to refuse sex, and age. Their mothers completed questionnaires assessing perception of maternal monitoring, safer sex self-efficacy, marital status, and educational level. At baseline, the adolescents reported non-participation in sexual activity. Survival analysis was conducted to determine the timing and predictors of sexual activity initiation for these adolescents.
Findings
Of the 396 adolescents, 28.5% did not survive; they participated in sexual activity within the 20-month period. Predictors of non-survival were the adolescents' age, perception of maternal monitoring, and intention to refuse sex.
Conclusion
Findings suggest interventions that increase maternal monitoring and adolescents' intentions to refuse sex could be beneficial in delaying sexual activity.
Introduction and Background
African American females accounted for 73% of the females between ages 13 and 19 who were HIV infected (Centers for Disease Control and Prevention [CDC], 2006). These infections were primarily transmitted through heterosexual contact (henceforth sexual activity) (CDC). Compared to 3% of Caucasian females, 7% of African American females initiate or have their first sexual activity before their 13th birthday (Grunbaum et al., 2004; Eaton et al., 2008). Initiating sexual activity before age 13 has been associated with increased risk for contracting HIV (Hall, Song, & McKenna, 2003). Sexual activity is having vaginal, anal, and/or oral sexual intercourse.
The integration of Bandura's social cognitive theory (1982) and Fishbein and Ajzen's theory of reasoned action (1975) suggests the importance of person and environmental variables in explaining the timing of initiation of sexual activity. Both theories propose that behavior is influenced by a reciprocal relationship between the person and her environment. Person variables associated with initiation of sexual activity are the adolescent female's HIV transmission knowledge, self-efficacy or confidence in her ability to refuse sex, intention or plans to refuse sex, perception of maternal monitoring, and age. The environmental variables include residing in a single parent home, and the mother's educational level, perception of maternal monitoring and safer sex self-efficacy or confidence in her ability to practice safer sex. The adolescent's intention to refuse sex has a direct, negative effect on initiation of sexual activity and is a function of HIV transmission knowledge, self-efficacy to refuse sex, perception of maternal monitoring, age and the environmental variables. HIV transmission knowledge, self-efficacy to refuse sex, perception of maternal monitoring, age and the environmental variables have indirect effects on sexual initiation through intention to refuse sex.
HIV transmission knowledge, self-efficacy to refuse sex, perception of maternal monitoring, age and the environmental variables can support or undermine intention to refuse sex as indicated by the following longitudinal empirical evidence. HIV transmission knowledge and self-efficacy to refuse sex was positively associated with intention to refuse sex for African American adolescent females (Dancy, Crittenden, & Talashek, 2006). Intention to refuse sex was positively associated with sexual abstinence for African American adolescent females (Dancy et al.; O'Donnell, Myint-U, O' Donnell, & Stueve, 2003; Stanton et al., 1996) and intention to participate in sexual activity was positively associated with participation in sexual activity for African American adolescents (O'Donnell, O'Donnell, & Stueve, 2001), South African adolescents (Mathews et al., 2009), and a mixed sample of Caucasian, African American, Latino and Asian adolescents (Kinsman, Romer, Furstenberg, & Schwartz, 1998). Additionally in their cross-sectional study, Dancy, Crittenden, and Freels (2006) found a positive association between self-efficacy to refuse sex and sexual abstinence for African American adolescent females.
Both cross-sectional (Dancy, Crittenden, & Freels; 2006) and longitudinal research (Dancy, Crittenden, & Talashek, 2006; Mathews et al., 2008; Whitbeck, Yoder, Hoyt, & Conger, 1999) revealed that African American adolescent females (Dancy, Crittenden, & Talashek), South African adolescents (Mathews), and Caucasian adolescents (Whitbeck et al.,) were more likely to participate in sexual activity as they grew older and that their intention to participate in sexual activity was positively associated with their growing older (Mathews et al.; Dancy, Crittenden, Freels). However, African American adolescent females' intention to refuse sex was positively associated with a reduction in their participation in sexual activity regardless of their growing older (Dancy, Crittenden, & Freels). Lastly consistent with longitudinal research (Mandara, Murray, & Bangi, 2003; Rosenthal et al., 2001), Dancy, Crittenden, and Freels' cross-sectional research found that African American adolescent females' perceptions of maternal monitoring was negatively associated with their likelihood of having participated in sexual activity. Other longitudinal studies found similar results for African American adolescent males (Mandara et al.), Caucasian adolescent females (Rosenthal et al.; Whitbeck et al), and Caucasian adolescent males (Whitbeck et al.).
The mother's effectiveness as a model and guide for her daughter's behavior may be enhanced by her own safer-sex self-efficacy, but may be hindered by her socioeconomic status, being a single parent or having low education. Low socioeconomic status, single parenthood, and mothers' education have been associated with timing of sexual initiation. Low socioeconomic status was positively associated with early participation in sexual activity for African American and South African adolescents (Mathews et al., 2009). Both cross-sectional (Felton & Bartoces, 2002) and longitudinal research (Whitbeck, Yoder, Hoyt, & Conger, 1999; Wu & Thomson, 2001) indicated that residing in a single-parent home was positively associated with early participation in sexual activity for Caucasian adolescent males and females (Whitbeck et al.) and for African American females (Felton & Bartoces; Wu & Thomson). However, Wu and Thomson found no association between residing in a single parent home and sexual initiation for Caucasian adolescent females. Lastly, Felton and Bartoces found no association between African American and Caucasian adolescent females' sexual initiation and their mothers' educational level.
Few studies have used multiple data collection points prospectively to discern the timing of sexual activity for African American adolescent females. A prospective approach with multiple data collection points will provide less ambiguity about the timing of and predictors (Burns & Grove, 2001) associated with sexual initiation for this at-risk population. Health care providers can use this information to tailor interventions at the critical time when African American adolescent females are likely to initiate sexual activity.
In the only prospective study found for African American females, McBride, Paikoff, and Holmbeck (2003) disclosed that 11.7% of their sample of low-income African American adolescent females initiated sexual activity over a two and a half year period. These adolescent females, with an average age of 11 years at baseline, provided data on their sexual activity at two time points: baseline and two and a half years later. With only two data collection points, it is difficult to pin down the timing of sexual initiation for these girls.
More data have been available on sexual initiation for other ethnic groups. However, these studies have typically collected data at a single point or separated by long intervals, making it difficulty to discern the timing of sexual initiation. Meier (2003), Mcneely et al. (2002), Whitbeck, Yoder, Hoyt, and Conger (1999) focused predominately on a Caucasian adolescent population to determine the rate of sexual initiation. Meier and Mcneely et al. collected data at baseline and a year later. Whitbeck et al. collected data at baseline and yearly for two years. At baseline, Meier's sample of males and females were between the ages of 15 and 18 years, Mcneely's et al. sample of females were 14 and 15 years, and Whitbeck's et al. sample of males and females were in the 8th grade. Over a 12 month period, 19% (Meier) and 15.8% (Mcneely et al.) of the adolescents experienced their first sexual activity. Over a 24 month period, 26% (Whitbeck et al.) initiated their first sexual activity. Mitchell et al. (2007) used a combination of retrospective and prospective data to assess annually over a seven year period the rate of sexual initiation for American Indian adolescents between 14 and 18 years at baseline. They found that the average age for first sexual activity was 15.1 years.
Purpose
The purpose was to determine survival or continued non-participation in sexual activity over a 20-month period for low-income inner city African American adolescent females who ranged in age from 11 to 14 years and who had not yet participated in sexual activity. The specific research questions were: 1) how long did these adolescents delay participation in sexual activity and 2) what predictors were associated with the timing of their initiation in sexual activity? The dependent variable for this survival analysis was self-reported participation in sexual activity collected at four time points over a 20-month period, which allowed the discernment of the time of initiation of sexual activity prospectively. The predictors of survival were the adolescent female's HIV transmission knowledge, self-efficacy to refuse sex, intention to refuse sex, perception of maternal monitoring, and age; her mother's perception of maternal monitoring, safer sex self-efficacy, marital status, and educational level; and the participation in an HIV risk reduction program.
Methods
Research Design and Study Setting
The sample came from a larger study described in Dancy, Crittenden, and Talashek (2006) that used a longitudinal quasi-experimental comparison group design of three intervention groups. The Mother/Daughter HIV risk reduction (MDRR) intervention (Dancy et al.), grounded in social cognitive theory and the theory of reasoned action, was a 6-week group skill-building program designed to increase adolescent females' self-efficacy and intention to refuse sex, delay in participation in sexual initiation and, if sexually active, to increase intention to use condoms and condom use. In the MDRR intervention, mothers were taught to deliver the HIV risk reduction content to their daughters. The MDRR intervention was compared to two control groups: the Health Expert HIV Risk Reduction (HERR) intervention where the HIV risk reduction content was delivered by the research staff and the Mother/Daughter Health Promotion (MDHP) intervention where mothers were taught to deliver content related to healthy eating and exercise to their daughters (Dancy et al.).
The study took place in poor African American communities in the Chicago metropolitan area. In these communities, 66% to 81% of the residents had income below the poverty line and 64% to 89% of the households were headed by females (City of Chicago Department of Public Health [CDPH], 2000a & b). The three communities ranked in the highest quintile of Chicago communities in AIDS prevalence (CDPH, 2000b). Since 2000, the Chicago prevalence rate for HIV infection has consistently been highest among African Americans; 56.9% of all HIV infected individuals were African Americans (Chicago Department of Public Health, 2008).
Sample
The convenience sample for this study consisted of 526 African American adolescents who met these selection criteria at baseline: aged 11 to 14 years, residing with their mothers, and their mothers reporting income below the federal poverty line (Dancy, Crittenden, & Talashek, 2006). Mothers were defined as legal guardians that included biological mothers, grandmothers, and adopted mothers. Of the 526 adolescents, 47 (8.9 %) reported at baseline (T1) that they had participated in sexual activity and were eliminated from the analysis. Eighty-three (17.3%) of the remaining 479 adolescents were lost to follow-up at the immediate post test (T2), resulting in a sample of 396 adolescents for whom we tracked survival. Attrition was due to participants moving and to lack of interest. Using t-tests and chi-square tests, we compared adolescents and mothers who were lost to follow up at T2 with those remaining in the study at T2. The tests showed no significant differences on demographic characteristics, except in education completed by the mothers. Mothers lost to follow-up were more likely to report trade school or an associate degree; those continuing in the panel were more likely to report high school or GED. Given that trade school might or might not have required high school or equivalent as a prerequisite, we did not deem this as an important difference between the two groups. See Table 1.
Table 1. Descriptive characteristics comparison (Subjects in panel at T2 versus lost to T2 follow-up).
| African American adolescent females | Subjects at T2 (N=396) |
T1 Subjects Lost to T2 Follow-up (N=83) |
P |
|---|---|---|---|
|
| |||
| Age at T1 | (Base = 396) | (Base=83) | |
| Range | 11 to 14 years | 11 to 14 years | N.S.b |
| Mean (SD) | 12.4 (1.1) | 12.3 (1.1) | |
|
| |||
| Grade level at T1 | (Base=396) | (Base=83) | |
| Range | 4th to 10th | 4th to 9th | N.S.b |
| Mean (SD) | 6.6 (1.2) | 6.6 (1.1) | |
|
| |||
| Grade earned at T1 -- % | (Base=391) | (Base=82) | |
| As | 29.4 | 24.4 | N.S.c |
| Bs | 45.5 | 43.9 | |
| Cs | 22.0 | 29.3 | |
| Ds | 2.3 | 1.2 | |
| Fs | 0.8 | 1.2 | |
|
| |||
| Mothers | (N=396) | (N=83) | |
|
| |||
| Age at T1 | (Base=396) | (Base=83) | N.S.b |
| Range | 22 to 75 year | 22 to 76 year | |
| Mean (SD) | 40.4 (10.2) | 39.1 (10.7) | |
|
| |||
| Number of Children at T1 | (Base=396) | Base=83) | |
| Range | 1-14 | 1-12 | N.S.b |
| Mean (SD) | 3.6 (2.2) | 4.0 (2.4) | |
|
| |||
| Marital Status at T1 -- % | (Base=396) | (Base=83) | |
| Married | 24.6 | 16.9 | N.S.c |
| Never Married | 45.3 | 59.0 | |
| Separated/Divorce | 22.3 | 16.9 | |
| Widowed | 7.6 | 7.2 | |
| Missing | 0.2 | 0.0 | |
|
| |||
| Highest Grade Completed at T1 -- % | (Base=395) | (Base=83) | |
| Less than 12th grade | 19.8 | 19.3 | <0.05c |
| Completed 12th or GED | 38.3 | 28.9 | |
| Trade School | 29.2 | 33.7 | |
| Associated Degree | 7.1 | 14.5 | |
| Bachelor | 2.5 | 2.4 | |
| Master | 3.1 | 1.2 | |
|
| |||
| Employment at T1 | (Base=389) | (Base=79) | |
| Employed Full or Part Time -- % | 54.2 | 51.9 | N.S.c |
|
| |||
| Monthly Income at T1 -- % | (Base=362) | (Base=81) | |
| Less than $500.00 | 27.6 | 29.6 | N.S.c |
| $500.00 - $1,499.00 | 53.0 | 52.1 | |
| $1,500.00 or more | 19.4 | 18.3 | |
|
| |||
| Receiving Welfare Assistance at T1 --%a | (Base=396) | (Base=83) | c |
| Public Aid or TANF | 13.2 | 13.1 | N.S. |
| Food Stamps | 48.3 | 54.2 | N.S. |
| Disability or SSI | 18.7 | 19.3 | N.S. |
| Social Security | 12.4 | 14.5 | N.S. |
| Unemployment Benefits | 5.8 | 7.2 | N.S. |
| Medicaid | 39.7 | 48.2 | N.S. |
| Medicare | 27.8 | 27.7 | N.S. |
| None | 30.8 | 28.9 | N.S. |
|
| |||
| Group Assignment for Mothers and Daughters | (Base 396) | (Base 83) | |
| MDRR | 32.1 | 31.3 | |
| MDHP | 33.6 | 42.2 | N.S. |
| HERR | 34.3 | 26.5 | |
Overlapping percentages will not sum to 100.
Two-tailed t-test.
Chi-square test.
Procedure
The University of Illinois at Chicago Office for Protection of Research Subjects approved this research project. Written consent and permission for participation in research was obtained from each mother and written assent to participate was obtained from each adolescent. Survival was tracked from the immediate post test (T2) until 20-months from baseline (T1) with data collected approximately every six months (T3 to T5). To afford maximal privacy, the Adolescent Questionnaire and the Mother Questionnaire, presented below, were conducted at each of the five time points with the audio computer-assisted self interview (A-CASI). Adolescents and their mothers were recruited over a two year period between 2002 and 2004 and data were collected between 2002 and 2007.
Instruments
The Adolescent Questionnaire consists of several scales: maternal monitoring, HIV transmission knowledge, self-efficacy to refuse sex, and intention to refuse sex. The questionnaire also has a single reported sexual item and a series of adolescent demographic questions. The Mother Questionnaire includes the maternal monitoring scale, the safer sex self-efficacy scale, and the mother demographic questions. The Adolescent and the Mother Questionnaires have been described extensively in previous publications (Dancy, Crittenden, & Talashek, 2006; Dancy, Crittenden, & Freels, 2006) and will be briefly covered below.
The maternal monitoring scale
The maternal monitoring scale (Steinberg, Lamborn, Dornbusch, & Darling, 1992; Steinberg, Lamborn, Darling, Mounts, & Dornbusch, 1994) with a Cronbach's alpha of 0.78 measures the adolescent's perceptions of how much her mother knows and tries to know what she does and where she is at night and after school. Its six items have a 3-point Likert format: mother doesn't know, knows a little, knows a lot; or mother doesn't try, tries a little, and tries a lot. It is computed as a rounded mean of the six items. Because it is highly skewed, we dichotomize the scale as a lot (=1) versus a little or less (=0).
The HIV transmission knowledge scale
The HIV transmission knowledge scale assesses awareness of the likelihood of acquiring HIV transmission through different types of behaviors, for example, sex with multiple partners, sex with someone with HIV, and using drug. It consists of seven items with a 4-point Likert format: very likely, somewhat likely, somewhat unlikely, and very unlikely. These items are summed and scored from most correct (4) to least correct (1). Its Cronbach's alpha is 0.84.
The self-efficacy to refuse sex scale
The self-efficacy to refuse sex scale (Stanton et al., 1995), has two dichotomous agree/disagree items that assess the adolescent's confidence in her ability to say no to sex. Its Kuder-Richardson reliability is 0.61.
The intention to refuse sex scale
The intention to refuse sex scale measures the adolescent's plans to decide not to have sex and to stick to her decision to say no to sex using four dichotomous agree/disagree items. It is a count of agree responses and its Kuder-Richardson reliability is 0.85.
Sexual activity
A single self-reported sexual participation item asks, “Have you had vaginal, anal and/or oral sex?” A value of 1 is assigned to yes responses and a value of 0 is assigned to no responses. To assure that the adolescents understand what information is being requested, the question is followed by these definitions of vaginal, anal, and oral sex. Vaginal sex is the boy's private part enters the girl's private part; anal sex is the boy's private parts enters the girl's butt, and oral sex is the girl's mouth touches the boy's private part or butt or the boy's mouth touches the girl's private part or butt. This single item provides a broad assessment of all three types of sexual intercourses, which is imperative given that all or any one of these types can enhance risk for sexually transmitted illnesses. Demographic questions ask information about the adolescent's age, grade level, and grade earned.
The Mother Questionnaire includes the maternal monitoring scale, the safer sex self-efficacy scale, and demographic questions. The maternal monitoring scale assesses the mother's perception of how much she knows and tries to know what her daughter does and where her daughter is at night and after school. It has the same number of items and is scored similarly to the adolescent's maternal monitoring scale. The Cronbach's alpha is 0.84.
The safer sex self-efficacy scale
The safer sex self-efficacy scale consists of three dichotomous (yes/no) items reflecting her own confidence in her ability to refuse unprotected sex, to decide not to have sex without a condom, and to stick with such a decision. The Kuder-Richardson reliability for the scale is 0.86.
Demographic questions ask about the mother's age, highest grade completed, employment status, monthly income, receipt of welfare assistance, marital status, and number of children. All mothers, except those mothers of adolescents in the HERR control group, that was taught by the research staff, complete the Mother questionnaire at each time point. The mothers of adolescents in the HERR group complete only the demographic questions at T1.
Analysis of Data
In the equation for predicting survival, intervention group assignment was represented by two dummy variables. The demographic predictors assessed at T1 were adolescents' age and mothers' marital status (currently married versus not married) and educational level (high school or equivalent versus less than high school). We subtracted adolescents' actual age at T1 in months from age in months at subsequent data collection points to determine the time elapsed in months for the survival curve. All scale predictor variables were assessed at T2. These predictor variables included adolescents' perception of maternal monitoring, HIV transmission knowledge, self-efficacy to refuse sex, and intention to refuse sex and mothers' perception of maternal monitoring and safer sex self-efficacy. The mother's maternal monitoring scale and the safer sex self-efficacy scale served as predictors in the survival analysis for mothers in the MDRR and MDHP interventions. Also, intervention group assignment represented by two dummy variables was used as a predictor of survival.
First we determined the trajectory of survival probabilities over time. Then we estimated proportional hazard models with Cox regression to determine the predictors for this trajectory (Collett, 1999; Kleinbaum, 1996). We introduced the predictors in three blocks representing causal order according to the theoretical perspective, to generate three models for survival during the 20-months from baseline. Predictors in earlier blocks might influence those in later blocks, but not vice versa. The first model included as predictors the adolescent's age at T1, the mother's marital status and education, and intervention assignment. It was estimated after testing for the viability of the proportional hazard assumption. The second equation added the adolescent's perception of maternal monitoring, HIV transmission knowledge and self-efficacy to refuse sex, and the mother's report of maternal monitoring and safer sex self efficacy. The third equation added the adolescent's reported intention to refuse sex.
Initially we generated two sets of preliminary models. For the entire sample, the second and third models included only scales for the adolescent. Then, limiting the analysis to the participants in the mother-daughter interventions, we repeated the models to include in the second and third models the scales for the mother. Lastly, we generated final models that included only those predictors with p-values for coefficients <0.05.
Results
At baseline, the 396 adolescents ranged in age from 11 to 14 years with a mean age of 12.4 years (SD = 1.1) and had a mean grade level of 6.6 (SD = 1.2) with a range of 4th to 10th grade. Mothers ranged in age from 22 to 76 years with a mean age of 40.4 years (SD = 10.2) and 24.6% reported being married. Nearly 20% had less than a high school education and approximately 80% reported a monthly income of less than $1,500. Please see Table 1 for additional demographic characteristics. Descriptive data for each scale predictor are presented in Table 2.
Table 2. Ranges and means of scale predictor variables at T2.
| African American adolescent females | |
|---|---|
|
| |
| HIV transmission knowledge | |
| Range | 7 to 28 |
| Mean (SD) | 22.8 (5.3) |
|
| |
| Perception of maternal monitoring | |
| Range | 0 to 1 |
| Mean (SD) | 0.83 (0.4) |
|
| |
| Self-efficacy to refuse sex | |
| Range | 0 to 2 |
| Mean (SD) | 1.5 (0.7) |
|
| |
| Intention to refuse sex | |
| Range | 0 to 4 |
| Mean (SD) | 3.2 (1.3) |
|
| |
| Mothers | |
|
| |
| Maternal monitoring scale | |
| Range | 2 to 3 |
| Mean (SD) | 2.9 (0.2) |
|
| |
| Safer sex self-efficacy scale | |
| Range | 0 to 6 |
| Mean (SD) | 4.8 (1.9) |
Survival, Non-Initiation of Sexual Activity
The majority of the adolescents in the sample survived the 20-month period without initiating sexual activity. Of the 396 adolescents who had not initiated sexual activity at baseline, 28.5% (n=113) did so within 20 months. Figure 1, panel A, shows the steadily decreasing probability of survival over the 20-month period.
Figure 1.
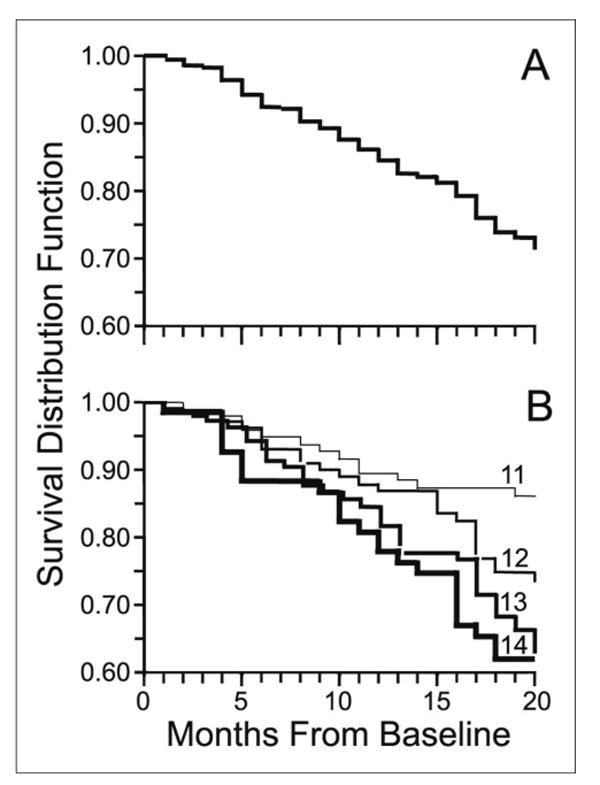
Distribution of survival from sex initiation over 20 months for African American adolescent females (product-limit estimate curve). Panel A: Survival probabilities for the entire sample (N=396). Panel B: Survival probabilities by age at T1.
Predictors of Survival, Non-Initiation of Sexual Activity
Table 3 shows the significant predictors in the three models for survival during the 20-month period. Because no environmental variables predicted survival, only the models for the entire sample are presented. Intervention assignment also did predict survival. The age of the adolescent was the strongest predictor of survival in model 1 and was the strongest predictor in all the models. The younger the adolescent was at baseline, the greater her probability of not initiating sexual activity. Non-survival increased with adolescent's age. By the end of the 20 months, 39% of the 14-year-old adolescents had participated in sexual activity, compared to 14% of 11-year-olds, 27% of 12-year-olds, and 37% of 13 year-olds. See Table 4 for the survival distribution for each time point by adolescent's initial age. Initiating sexual activity started between three and nine months and continued through 20 months. The adolescent's perception that her mother monitored her activities was a significant predictor in models 2 and 3. Adolescents who perceived more maternal monitoring survived longer without initiating sexual activity. The adolescent's HIV transmission knowledge and self-efficacy to refuse sex did not predict survival, but her intention to refuse sex at T2 was positively related to survival. Figure 1, panel B, displays the survival distributions by the adolescent's initial age.
Table 3. Cox proportional regression models for African American adolescent females' sex initiation within 20 months (N=396).
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Predictors | OR (95% CI) | P* | OR (95% CI) | P | OR (95% CI) | P |
| African American adolescent females' age (T1) | 1.44 (1.20, 1.74) | <.01 | 1.47 (1.22, 1.78) | <.01 | 1.45 (1.20, 1.76) | <.01 |
| African American adolescent females' perception of maternal monitoring (T2) | 0.55 (0.36, 0.83) | <.01 | 0.59 (0.38, 0.89) | <.05 | ||
| African American adolescent females' intention to refuse sex (T2) | 0.82 (0.72, 0.94) | <.01 | ||||
Two-tailed P values
Table 4. The survival probability of African American adolescent females not having sex within 20 months by months (time point) and initial age group.
| Time interval in Months (Time point) | Age11 (N=104) | Age12 (N=110) | Age13 (N=110) | Age14 (N=73) |
|---|---|---|---|---|
| 0 (T1) | 1.00 | 1.00 | 1.00 | 1.00 |
| 3 (T2) | 0.99 | 0.98 | 0.97 | 0.97 |
| 9 (T3) | 0.93 | 0.90 | 0.87 | 0.87 |
| 15 (T4) | 0.87 | 0.83 | 0.78 | 0.75 |
| 20 (T5) | 0.86 | 0.73 | 0.63 | 0.61 |
Conclusions and Discussion
Over a 20-month period, the survival analysis revealed that for the total sample of low-income African American adolescent females, 28.5% experienced initiation of sexual activity. Although the majority of the adolescent females in this longitudinal prospective research continued to delay the initiation of sexual activity, the non-survival of a little over a quarter of all the adolescents was alarming. It was even more alarming per age group: more than a third of the 13 and 14 year old adolescents and a little over a fourth of the 12 year old adolescents initiated sexual activity. These rates in this study reflected a more extensive and comprehensive perspective and assessment of sexual activity as including vaginal, anal, and/or oral sexual intercourse, which may provide a more accurate reflection of reality. While most studies have focused exclusively on vaginal sex, this exclusive focus may not reflect these adolescents' true risk. Though these rates were higher than rates reported for an older adolescent Caucasian population that focused primarily on vaginal sexual intercourse (Meier, 2003; Mcneely et al., 2002), these rates were consistent with the report that African American females, compared to Caucasian females, were more likely to have their first sexual activity before their 13th birthday (Grunbaum et al., 2004). Our 11 year old adolescents had a similar sexual initiation rate as those African American adolescent females with a mean age of 11 years in the prospective study conducted by McBride, Paikoff, and Hombeck (2003).
This longitudinal prospective examination of the initiation of sexual activity revealed never before reported data on the timing of sexual initiation for African American adolescent females. For the 12, 13 and 14 year old adolescents in our sample, initiation of sexual activity began within three to nine months and continued through 20 months. These low-income African American adolescents starting at age 12 years were very vulnerable to early initiation of sexual activity. Residing in low-income inner city neighborhoods has been associated with early initiation of sexual activity (Ramirez-Valles, Zimmerman, & Juarez, 2002) and with assuming adult roles at an early age for African American adolescents (Hamburg, 1997; Doswell, Millor, Thompson et al. 1998). In addition, CDC (2008) reported that poverty has and continues to play a decisive role in African American females' increased HIV risk.
Predictors of initiation of sexual activity were the adolescent's perception of maternal monitoring and intention to refuse sex. In their comprehensive review of 69 research studies that focused on adolescent sexual behavior, Buhi and Goodson (2007) found that weak environmental restraints were consistently reported as a predictor for initiating sexual activity. Weak environmental restraints were defined as the lack of parental monitoring that permits adolescents to spend considerable time alone with the opposite sex. Additionally, qualitative studies have revealed that adolescents perceived lack of parental monitoring and being home alone as risk factors for initiation of sexual activity and for engaging in sexual activity (Dancy, Kaponda, Kachingwe, & Norr, 2006; Dancy, 2003; Dancy, 1999). Buhi and Goodson also found that intention was the most consistently and stable reported predictor of initiating sexual activity for adolescents.
HIV transmission knowledge, self-efficacy to refuse sex, living with a single mother and mother's educational level were not predictors of sexual initiation. Similar to cross-sectional research (Bachanas et al., 2002) and longitudinal research (O'Donnell, Myint-U, O'Donnell, & Stueve, 2003), we found that HIV transmission knowledge and self-efficacy to refuse sex were not predictors of sexual initiation. This is not surprising given that knowledge alone has not been sufficient to predict behavior (Fisher, Misovich, & Fisher, 1992; Kirby, 1992). Though HIV transmission knowledge has predicted intention to refuse sex (Dancy, Crittenden, & Talashek, 2006), knowledge without skills is insufficient for behavioral change and maintenance (Fisher, Misovich, & Fisher, 1992; Kirby, 1992). Self-efficacy to refuse sex at T2 was not a predictor for initiation of sexual activity, even before intention to refuse sex was added to the model. Thus, in contrast to the results of the retrospective study of Dancy, Crittenden, and Freels (2006), self-efficacy to refuse sex did not affect survival indirectly through intention to refuse sex. Future research should incorporate self-efficacy as a time-varying predictor of survival. In regards to living with a single mother and mother's educational level, we strongly suspect that the homogenous nature of our low socioeconomic status sample accounted for the lack of predictive power. Additional prospective research is needed given that cross-sectional data (Felton & Bartoces, 2002) and retrospective data (Wu & Thomson, 2001) have yielded a positive association between African American adolescent females' initiation of sexual activity and living with a single mother. This additional research should focus on a heterogeneous sample representing African American adolescent females and their mothers from multiple socioeconomic levels with diverse educational statuses and living arrangements. Even though our prospective data were similar to cross sectional data (Felton & Bartoces) that revealed that adolescents' mothers' education was not a significant predictor of the adolescents' sexual initiation, additional prospective research on a heterogeneous sample would provide further credence for this finding.
Implications
Health care providers need to be cognizant of our results indicating that low-income African American adolescent females are at increased risk for early initiation of sexual activity and that maternal monitoring, as perceived by the adolescent, can help adolescent females delay initiation of sexual activity. Similar to the MDRR HIV risk reduction intervention, other mother-adolescent HIV prevention interventions (DiIorio et al., 2006; Wu et al., 2003; Stanton et al., 2004) have not been successful in helping adolescents delay initiation of sexual activity. While our prospective survival results underscore the critical importance of maternal monitoring, these HIV risk reduction interventions have typically not included maternal monitoring as an essential component. Including strategies in sex education and HIV risk reduction interventions to promote effective maternal monitoring may prove to be beneficial for adolescents. Future research is needed to explore the efficacy of maternal monitoring in delaying initiation of sexual activity.
Limitation
The self-report of sensitive information related to sexual behavior is a limitation. However with the use of A-CASI, maximal privacy was provided in the report of sexual information. In use with African American children between the ages of 9 and 15 years, compared to face-to-face interviews, the A-CASI was found to be more effective in eliciting honest reports about sexual activity (Romer et al., 1997). In addition, the A-CASI elicited less response bias than self-administered questionnaires (Gribble, Miller, Rogers, & Turner, 1999). The use of a single item to measure sexual activity may be a limitation. A single item measure reduces the ability to determine internal consistency of the measure (Nagy, 2002). Lastly, another limitation is the inclusion of adolescents who received the HIV risk reduction content. However, this limitation is minor given the fact that the HIV risk reduction content had no effect on the initiation of sexual activity.
Conclusion
Low-income African American adolescent females beginning at age 12 are at risk for initiating sexual activity and are more inclined to initiate sexual activity as they age. Future research should focus on the exploration of the essential components of neighborhood programs designed to enhance adolescents' HIV risk reduction behaviors. These programs should be culturally sensitive and age specific HIV risk reduction interventions that enhance adolescents' intention to refuse sex and parental monitoring of adolescents' behaviors and whereabouts.
Acknowledgments
The project described was supported by Grant Number RO1 MH63638 from the National Institute of Mental Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institute of Mental Health. We acknowledge Kelvin Rodolfo, PhD, for his work in the production of Figure 1.
Funding Source: NIH: NIMH RO1 MH63638
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Barbara L. Dancy, Email: bdancy@uic.edu, University of Illinois at Chicago, 845 South Damen, Office 1060, M/C 802, Chicago, IL 60612, 312-996-9168 (Office), 312-996-9049 (Fax).
Kathleen S. Crittenden, Email: kcritt@uic.edu, University of Illinois at Chicago, E8022 Bakkom Road, Viroqua, WI 54665, 608-637-6159 (Office).
Hongyan Ning, Email: h-ninq@northwestern.edu, Northwestern University, 680 N. Lake Shore Dr., Suite 1102, Chicago, IL 60611, 312-503-2766 (Office), 312-503-2707 (Fax).
References
- Bachanas PJ, Morris MK, Lew-Gess JK, Sarett-Cuasay EJ, Sirl K, Ries JK, et al. Predictors of risky sexual behavior in African American girls: Implications for prevention interventions. Journal of Pediatric Psychology. 2002;27(6):519–530. doi: 10.1093/jpepsy/27.6.519. [DOI] [PubMed] [Google Scholar]
- Bandura A. Self-efficacy mechanism in human agency. American Psychologist. 1982;37:122–147. [Google Scholar]
- Buhi ER, Goodson P. Predictors of adolescent sexual behavior and intention: A theory guided systematic review. Journal of Adolescent Health. 2007;40:4–21. doi: 10.1016/j.jadohealth.2006.09.027. [DOI] [PubMed] [Google Scholar]
- Burns N, Grove SK. The practice of nursing research: Conduct, critique, & utilization. Philadelphia: W. B. Saunders; 2001. [Google Scholar]
- Centers for Disease Control and Prevention. Cases of HIV infection and AIDS in the United States, by race/ethnicity, 2000-2004. HIV/AIDS Surveillance Supplemental Report. 2006;12(1):17–21. [Google Scholar]
- Centers for Disease Control and Prevention. HIV and AIDS in the United States: A picture of today's epidemic. 2008 Retrieved August 4, 2008 from http://www.cdc.gov/hiv/topics/surveillance/united_states/htm.
- Chicago Department of Public Health. STD/HIV/AIDS Chicago. Chicago, Illinois: Chicago Department of Public Health; 2008. [Google Scholar]
- City of Chicago Department of Public Health. Community area health inventory, 1996-1998: Volume I: Demographic and health profiles. Chicago, Illinois: Chicago Department of Public Health; 2000a. [Google Scholar]
- City of Chicago Department of Public Health. Community area health inventory, 1996-1998: Volume II: Rankings. Chicago, Illinois: Chicago Department of Public Health; 2000b. [Google Scholar]
- Collett D. Modelling survival data in medical research. London: Chapman and Hall; 1999. [Google Scholar]
- Dancy BL, Crittenden KS, Freels S. African American adolescent females' predictors of having sex. Journal of National Black Nurses Association. 2006;17(2):30–38. [PubMed] [Google Scholar]
- Dancy BL, Crittenden KS, Talashek M. Mothers' effectiveness as HIV risk reduction educators for adolescent daughters. Journal of Health Care for the Poor and Underserved. 2006;17:218–239. doi: 10.1353/hpu.2006.0012. [DOI] [PubMed] [Google Scholar]
- Dancy BL, Kaponda C, Kachingwe S, Norr K. Risky sexual behaviors of adolescents in rural Malawi: Evidence from focus groups. Journal of National Black Nurses Association. 2006;17(1):22–28. [PubMed] [Google Scholar]
- Dancy BL. Focus on solutions: A community-based mother/daughter HIV risk reduction intervention. In: Gilbert DJ, Wright EM, editors. African American women and HIV/AIDS. Westport, CT: Praeger Publisher; 2003. pp. 183–189. [Google Scholar]
- Dancy BL. AIDS-risk behaviors and situations as perceived by adolescents in Gaborone, Botswana. Journal of National Black Nurses Association. 1999;10:35–45. [PubMed] [Google Scholar]
- DiIorio C, Resnicow K, McCarty F, De AK, Dudley WN, Wang DT, et al. Keepin' it R.E.A.L.! Results of a mother-adolescent HIV prevention program. Nursing Research. 2006;55(1):43–51. doi: 10.1097/00006199-200601000-00006. [DOI] [PubMed] [Google Scholar]
- Doswell WM, Mollor GK, Thompson H, Braxter B. Self-image and self-esteem in African-American preteen girls: Implications for mental health. Issues in Mental Health Nursing. 1998;19:71–94. doi: 10.1080/016128498249222. [DOI] [PubMed] [Google Scholar]
- Eaton DD, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J. Youth risk behavior surveillance – United States, 2007. Morbidity and Mortality Weekly Review: Surveillance Summaries. 2008;57(SS04) [PubMed] [Google Scholar]
- Felton GM, Bartoces M. Predictors of initiation of early sex in black and white adolescent females. Public Health Nursing. 2002;19(1):59–67. doi: 10.1046/j.1525-1446.2002.19008.x. [DOI] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Belief, attitude, intention and behavior: An introduction to theory and research. Boston: Addison-Wesley; 1975. [Google Scholar]
- Fisher JD, Misovich SJ, Fisher WA. Impact of perceived social norms on adolescents' AIDS-risk behavior and prevention. In: DiClemente RJ, editor. Adolescents and AIDS: A Generation in Jeopardy. London: Sage Publications; 1992. pp. 117–136. [Google Scholar]
- Gribble JN, Miller HG, Rogers SM, Turner CF. Interview mode and measurement of sexual behaviors: Methodological issues. Journal of Sex Research. 1999;36(1):16–24. doi: 10.1080/00224499909551963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grunbaum JA, Kann L, Kinchen S, Ross J, Hawkins J, Lowry R, et al. Youth risk behavior surveillance - United States, 2003. Morbidity and Mortality WeeklyRreport: CDC Surveillance summaries. 2004;53(2):1–95. [PubMed] [Google Scholar]
- Hall HI, Song R, McKenna MT. Increases in HIV diagnoses--29 states, 1999-2002. Morbidity and Mortality Weekly Report. 2003;52(47):1145–1148. [PubMed] [Google Scholar]
- Hamburg DA. Toward a strategy for healthy adolescent development. American Journal of Psychiatry. 1997;154:7–12. doi: 10.1176/ajp.154.6.6. [DOI] [PubMed] [Google Scholar]
- Kinsman SB, Romer D, Furstenberg FF, Schwarz DF. Early sexual initiation: The role of peer norms. Pediatrics. 1998;102(5):1185–1192. doi: 10.1542/peds.102.5.1185. [DOI] [PubMed] [Google Scholar]
- Kirby D. School-based programs to reduce sexual risk-taking behaviors. Journal of School Health. 1992;62:280–287. doi: 10.1111/j.1746-1561.1992.tb01244.x. [DOI] [PubMed] [Google Scholar]
- Kleinbaum DG. Survival analysis: A self-learning text. New York: Springer-Verlag; 1996. [Google Scholar]
- Mandara J, Murray CB, Bangi AK. Predictors of African American adolescent sexual activity: An ecological framework. Journal of Black Psychology. 2003;29(3):337–356. [Google Scholar]
- Mathews C, Aaro LE, Flisher AJ, Mukoma W, Wubs AG, Schaalma H. Predictors of early first sexual intercourse among adolescents in Cape Town, South Africa. Health Education Research. 2009;24(1):1–10. doi: 10.1093/her/cym079. [DOI] [PubMed] [Google Scholar]
- McBride CK, Paikoff RL, Holmbeck GN. Individual and familial influences on the onset of sexual among urban African Ameircan adolescents. Journal of Consulting and Clinical Psychology. 2003;71(1):159–167. [Google Scholar]
- Mcneely C, Shew ML, Beuhring T, Sieving R, Miller BC, Blum RWM. Mothers' influence on the timing of first sex among 14 and 15-year-olds. Journal of Adolescent Health. 2002;31(3):256–265. doi: 10.1016/s1054-139x(02)00350-6. [DOI] [PubMed] [Google Scholar]
- Meier AM. Adolescents' transition to first, religiosity, and attitudes about sex. Social Forces. 2003;81(3):1031–1052. [Google Scholar]
- Mitchell CM, Whitesell NR, Spicer P, Beals J, Kaufman CE, the Pathways of Choice Healthy Ways Project Team Cumulative risk for early sexual initiation among American Indian youth: A discrete-time survival analysis. Journal of Research on Adolescence. 2007;17(2):387–412. [Google Scholar]
- Nagy MS. Using a single-item approach to measure facet job satisfaction. Journal of Occupational & Organizational Psychology. 2002;75(1):77–86. [Google Scholar]
- O'Donnell L, O'Donnell CR, Stueve A. Early sexual initiation and subsequent sex-related risks among urban minority youth: The reach for health study. Family Planning Perspectives. 2001;33(6):268–275. [PubMed] [Google Scholar]
- O'Donnell L, Myint-U A, O'Donnell CR, Stueve A. Long-term influence of sexual norms and attitudes on timing of sexual initiation among urban minority youth. Journal of School Health. 2003;73(2):68–75. doi: 10.1111/j.1746-1561.2003.tb03575.x. [DOI] [PubMed] [Google Scholar]
- Ramirez-Valles J, Zimmerman M, Juarez L. Gender differences of neighborhood and social control processes: A study of the timing of first among low-achieving, urban, African-American youth. Youth and Society. 2002;33:418–441. [Google Scholar]
- Romer D, Hornik R, Stanton B, Black M, Li X, Ricardo I, et al. “Talking” computers: A reliable and private method to conduct interviews on sensitive topics with children. The Journal of Sex Research. 1997;34(1):3–9. [Google Scholar]
- Rosenthal SL, Von Ranson KM, Cotton S, Biro FM, Mills L, Succop PA. Sexual initiation: Predictors and developmental trends. Sexually Transmitted Diseases. 2001;28(9):527–532. doi: 10.1097/00007435-200109000-00009. [DOI] [PubMed] [Google Scholar]
- Stanton BF, Black M, Feigelman S, Ricardo I, Galbraith J, Kaljee L, et al. Development of a culturally, theoretically and developmentally based survey instrument for assessing risk behaviors among African-American early adolescents living in urban low-income neighborhoods. AIDS Education and Prevention. 1995;7(2):160–177. [PubMed] [Google Scholar]
- Stanton B, Cole M, Galbraith J, Li X, Pendleton S, Cottrel L, et al. Randomized trial of a parent intervention: Parents can make a difference in a long-term adolescent risk behaviors, perception, and knowledge. Archive of Pediatrics Adolescent Medicine. 2004;158:947–955. doi: 10.1001/archpedi.158.10.947. [DOI] [PubMed] [Google Scholar]
- Stanton BF, Li X, Black MM, Ricardo I, Galbraith J, Feigelman S, et al. Longitudinal stability and predictability of sexual perceptions, intentions, and behaviors among early adolescent African-Americans. Journal of Adolescent Health. 1996;18:10–19. doi: 10.1016/1054-139x(95)00070-9. [DOI] [PubMed] [Google Scholar]
- Steinberg L, Lamborn SD, Darling N, Mounts NS, Dornbusch SM. Over-time changes in adjustment and competence among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child development. 1994;65(3):754–770. doi: 10.1111/j.1467-8624.1994.tb00781.x. [DOI] [PubMed] [Google Scholar]
- Steinberg L, Lamborn SD, Dornbusch SM, Darling N. Impact of parenting practices on adolescent achievement: Authoritative parenting, school involvement, and encouragement to succeed. Child development. 1992;63(5):1266–1281. doi: 10.1111/j.1467-8624.1992.tb01694.x. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Yoder KA, Hoyt DR, Conger RD. Early adolescent sexual activity: A developmental study. Journal of Marriage and the Family. 1999;61(4):934–946. [Google Scholar]
- Wu Y, Stanton BF, Galbraith J, Kaljee L, Cottrell L, Li X, et al. Sustaining and broadening intervention impact: A longitudinal randomized trial of 3 adolescent risk reduction approaches. Pediatrics. 2003;111(1):e32–e38. doi: 10.1542/peds.111.1.e32. Retrieved September 4, 2007, from http://www.pediatrics.org/cgi/content/full/111/1/e32. [DOI] [PubMed] [Google Scholar]
- Wu LL, Thomson E. Race differences in family experience and early sexual initiation: Dynamic models of family structure and family change. Journal of Marriage and the Family. 2001;63(3):682–696. [Google Scholar]