

Abstract
Endometrial polyps, submucous fibroids, uterine septa, and intrauterine adhesions can be found by ultrasound (US), HSG, hysteroscopy, or any combined in 10–15 % of infertile women. Observational studies suggest a better reproductive outcome when these anomalies are removed by operative hysteroscopy. The current Cochrane review assesses the effectiveness of hysteroscopy for treating these suspected anomalies in women with otherwise unexplained infertility or prior to intrauterine insemination, in vitro fertilization, or intracytoplasmic sperm injection.
Keywords: Hysteroscopy, Subfertility, Uterine cavity abnormalities, Randomized controlled trial
Background
Endometrial polyps, submucous fibroids, uterine septa, and intrauterine adhesions can be found by ultrasound (US), HSG, hysteroscopy, or any combined in 10–15 % of infertile women. Observational studies suggest a better reproductive outcome, when these anomalies are removed by operative hysteroscopy. The current Cochrane review assesses the effectiveness of hysteroscopy for treating these suspected anomalies in women with otherwise unexplained infertility or prior to intrauterine insemination (IUI), in vitro fertilization (IVF), or intracytoplasmic sperm injection (ICSI) [1].
Methods
We searched electronic databases including CENTRAL (The Cochrane Library 2012, Issue 7), MEDLINE (1950 to 27 October 2012), and EMBASE (1974 to 27 October 2012) conference proceedings from the American Society for Reproductive Medicine through hand searching (from 2008 to 30 October 2012) and reference lists of retrieved articles. Eligible reports were parallel-design randomized trials (RCTs), comparing operative hysteroscopy with a control intervention in women with suspected uterine cavity abnormalities and otherwise unexplained infertility or undergoing IUI, IVF, or ICSI. The primary outcomes were live birth and hysteroscopy complication rates. Secondary outcomes were ongoing or clinical pregnancy and miscarriage rates. We expressed the dichotomous outcome measures as Mantel–Haenszel odds ratios (ORs) with 95 % confidence intervals (CIs) using a fixed-effect model.
Results
Trial quality
Only two studies met the eligibility criteria for inclusion in the review. One study included 94 women with otherwise unexplained infertility and not more than two submucous fibroids or one submucous fibroid combined with one intramural fibroid, all smaller than 40 mm [2]. The second trial [5] assessed the effectiveness of the hysteroscopic removal of endometrial polyps with a mean diameter of 16 mm diagnosed by Doppler US in 215 women bound to undergo gonadotropin treatment and IUI for unexplained, male or female factor infertility for at least 2 years. Both trials used computer-generated random number tables; in only one allocation concealment was adequate [5]. Blinding of patients, personnel, and outcome assessors was not assessed because these items are less relevant in the setting of a surgical trial with unequivocal outcomes and a long follow-up period. Both studies were at low risk for attrition bias but had some potential for selective outcome reporting; no data for live birth rates were available despite long follow up periods of 86 [2] and 50 months [5]. We could not do a formal assessment of publication bias, since only two RCTs were included in the current review.
Primary outcomes: live birth and hysteroscopy complication rates
We retrieved no data for all primary outcomes.
Secondary outcomes
Clinical pregnancy rates
Removal of not more than two submucous fibroids or one submucous fibroid combined with one intramural fibroid, all smaller than 40 mm, in women with unexplained infertility for at least 1 year tends to increase the odds of clinical pregnancy compared to regular fertility-oriented intercourse. The differences between both comparison groups fail to reach statistical significance (OR 2.4, 95 % CI 0.97–6.2) (Fig. 1). Our results are not in accordance with the calculation of the authors in the primary study report; they reported statistically significant differences between both comparison groups both in women with not more than two submucous fibroids only or one submucous combined with one intramural fibroid [2].
Fig. 1.
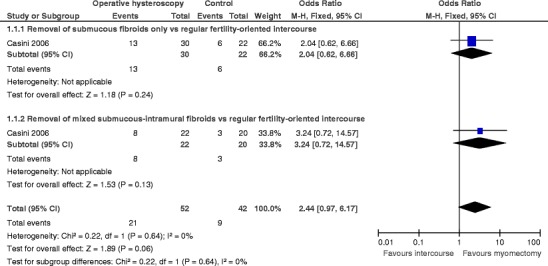
Forest plot of comparison: 1 Hysteroscopic myomectomy vs. regular fertility-oriented intercourse in women with unexplained subfertility and not more than two submucous fibroids or one submucous fibroid combined with one intramural fibroid, all smaller than 40 mm. Outcome: 1.1 Clinical pregnancy
The hysteroscopic removal of endometrial polyps with a mean size of 16 mm increases the odds of clinical pregnancy prior to IUI for unexplained male or female factor infertility for at least 2 years, compared to diagnostic hysteroscopy and polyp biopsy only (OR 4.4, 95 % CI 2.5–8.0).
Miscarriage rates
There is no evidence for differences in the miscarriage rates after the hysteroscopic removal of not more than two submucous fibroids or one submucous fibroid with one intramural fibroid in women with otherwise unexplained infertility for at least 1 year, compared to regular fertility-oriented intercourse (OR 1.5, 95 % CI 0.47–5.00).
Conclusions
The only randomized study published in the literature on the hysteroscopic removal of fibroids in infertile women has claimed statistically significant differences in the clinical pregnancy rates between both comparison groups. Our own recalculation of the available data fails to demonstrate statistically significant differences. This statistical error raises concerns about the validity of the published primary data. Moreover, we judged the overall study quality study to be very low. This has implications for clinical research; additional RCTs studying the effectiveness of hysteroscopic myomectomy in infertile women are needed. The implications for daily practice are more controversial. The gynecological profession widely accepts that submucosal and intramural fibroids interfere with fertility in decreasing order of importance based on the results and conclusions of a large systematic literature review with a meta-analysis of observational studies [6, 7]. While conservative, medical, and surgical treatment are all considered as being appropriate for treating symptomatic fibroids, myomectomy seems the only reasonable treatment option for women who wish to become pregnant. Women treated by hysteroscopic myomectomy for submucosal fibroids might have similar reproductive outcomes as infertile women with normal uterine cavities [8]. According to one prospective study, the surgical removal of large intramural fibroids in women with otherwise unexplained infertility prior to IVF treatment might increase the likelihood of a successful reproductive outcome [4]. Our critical appraisal of the current evidence supports the conclusion published by others in the recent past; at the present, there is still evidence of uncertainty on the effectiveness of removing fibroids in infertile women [3].
The hysteroscopic removal of endometrial polyps in women bound to undergo IUI for unexplained, male, or female factor infertility for at least 24 months increases the odds of clinical pregnancy compared to diagnostic hysteroscopy and biopsy only. The level of evidence of this single study was graded as high.
More well-designed pragmatic RCTs are needed to assess the effectiveness of the hysteroscopic removal of endometrial polyps, submucous fibroids, uterine septa, or intrauterine adhesions in women with otherwise unexplained infertility or prior to IUI, ICSI, or IVF, preferably measuring live birth and adverse events as primary outcomes. The effects of the number, size, and location of the intrauterine pathology as well as the relationship between the timing of the hysteroscopy and subsequent fertility treatment should be addressed by predefined and sensible subgroup analyses.
References
- 1.Bosteels J, Kasius J, Weyers S, Broekmans FJ, Mol BWJ, D’Hooghe TM (2013) Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities. Cochrane Database of Systematic Reviews Issue 1. Art. No.:CD009461 [DOI] [PubMed]
- 2.Casini ML, Rossi F, Agostini R, Unfer V. Effects of the position of fibroids on fertility. Gynecol Endocrinol. 2006;22(2):106–9. doi: 10.1080/09513590600604673. [DOI] [PubMed] [Google Scholar]
- 3.Farquhar C. Do uterine fibroids cause infertility and should they be removed to increase fertility? British Med J. 2009;338:b126. doi: 10.1136/bmj.b126. [DOI] [PubMed] [Google Scholar]
- 4.Hart R, Khalaf Y, Yeong CT, Seed P, Taylor A, Braude P. Prospective controlled study of the effects of uterine fibroids on the outcome of assisted conception treatment. Hum Reprod. 2001;16:2411–2417. doi: 10.1093/humrep/16.11.2411. [DOI] [PubMed] [Google Scholar]
- 5.Pérez-Medina T, Bajo-Arenas J, Salazar F, Redondo T, Sanfrutos L, Alvarez P, et al. Endometrial polyps and their implication in the pregnancy rates of patients undergoing intrauterine insemination: a prospective, randomized study. Hum Reprod. 2005;20(6):1632–5. doi: 10.1093/humrep/deh822. [DOI] [PubMed] [Google Scholar]
- 6.Pritts EA. Fibroids and infertility: a systematic review of the evidence. Obstet Gynecol Surv. 2001;56:483–91. doi: 10.1097/00006254-200108000-00022. [DOI] [PubMed] [Google Scholar]
- 7.Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009;91:1215–23. doi: 10.1016/j.fertnstert.2008.01.051. [DOI] [PubMed] [Google Scholar]
- 8.Somigliana E, Vercellini P, Daguati R, Pasin R, De Giorgi O, Crosignani PG. Fibroids and female reproduction: a critical analysis of the evidence. Hum Reprod Updat. 2007;13:465–76. doi: 10.1093/humupd/dmm013. [DOI] [PubMed] [Google Scholar]