

Abstract
Hospital information system is widely used to improve work efficiency of hospitals in China. However, it is lack of the function providing pharmaceutical information service for clinical pharmacists. A novel clinical pharmacy management system developed by our hospital was introduced to improve the work efficiency of clinical pharmacists in our hospital and to carry out large sample statistical analyzes by providing pharmacy information services and promoting rational drug use. Clinical pharmacy management system was developed according to the actual situation. Taking prescription review in the department of general surgery as the example, work efficiency of clinical pharmacists, quality and qualified rates of prescriptions before and after utilizing clinical pharmacy management system were compared. Statistics of 48,562 outpatient and 5776 inpatient prescriptions of the general surgical department were analyzed. Qualified rates of both the inpatient and outpatient prescriptions of the general surgery department increased, and the use of antibiotics decreased. This system apparently improved work efficiency, standardized the level and accuracy of drug use, which will improve the rational drug use and pharmacy information service in our hospital. Meanwhile, utilization of prophylactic antibiotics for the aseptic operations also reduced.
Keywords: Clinical pharmacist, electronic information, pharmaceutical services, prescription review
With the rapid development of computer communication technology in national health reform in China, hospitals have significantly changed their ways in dealing with medical information. Many hospitals introduced hospital information system (HIS) to store, dispose, and manage plenty of medical information by computers, and clinical pharmacy management system (CPMS) is the core part of HIS.[1,2] At present, CPMS in our hospital emphasizes on the guarantee of drug supply including the stock, sell, and store of drugs, i.e., the logistics and fund flow. This system has realized the transition from manual to computer accounting. However, focus of the pharmacists in our hospital has gradually changed to the patient-centered pharmaceutical care.[3,4] The function providing pharmaceutical information service for clinical pharmacists has not been incorporated in the current HIS, which can be remedied by applying the advanced computer software.[5,6]
Currently, main responsibilities of the clinical pharmacists in our hospital include: 1) Cooperating with doctors closely to grasp the overall conditions of patients and completing their corresponding medical records. 2) Before 2011, the clinical pharmacists in our hospital randomly selected 100 outpatient prescriptions and 30 inpatient medical orders monthly to analyze, review, complete, and submit the prescription review lists. 3) Complying with the relative requirements in “Notification on the establishment of clinical use of antibiotics and bacterial resistance monitoring network” (Except for the establishment of national ‘clinical use of antibiotics monitoring network’ and ‘bacterial resistance monitoring network,’ corresponding monitoring should also be gradually carried out in appropriate areas and units.), the clinical pharmacists should randomly select 120 medical records annually to complete and submit the reports. 4) Completing the reports of adverse drug reactions monthly (ADR).
Two problems will arise when the clinical pharmacists in our hospital intend to fulfill the above missions, one of which is the heavy workload. Taking prescription review as the example, pharmacists need to select 100 prescriptions and 30 medical orders equally according to the requirements, and they also need to check the corresponding paper medical records to extract and evaluate the information of prescriptions or medical orders. Besides, it will take more time and efforts to complete the prescription review forms. Especially, filling in the number of basic drugs is in need of checking individual drug information in every prescription. Meanwhile, when filling in the antibacterial drug reports, pharmacists need to check the entire medical records of patients to acquire the requested information, which will take a long time to complete only one report form. In addition, samples consisting of 100 prescriptions, 30 medical orders and 120 medical records are still insufficient, and the data obtained by different samplers will differ greatly during the same period. Thus, the data cannot properly reflect the overall situation of prescriptions and the use of antibiotics.
As a result, it is crucial to effectively improve the overall work efficiency of the pharmacy department by systematizing, standardizing, and scientizing the management. Thereby motivated, a novel CPMS that is more suitable for the clinical pharmacists was developed by our hospital in 2010, and was put into effect on January 1, 2011. The system is connected to HIS of our hospital, which will be able to replace the jobs of clinical pharmacists including manual samplings, reviews of prescriptions (medical orders), and filling in the reports of the use of antibiotics. Besides, CPMS is also able to customize paper prescriptions and medical orders according to “Prescription Administrative Policy” and related laws and regulations.[7,8] The system has been utilized in our hospital for a period of time and performed quite well.
The main advantages of the system embodied in the following aspects. It can provide real-time monitoring for the prescriptions and medical orders and warn the irrational use of drugs timely, which thus greatly improve the qualified rates of prescriptions. According to the relevant rules in “Prescription Administrative Policy” of WHO (Medical institutions should establish prescription review systems, complete prescription review forms, implement dynamic monitor, and abnormal warn for prescriptions, register, and report irrational prescriptions, and intervene irrational drug use in time.)[9,10] It will realize the screening and statistical analysis of large sample cases precisely and thoroughly to meet the requirements of clinical pharmacy research.
Taking prescription review as the example, qualified rates of prescriptions, daily use of antibiotics, and use of antibiotic in aseptic operations in the general surgery department in 2010 and 2011 were counted and compared. The results before and after applying CPMS were summarized below.
MATERIALS AND METHODS
Out of 48,562 outpatient and 5776 inpatient prescriptions recorded in the general surgical department in 2011, 947 cases with class 1 incisions were included. Mean age of the patients was 42±12 years. The cases included 26,879 males and 21,683 females.
Patient information:
Inpatient (or outpatient) numbers, names, gender, ages, weights, hospitalized days. Surgery names and time were also recorded for the patients with class 1 incisions.[11]
Drug information:
The number of used drugs, the number of antibiotics, usage, dosage, and using time of antibiotics were recorded.
Evaluation criteria:
Openness of prescription diagnoses, symptomatic treatments, correct drug use for special groups (elderly, children or patients with special diseases), correct prophylactic drug use for inpatients after aseptic operations, were included.
Statistics:
Large sample cases were screened by CPMS developed by our hospital. The data obtained were subjected to statistical analysis using one way ANOVA.
RESULTS
Large sample prescriptions after using the novel clinical pharmacy management system:
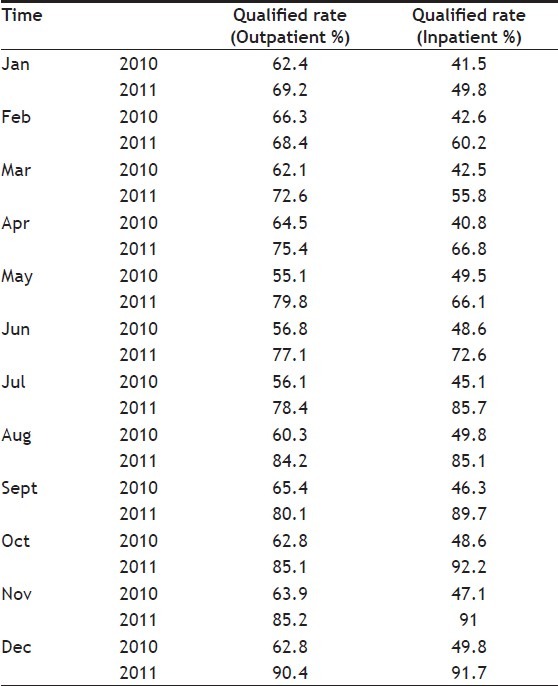
Large samples of all the outpatient and inpatient prescriptions in our hospital were successfully screened by the novel CPMS since January 1, 2011. Qualified rates of the outpatient prescriptions in the general surgery department gradually increased from 44.1% in January to 92.6% in December, and those of the inpatient prescriptions rose from 63.3% in January to 94.6% in December. The results are shown in Table 1.
Table 1.
QUALIFIED RATES OF THE PRESCRIPTIONS OF THE GENERAL SURGERY DEPARTMENT IN 2011

Use of antibiotics for outpatients and inpatients:
Since we applied the new CPMS to intervene the prescriptions in 2011, use of antibiotics for the outpatients in the general surgery department significantly dropped from 33.7% in January to 18.2% in December, and those for the inpatients decreased from 73.5% in January to 32.0% in December. The results are listed in Table 2.
Table 2.
PROPORTION OF ANTIBIOTIC TREATMENT IN 2011 (%)

Use of prophylactic antibiotics for aseptic operations:
We also intervened in the use of prophylactic antibiotics for aseptic operations by the new CPMS. The use of prophylactic antibiotics for the inpatient aseptic operations apparently decreased from 86.92% in January to 33.39% in December in 2011, and the results are summarized in Table 3.
Table 3.
USE OF PROPHYLACTIC ANTIBIOTICS FOR ASEPTIC OPERATIONS IN 2011

Use intensity of antibiotics for inpatients in 2011:
The use of antibiotics in the hospital has been strictly limited by the new CPMS since January 1, 2011, which obviously reduced the defined daily dose (DDD) of antibiotics for the inpatients from 138.92 in January to 36.51 in December as shown in Table 4.
Table 4.
DDD VALUES OF ANTIBIOTICS FOR INPATIENTS IN 2011

Qualified rates of prescriptions before and after utilizing clinical pharmacy management system:
Qualified rates of the outpatient and inpatient prescriptions before and after utilizing CPMS were statistically compared. Considering that inefficient manual counting methods were used to gather prescriptions in our hospital in 2010, only 100 outpatient prescriptions and 30 inpatient medical orders of the general surgery department were collected. However, when the same amount of prescriptions was still collected in 2011, the qualified rates of prescriptions all increased to different extents after employing CPMS since January 1, 2011, as seen in Table 5.
Table 5.
QUQLIFIED RATES OF OUTPATIENT AND INPATEINT PRESCRIPTIONS OF THE GENERAL SURGERY DEPARTMENT
DISCUSSION
Electronic information of patients and prescriptions (medical orders) could be directly acquired by connecting the novel CPMS to the original HIS, which effectively reduced the reading time that clinical pharmacists spent on the paper medical records. Thus, this system will be able to assist the review of all the prescriptions.[12,13]
Before 2011, it took three pharmacists and one week to review 100 prescriptions and 30 medical orders a month, and the quality was also unsatisfactory. Besides, when one or more specific patients, doctors, departments, or diseases were sampled and reviewed, the workload would largely increase. Moreover, it was very difficult to complete the missions manually, and the error rates were relatively higher. On the contrary, it merely took a pharmacist one week to review all the prescriptions or medical orders with the aid of CPMS, which will reduce the workload of clinical pharmacists, enhance the prescription quality, and effectively increase the overall work efficiency of the pharmacy department.
The humanized design of CPMS provided a variety of sampling and screening methods. Parameters including counting time, department, doctor, diagnosis, patient name, inpatient (or outpatient) number, electronic medical record, prescription review, use of antibiotics and others, could be freely set. Then, the system created a list concerning the review and statistical analysis of individual prescriptions or medical orders. Besides, when prescription samplings were required according to “Management Standards of Hospital Prescription Reviews,” desired sampling number or sampling rates of prescriptions could also be set in the screening interface, allowing random samplings and samplings at equal intervals.[14]
Generally, CPMS was mainly utilized to review prescriptions (medical orders) in order to cooperate with doctors closely to prevent irrational drug use timely. Consequently, the system has optimized the workflow in the hospital and increased the qualified rates of prescriptions (or medical orders) steadily. Meanwhile, taking into consideration that the Chinese Ministry of Health launched a nationwide “special action of antimicrobial agents” in 2011 to address the abuse of antibiotics, another important function that could enable the reasonable and orderly use of antibiotics was also incorporated in CPMS.
General aseptic operations with class 1 incisions, such as body surface operations of heads, necks, trunks, and limbs, inguinal hernia hernioplasty without artificial implants, thyroid adenoma resections and breast fibroadenoma resections, mostly do not need antibiotics.[15,16] Antibiotics should only be allowed for the patients that have undergone major aseptic operations and long time operations, and those with large areas of trauma or other high infection risks.[17] The novel CPMS can monitor, timely track, and intervene each operation with class 1 incision, which will reduce the use of prophylactic antibiotics for aseptic operations.
Moreover, DDD, an important index to assess whether excessive antibiotics are used, is also incorporated in CPMS. After the novel CPMS was introduced, DDD values in our hospital significantly decreased to those meeting the requirement of WHO (<40) in a short time.[18,19] Meanwhile, CPMS was compatible with the function of reviewing prescriptions (or medical orders) in the rational drug use monitoring system. After obtaining the information of patients by HIS, pharmacists could use the system to review entire prescriptions (or medical orders), find out irrational use of drugs, and the corresponding reasons with references. Based on the current statistics, the level of outpatient and inpatient prescriptions has been significantly improved by CPMS. Furthermore, medical information search was also incorporated in the system, which was able to accelerate the search for directions, pharmacopeia, clinical medication guides. Thus, the system has effectively reduced the review time of prescriptions (or medical orders) as well as improved the quality.[20,21]
Lastly, the system also granted various permission authorities for users. The highest authorization level in our hospital allowed the users to manage all the reviewed prescriptions and submitted forms to detect problems timely and to realize the management and monitoring of prescriptions.[22] In addition, the system could statistically analyze the drug use conditions in our hospital, which would improve monitoring and provide additional support for decision making.
In summary, the novel CPMS not only effectively facilitated the scientization of pharmacy information service in our hospital, but also performed as an essential part of information construction in our hospital. Besides, the system could fully utilize the resources of local area network and HIS to extract the information of patients including diagnoses and prescriptions (or medical orders). Meanwhile, the resulting electronic records would avoid errors resulted from manual operations. Prescriptions (medical orders) could be reviewed by the system in time to find out irrational drug use and give corresponding references, which would improve the work efficiency of the pharmacy department and provide professional medical instructions. Furthermore, the system was able to economize medical resources, reduce errors, facilitate rational drug use, and eventually promote the clinical drug information services in the whole hospital onto a new level.
Footnotes
Bao, et al.: Novel Clinical Pharmacy Management System
REFERENCES
- 1.Jiang J, Yan Z, Kandachar P, Freudenthal A. A mobile monitoring system of blood pressure for underserved in China by information and communication technology service. IEEE Trans Inf Technol Biomed. 2010;14:748–757. doi: 10.1109/TITB.2010.2043534. [DOI] [PubMed] [Google Scholar]
- 2.Olveda R, Leonardo L, Zheng F, Sripa B, Bergquist R, Zhou XN. Coordinating research on neglected parasitic diseases in Southeast Asia through networking. Adv Parasitol. 2010;72:55–77. doi: 10.1016/S0065-308X(10)72003-0. [DOI] [PubMed] [Google Scholar]
- 3.Zhu M, Guo DH, Liu GY, Pei F, Wang B, Wang DX, et al. Exploration of clinical pharmacist management system and working model in China. Pharm World Sci. 2010;32:411–5. doi: 10.1007/s11096-010-9407-8. [DOI] [PubMed] [Google Scholar]
- 4.Su C, Ji H, Su Y. Hospital pharmacists’ knowledge and opinions regarding adverse drug reaction reporting in Northern China. Pharmacoepidemiol Drug Saf. 2010;19:217–22. doi: 10.1002/pds.1792. [DOI] [PubMed] [Google Scholar]
- 5.Vargas M. A look at Chinese pharmacies: A student’s perspective. Consult Pharm. 2009;24:463–4. doi: 10.4140/tcp.n.2009.052. [DOI] [PubMed] [Google Scholar]
- 6.Chen W, Tang S, Sun J, Ross-Degnan D, Wagner AK. Availability and use of essential medicines in China: Manufacturing, supply, and prescribing in Shandong and Gansu provinces. BMC Health Serv Res. 2010;10:211. doi: 10.1186/1472-6963-10-211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cao M. Wang Ang and his Variorum of medical recipes (Yi fang ji jie) Zhonghua Yi Shi Za Zhi. 2000;30:179–81. [PubMed] [Google Scholar]
- 8.Morgan S, Hanley G, Cunningham C, Quan H. Ethnic differences in the use of prescription drugs: A cross-sectional analysis of linked survey and administrative data. Open Med. 2011;5:e87–93. [PMC free article] [PubMed] [Google Scholar]
- 9.Doyon S, Perreault M, Marquis C, Gauthier J, Lebel D, Bailey B, et al. Quantitative evaluation of a clinical intervention aimed at changing prescriber behaviour in response to new guidelines. J Eval Clin Pract. 2009;15:1111–7. doi: 10.1111/j.1365-2753.2009.01259.x. [DOI] [PubMed] [Google Scholar]
- 10.Wellman GS, Vidican C. Pilot study of a hierarchical Bayes method for utility estimation in a choice-based conjoint analysis of prescription benefit plans including medication therapy management services. Res Social Adm Pharm. 2008;4:218–30. doi: 10.1016/j.sapharm.2007.08.002. [DOI] [PubMed] [Google Scholar]
- 11.Mataftsi A, Tsinopoulos IT, Tsaousis KT, Dimitrakos SA. Perioperative antibiotic prophylaxis during cataract surgery in Greece. J Cataract Refract Surg. 2011;37:1732–3. doi: 10.1016/j.jcrs.2011.07.013. [DOI] [PubMed] [Google Scholar]
- 12.Reuther LO, List SB, Christensen HR. Application of the medicine profile in an ambulatory setting. Ugeskr Laeger. 2008;170:2427–32. [PubMed] [Google Scholar]
- 13.Mayer T. E-prescribing hits the medical world: What physicians need to know to get the right technology. J Med Pract Manage. 2001;17:103–5. [PubMed] [Google Scholar]
- 14.Bernstein PS, Sanghvi T, Merkatz IR. Improving preconception care. J Reprod Med. 2000;45:546–52. [PubMed] [Google Scholar]
- 15.Chinese Medical Association; Pharmacy Professional Advisory Committee of Chinese Hospital Association; Hospital Pharmacy Advisory Committee of Chinese Pharmaceutical Association. Guiding Principles for Clinical Application of Antibiotics. Adver Drug React J. 2005;7:42. [Google Scholar]
- 16.Yan X, Tao X, He L, Cui Z, Zhang J. Increasing resistance in multiresistant methicillin-resistant Staphylococcus aureus clones isolated from a Chinese hospital over a 5-year period. Microb Drug Resist. 2011;17:235–9. doi: 10.1089/mdr.2010.0029. [DOI] [PubMed] [Google Scholar]
- 17.Currie J, Lin W, Zhang W. Patient knowledge and antibiotic abuse: Evidence from an audit study in China. J Health Econ. 2011;30:933–49. doi: 10.1016/j.jhealeco.2011.05.009. [DOI] [PubMed] [Google Scholar]
- 18.Evirgen O, Onlen Y, Ertan O. The intensity of antibiotic usage in the university hospital and the investigation of an inappropriate use of antibiotics. Bratisl Lek Listy. 2011;112:595–598. [PubMed] [Google Scholar]
- 19.Dumartin C, L’Heriteau F, Pefau M, Bertrand X, Jarno P, Boussat S, et al. Antibiotic use in 530 French hospitals: Results from a surveillance network at hospital and ward levels in 2007. J Antimicrob Chemother. 2010;65:2028–36. doi: 10.1093/jac/dkq228. [DOI] [PubMed] [Google Scholar]
- 20.Mahajan B, Kjar D, Godwin D, Robertson A, Ponder T. PS1-26: Data quality issues/checks while building virtual data warehouse enrollment, demographics, provider and utilization tables from scratch. Clin Med Res. 2011;9:184–5. [Google Scholar]
- 21.Yang TH, Ku CY, Yen DC, Hsieh WH. Electronic Hand-Drafting and Picture Management System. J Med Syst. 2012;36:2297–307. doi: 10.1007/s10916-011-9697-y. [DOI] [PubMed] [Google Scholar]
- 22.Deitelzweig SB, Lin J, Kreilick C, Hussein M, Battleman D. Warfarin therapy in patients with venous thromboembolism: Patterns of use and predictors of clinical outcomes. Adv Ther. 2010;27:623–33. doi: 10.1007/s12325-010-0056-z. [DOI] [PubMed] [Google Scholar]