

Abstract
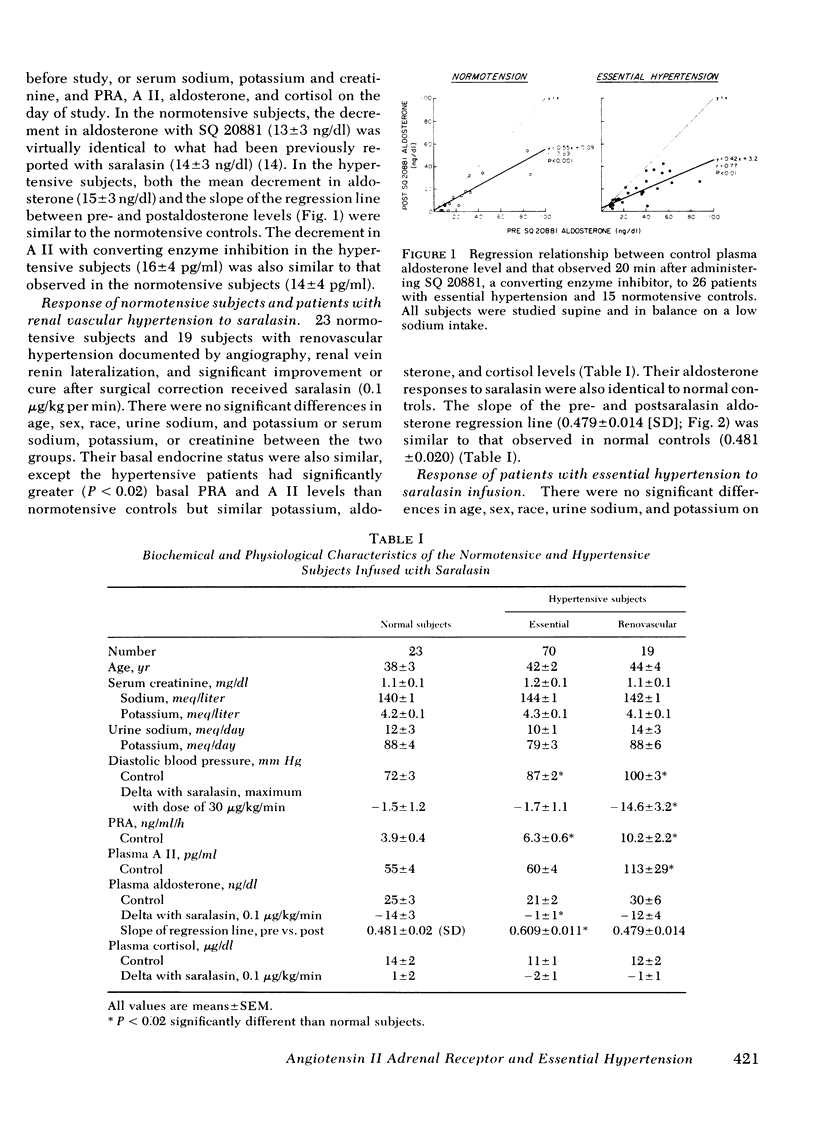
To determine the mechanism underlying altered adrenal responsiveness in patients with essential hypertension, the renin-angiotensin-aldosterone axis was assessed in normotensive and hypertensive subjects using three pharmacological probes: SQ 20881, a converting enzyme inhibitor; saralasin, a competitive angiotensin antagonist with prominent agonist properties; and angiotensin itself. All subjects were studied while supine and in balance on a 10 meq Na/100 meq K intake. The decrement in plasma aldosterone with SQ 20881 in 26 hypertensive subjects (15±3 ng/dl) was normal (13±4 ng/dl), suggesting that the altered adrenal responsiveness in hypertensives is not because of a change in a postreceptor event or in the relative contribution of angiotensin to the control of aldosterone secretion.
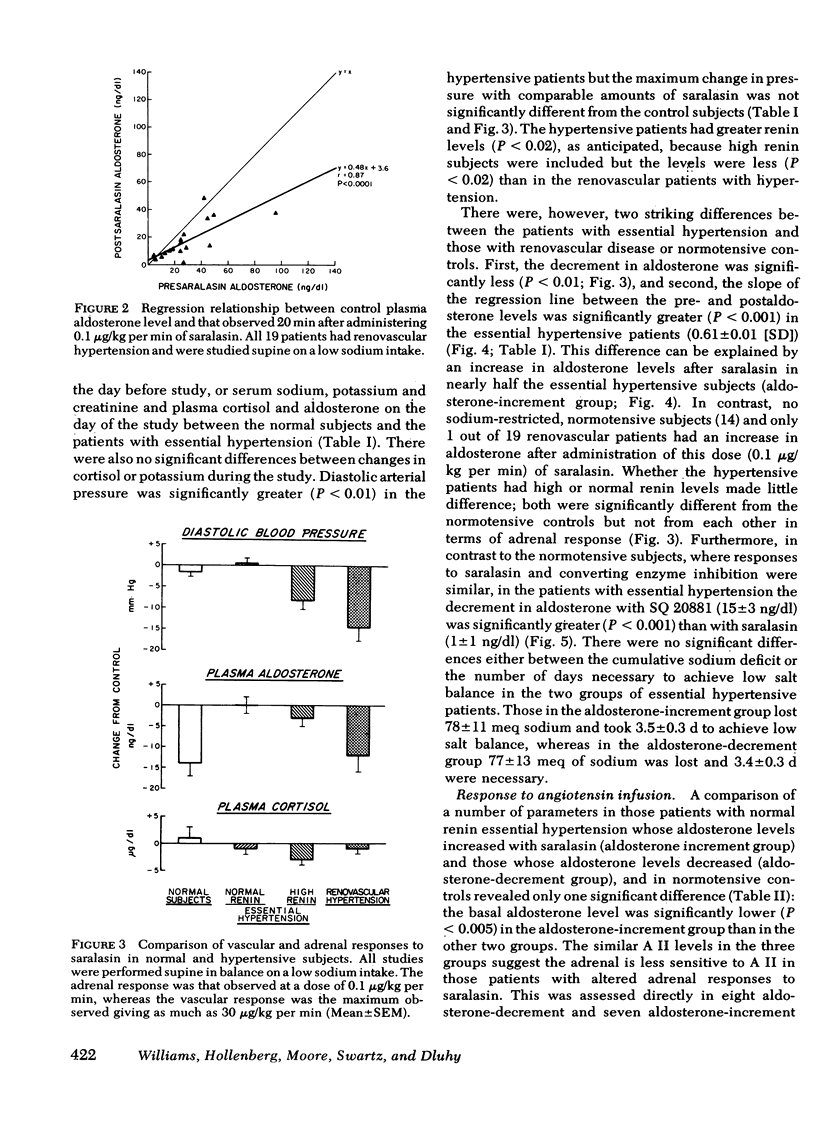
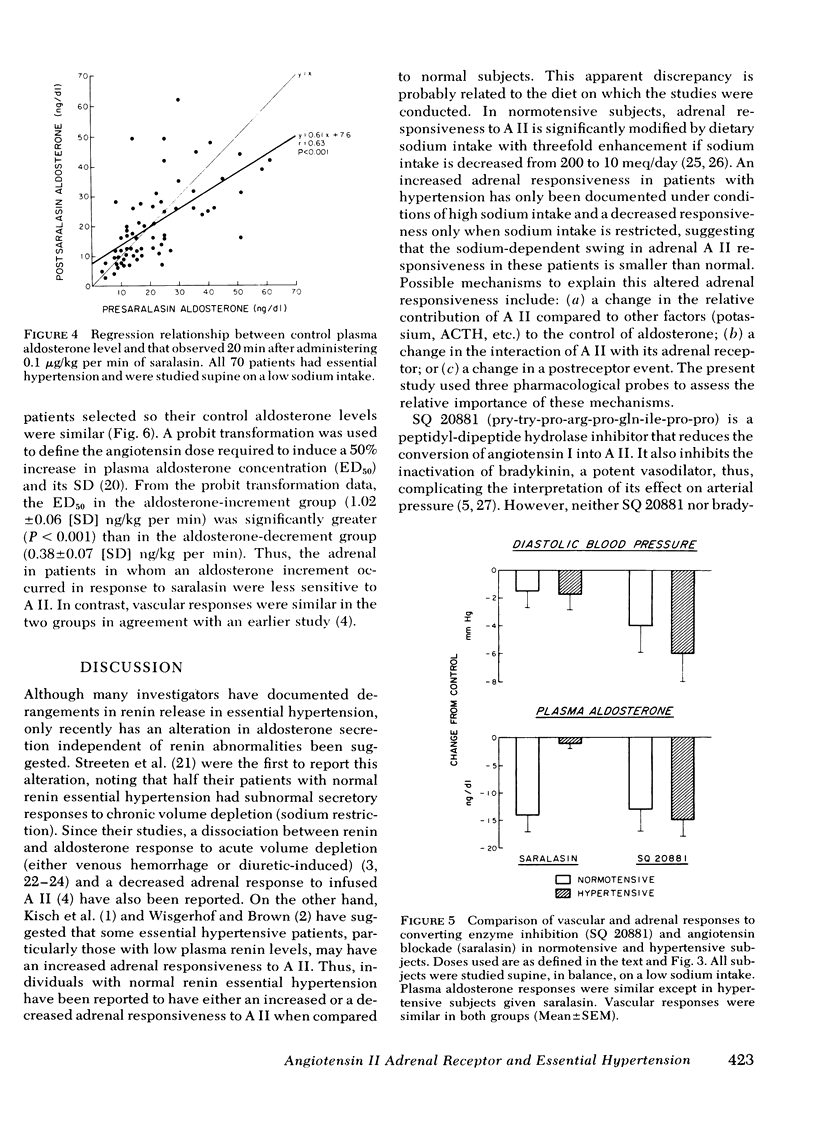
Saralasin at a dose (0.1 μg/kg per min) that reduced aldosterone levels in all normals produced a normal aldosterone decrement (14±3 ng/dl) in 19 patients with renovascular hypertension (12±4 ng/dl). The same dose, however, had no net effect on plasma aldosterone levels in 70 patients with normal or high renin essential hypertension (−1±1 ng/dl) despite identical metabolic balance and control renin and angiotensin levels. The altered response could be explained by an agonist effect, aldosterone rising in 45 of the essential hypertensives. There were no significant differences between normal and abnormal responders in pre- and postcortisol, -potassium, -renin and -angiotensin concentrations.
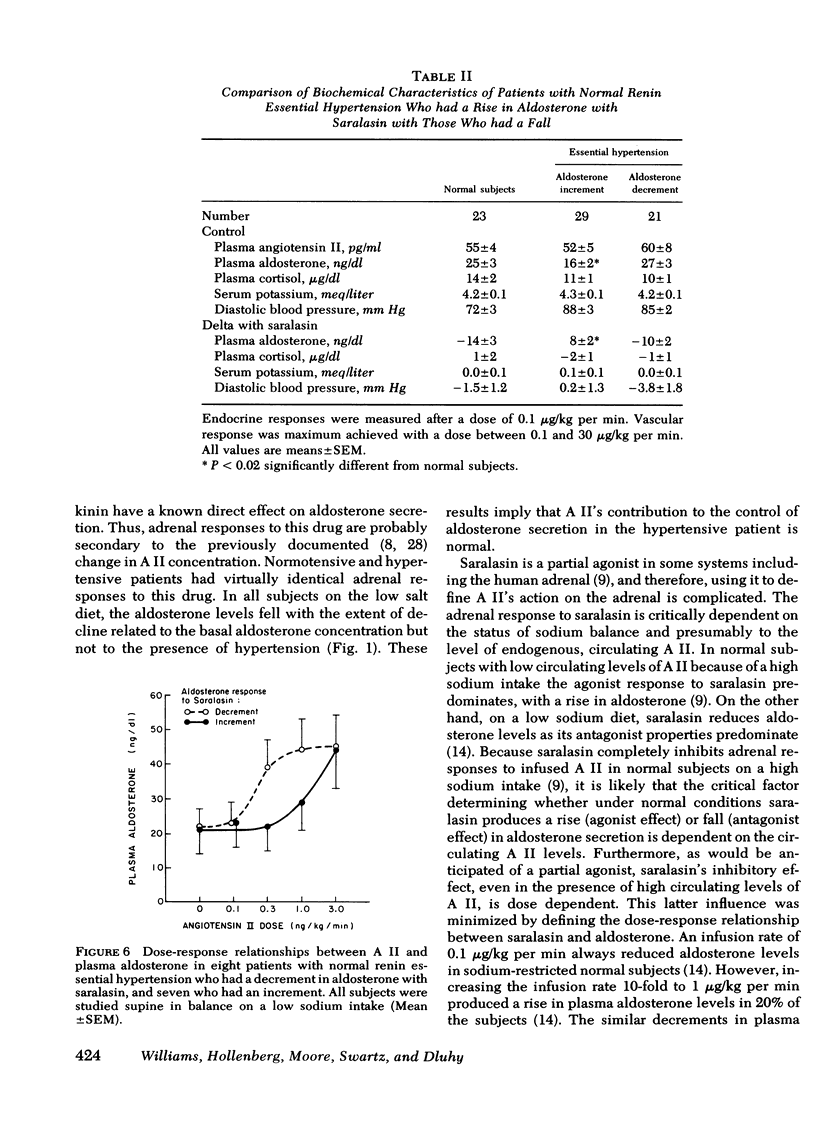
Angiotensin was infused (0.1-3 ng/kg per min) in 15 patients with normal renin essential hypertension, previously studied with saralasin. A probit transformation defined the dose required to induce a 50% increase in aldosterone (ED50). In the patients in whom aldosterone rose with saralasin, the dose required to induce a 50% increase was significantly greater (P < 0.001) than in those in whom aldosterone fell normally (1.02±0.06 [SD] vs. 0.38±0.07 ng/kg per min). Vascular responses were similar in the various groups. We conclude that altered adrenal responsiveness to angiotensin in some essential hypertensive patients is secondary to a change in the interaction of angiotensin with its adrenal receptor.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Brown R. D., Tucker R., Tue K., Wisgerhof M., Salassa R. Effect of saralasin on plasma aldosterone in hypertensive man. J Lab Clin Med. 1978 Mar;91(3):473–479. [PubMed] [Google Scholar]
- Case D. B., Wallace J. M., Keim H. J., Weber M. A., Sealey J. E., Laragh J. H. Possible role of renin in hypertension as suggested by renin-sodium profiling and inhibition of converting enzyme. N Engl J Med. 1977 Mar 24;296(12):641–646. doi: 10.1056/NEJM197703242961201. [DOI] [PubMed] [Google Scholar]
- Christlieb A. R., Hickler R. B., Lauler D. P., Williams G. H. Hypertension with inappropriate aldosterone stimulation. N Engl J Med. 1969 Jul 17;281(3):128–131. doi: 10.1056/NEJM196907172810304. [DOI] [PubMed] [Google Scholar]
- Collier J. G., Robinson B. F., Vane J. R. Reduction of pressor effects of angiotensin I in man by synthetic nonapeptide (B.P.P. 9a or SQ 20,881) which inhibits converting enzyme. Lancet. 1973 Jan 13;1(7794):72–74. doi: 10.1016/s0140-6736(73)90468-6. [DOI] [PubMed] [Google Scholar]
- Collins R. D., Weinberger M. H., Dowdy A. J., Nokes G. W., Gonzales C. M., Luetscher J. A. Abnormally sustained aldosterone secretion during salt loading in patients with various forms of benign hypertension; relation to plasma renin activity. J Clin Invest. 1970 Jul;49(7):1415–1426. doi: 10.1172/JCI106359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emanuel R. L., Cain J. P., Williams G. H. Double antibody radioimmunoassay of renin activity and angiotensin II in human peripheral plasma. J Lab Clin Med. 1973 Apr;81(4):632–640. [PubMed] [Google Scholar]
- Gavras H., Gavras I., Textor S., Volicer L., Brunner H. R., Rucinska E. J. Effect of angiotensin converting enzyme inhibition on blood pressure, plasma renin activity and plasma aldosterone in essential hypertension. J Clin Endocrinol Metab. 1978 Feb;46(2):220–226. doi: 10.1210/jcem-46-2-220. [DOI] [PubMed] [Google Scholar]
- Hauger R. L., Aguilera G., Catt K. J. Angiotensin II regulates its receptor sites in the adrenal glomerulosa zone. Nature. 1978 Jan 12;271(5641):176–178. doi: 10.1038/271176a0. [DOI] [PubMed] [Google Scholar]
- Hollenberg N. K., Chenitz W. R., Adams D. F., Williams G. H. Reciprocal influence of salt intake on adrenal glomerulosa and renal vascular responses to angiotensin II in normal man. J Clin Invest. 1974 Jul;54(1):34–42. doi: 10.1172/JCI107748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollenberg N. K., Williams G. H., Burger B., Ishikawa I., Adams D. F. Blockade and stimulation of renal, adrenal, and vascular angiotensin II receptors with 1-Sar, 8-Ala angiotensin II in normal man. J Clin Invest. 1976 Jan;57(1):39–46. doi: 10.1172/JCI108266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kem D. C., Weinberger M. H., Higgins J. R., Kramer N. J., Gomez-Sanchez C., Holland O. B. Plasma aldosterone response to ACTH in primary aldosteronism and in patients with low renin hypertension. J Clin Endocrinol Metab. 1978 Apr;46(4):552–560. doi: 10.1210/jcem-46-4-552. [DOI] [PubMed] [Google Scholar]
- Kisch E. S., Dluhy R. G., Williams G. H. Enhanced aldosterone response to angiotensin II in human hypertension. Circ Res. 1976 Jun;38(6):502–505. doi: 10.1161/01.res.38.6.502. [DOI] [PubMed] [Google Scholar]
- Moore T. J., Williams G. H., Dluhy R. G., Bavli S. Z., Himathongkam T., Greenfield M. Altered renin-angiotensin-aldosterone relationships in normal renin essential hypertension. Circ Res. 1977 Aug;41(2):167–171. doi: 10.1161/01.res.41.2.167. [DOI] [PubMed] [Google Scholar]
- Oelkers W., Brown J. J., Fraser R., Lever A. F., Morton J. J., Robertson J. I. Sensitization of the adrenal cortex to angiotensin II in sodium-deplete man. Circ Res. 1974 Jan;34(1):69–77. doi: 10.1161/01.res.40.4.69. [DOI] [PubMed] [Google Scholar]
- Park W. K., Regoli D., Rioux F. Characterization of angiotensin receptors in vascular and intestinal smooth muscles. Br J Pharmacol. 1973 Jun;48(2):288–301. doi: 10.1111/j.1476-5381.1973.tb06915.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sancho J., Re R., Burton J., Barger A. C., Haber E. The role of the renin-angiotensin-aldosterone system in cardiovascular homeostasis in normal human subjects. Circulation. 1976 Mar;53(3):400–405. doi: 10.1161/01.cir.53.3.400. [DOI] [PubMed] [Google Scholar]
- Stephens G. A., Davis J. O., Freeman R. H., Watkins B. E., Khosla M. C. The effects of angiotensin II blockade in conscious sodium-depleted dogs. Endocrinology. 1977 Aug;101(2):378–378. doi: 10.1210/endo-101-2-378. [DOI] [PubMed] [Google Scholar]
- Streeten D. H., Anderson G. H., Freiberg J. M., Dalakos T. G. Use of an angiotensin II antagonist (saralasin) in the recognition of "angiotensinogenic" hypertension;. N Engl J Med. 1975 Mar 27;292(13):657–662. doi: 10.1056/NEJM197503272921301. [DOI] [PubMed] [Google Scholar]
- Streeten D. H., Schletter F. E., Clift G. V., Stevenson C. T., Dalakos T. G. Studies of the renin-angiotensin-aldosterone system in patients with hypertension and in normal subjects. Am J Med. 1969 Jun;46(6):844–861. doi: 10.1016/0002-9343(69)90086-2. [DOI] [PubMed] [Google Scholar]
- Tuck M. L., Williams G. H., Cain J. P., Sullivan J. M., Dluhy R. G. Relation of age, diastolic pressure and known duration of hypertension to presence of low renin essential hypertension. Am J Cardiol. 1973 Oct;32(5):637–642. doi: 10.1016/s0002-9149(73)80056-6. [DOI] [PubMed] [Google Scholar]
- Underwood R. H., Williams G. H. The simultaneous measurement of aldosterone, cortisol, and corticosterone in human peripheral plasma by displacement analysis. J Lab Clin Med. 1972 May;79(5):848–862. [PubMed] [Google Scholar]
- Williams G. H., Hollenberg N. K. Accentuated vascular and endocrine response to SQ 20881 in hypertension. N Engl J Med. 1977 Jul 28;297(4):184–188. doi: 10.1056/NEJM197707282970404. [DOI] [PubMed] [Google Scholar]
- Williams G. H., Hollenberg N. K., Braley L. M. Influence of sodium intake on vascular and adrenal angiotensin II receptors. Endocrinology. 1976 Jun;98(6):1343–1350. doi: 10.1210/endo-98-6-1343. [DOI] [PubMed] [Google Scholar]
- Williams G. H., Hollenberg N. K., Brown C., Mersey J. H. Adrenal responses to pharmacological interruption of the renin-angiotensin system in sodium-restricted normal man. J Clin Endocrinol Metab. 1978 Oct;47(4):725–731. doi: 10.1210/jcem-47-4-725. [DOI] [PubMed] [Google Scholar]
- Williams G. H., Rose L. I., Dluhy R. G., McCaughn D., Jagger P. I., Hickler R. B., Lauler D. P. Abnormal responsiveness of the renin aldosterone system to acute stimulation in patients with essential hypertension. Ann Intern Med. 1970 Mar;72(3):317–326. doi: 10.7326/0003-4819-72-3-317. [DOI] [PubMed] [Google Scholar]
- Wisgerhof M., Brown R. D. Increased adrenal sensitivity to angiotensin II in low-renin essential hypertension. J Clin Invest. 1978 Jun;61(6):1456–1462. doi: 10.1172/JCI109065. [DOI] [PMC free article] [PubMed] [Google Scholar]