

Abstract
Cone beam computed tomography is a 3-dimensional high resolution imaging method. The purpose of this study was to compare the effects of 3 different NiTi rotary instruments used to prepare curved root canals on the final shape of the curved canals and total amount of root canal transportation by using cone-beam computed tomography. A total of 81 mesial root canals from 42 extracted human mandibular molars, with a curvature ranging from 15 to 45 degrees, were selected. Canals were randomly divided into 3 groups of 27 each. After preparation with Protaper, Revo-S and Hero Shaper, the amount of transportation and centering ability that occurred were assessed by using cone beam computed tomography. Utilizing pre- and post-instrumentation radiographs, straightening of the canal curvatures was determined with a computer image analysis program. Canals were metrically assessed for changes (surface area, changes in curvature and transportation) during canal preparation by using software SimPlant; instrument failures were also recorded. Mean total widths and outer and inner width measurements were determined on each central canal path and differences were statistically analyzed. The results showed that all instruments maintained the original canal curvature well with no significant differences between the different files (P = 0.226). During preparation there was failure of only one file (the protaper group). In conclusion, under the conditions of this study, all instruments maintained the original canal curvature well and were safe to use. Areas of uninstrumented root canal wall were left in all regions using the various systems.
Keywords: Rotary NiTi instrument, canal curvature, canal straightening
INTRODUCTION
The preparation of the root canal determines the success of all subsequent teps. Adequate instrumentation combined with effective irrigation is required to achieve sufficient disinfection during root canal treatment[1],[2]. The inherent anatomy and morphology of the root canal system imposes other challenges necessary for efficient disinfection. Isthmuses, inter-canal and intra-canal communications, curvatures and oval-shaped canals make disinfection of the root canal system challenging[3]–[6].
The aim of root canal treatment is to clean and shape the canals adequately. The shape of the prepared canals should provide a space for the irrigating solution to optimize the eradication of microorganisms. Additionally, the prepared shape should allow for adequate obturation. These aims are commonly achieved by using rotary NiTi file systems with sodium hypochlorite[7]. A three-dimensional file that will adapt to the shape and size of the existing canal anatomy was developed recently and has demonstrated promising results[8].
Micro-computed tomography (MCT) has been commonly used to evaluate root canal shaping results in terms of the amount of hard tissue removed and the percentage of canal wall surface affected by the procedure[6],[7],[9]. Knowledge of the complex tooth internal anatomy and careful planning of an endodontic treatment are mandatory to reduce failure rates[10].
Schneider[11] emphasized that the root canal should present a flare shape, from apical to coronal, preserving the apical foramen and not altering the original canal curvature. The most appropriate canal shape for irrigation and filling with gutta-percha is a continuously tapering funnel shape with the smallest diameter at the end-point and the largest at the orifice[12]. Over the years, many techniques, instruments and devices have been described, but few appear capable of consistently producing the appropriate conical flared form demanded by modern obturation techniques. This problem is particularly important in narrow curved canals[13].
Several instrumentation techniques have been developed to make root canal preparation easier and more effective[14]–[16], especially after the development of nickel-titanium instruments. However, transportation of the apical foramen, creation of ledges, elbows, zips, perforations, and instrument fracture can occur along with loss of working length[14],[17],[18]. In the last decades, many new NiTi rotary instruments have been developed and introduced by various manufacturers. Most clinicians prefer these systems because of their advantages such as saving time[19] and better cutting efficiency[20]. Nevertheless, some functions of NiTi rotary systems such as cleaning ability, increased stress, and the inability to adequately prepare oval canals are still controversial. Additionally, Kim et al.[21] found a potential relationship between the design of NiTi instruments and the incidence of vertical root fractures. They concluded that file design affected apical stress and strain concentrations during root canal instrumentation.
Biomechanical studies are still needed to better understand the reasons for these fractures and to try to reduce or avoid them. In particular, studies analyzing the files' working conditions in terms of involved loads and displacements could be helpful in the assessment of the files' separation risks (by a comparison between the involved loads and the strength of the file). Different experimental set-ups and protocols have been proposed to study the forces developed during a root canal preparation on extracted teeth or synthetic blocks[22]–[26].
Rotary nickel-titanium (NiTi) instruments have become very popular because it has been shown that most of them seem to be safe to use when used according to the manufacturers' guidelines. They are able to enlarge root canals rapidly and are well suited for preparing even severely curved root canals[27]–[30]. Although the advantages of rotary NiTi rotaries are well accepted, the influence of the design of the cutting blades of these instruments is still controversial with regard to their efficiency and cleaning ability[3],[27],[28].
Nickel-titanium rotary instruments reduce procedural errors and the time required to finish root canal preparation. Another NiTi system was recently introduced by Dentsply Maillefer (Ballaigues, Switzerland) for the same purpose of creating an initial glide path mechanically. According to the manufacturer, the Path File is a system composed of 3 instruments with a square cross-section and .02 taper. The first file of the Path File sequence is recommended for use immediately after exploring the root canal with a #10 manual K-type file[30].
The methods commonly used for evaluating canal shaping are radiographs[31], tooth sections[32], and plastic blocks[33]. Microcomputed tomography (MCT) scanning, although a time- and money-consuming method[34], has major advantages. MCT scanning implements a small field of vision and, therefore, has a high resolution up to 4 mm, which is adequate for accurate evaluation of root canal preparations[25],[34]. Several methodologies have been proposed to assess the action of endodontic instruments on the canal walls. More recently, the use of computed tomography (CT) has been suggested for this purpose because it is a nondestructive method that allows measuring the amount of root dentin removed by endodontic instruments[35]. On the other hand, preparing to small apical dimensions is recommended for prevention of instrumentation errors such as apical transportation and also to preserve as much radicular dentin as possible[34]. The pre- and postoperative acquisitions of MCT scanning can be precisely superimposed to the nearest voxel so that volumes and areas can be easily computed and compared using customized computer software. MCT scanning is noninvasive and, therefore, multiple scans can be performed on the same specimen[36]. Furthermore, cone-beam computed tomography (CBCT) images permit nondestructive and metrically exact analyses of variables such as volume, surface areas, cross-sectional shape, and taper. The fraction of prepared surface can be analyzed with software which does not interfere in the original format of the images, allowing the analysis of the exact position and direction of canal transportation by CT scans obtained in voxel for three dimensional analyses[34].
Root canal shape can be challenging to the endodontist, especially in teeth with dilacerated roots which require caution in choosing the most appropriate endodontic instrument and instrumentation technique. In view of the above, the present study aimed to compare the effects of 3 different Nickel Titanium rotary instruments on the final shape and total amount of transportation of curved mesial root canals in extracted human mandibular molar teeth using CBCT.
MATERIALS AND METHODS
Sample preparation
A total of 42 recently extracted human mandibular molars were prepared to obtain 81 mesial root canals. The mandibular molars were obtained from Department of Oral Surgery of Cairo University. The selected root canals had curved canals ranging from 15° to 45°. The molar teeth were selected with the approval of the Ethics in Research Committee of the Center of Health Sciences of the University. Ethical clearance was obtained from the Ethical Committee of the Faculty of Oral and Dental Medicine of Cairo University. Molars were extracted for periodontal and prosthetic reasons. The mesial roots had to have completely formed apices and curved roots[37]. Tissue fragments and calcified debris were removed from the teeth by scaling. The samples were identified by random numbering from 1 to 81. The teeth were stored in 10% formalin solution.
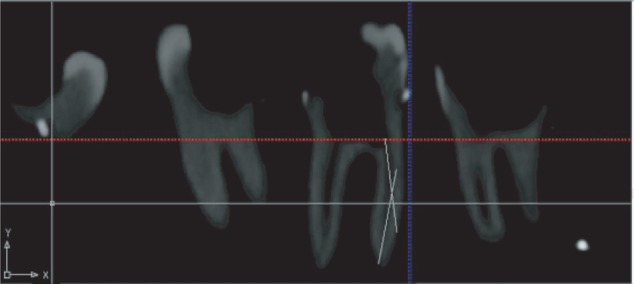
Preoperative periapical radiographs were used to inspect the mesial roots of fully-developed apices and to determine the angle of root curvature (Fig. 1). Teeth that had two canals in the mesial root with independent apical foramina and no calcifications or internal resorption were selected for the experiment. Root canals having the same foramen as well as S- or C-shaped canals or anastomosis between the canals were excluded[36].
Fig. 1. Method of determination of the canal curvature.
The coronal access was made using a #1016 round diamond bur (KG Sorensen, Sao Paulo, Brazil) under water spray cooling, high-speed hand-piece followed by the straight-line access of the walls with an Endo-Z bur (Dentsply Maillefer). To determine the working length, a size 10 K-file (Dentsply Maillefer) was inserted into the mesio-buccal and mesio-lingual canals until it was visible at the apical foramen. The working length of each canal was measured to be 1 mm less than the length measured[36].
Embedding of the specimens in acrylic resin blocks
Very small pieces of gutta percha were glued on the four surfaces of the tooth (mesial, distal, buccal, and lingual) at the level of the cemento-enamel junction. Small pieces of orthodontic wire were inserted at the periphery of acrylic resin for adjustment of scan orientation. The specimens were embedded in auto polymerizing acrylic resin (Acrostone, Dental & Medical Supplies, Cairo, Egypt) using a plastic mold. In order to prevent the resin from entering and polymerizing into the apical foramen, the apices of the roots were sealed with wax (Wilson, Sao Paulo, Brazil). Acrylic resin was mixed according to the manufacturer's instructions and poured into the mold. Each sample was inserted into the unset acrylic resin so that its long axis was parallel to the long axis of the mold to ensure standardization of the specimens for the tomography images before and after root canal instrumentation. The acrylic resin was allowed to set. The preoperative angle of curvature was measured according to Schneider technique using CBCT (Image J software 1.36b; National). The specimens were randomly divided into three groups with 27 root canals per group. The Protaper rotary system (Dentsply Maillefer) was used for group 1, the Revo- S rotary system (MicroMega, Besaçon) for group 2 and the Hero- Shaper rotary system (MicroMega, Besaçon) for group 3.
Root Canal Preparation
All canals were instrumented with crown-down methodology to the working length at a speed of 350 rpm and a torque-control by using an 8:1 reduction hand piece (X-Smart; DENTSPLY Tulsa Dental, Tulsa, OK). For irrigating the root canals, a freshly prepared 2.5% sodium hypochlorite solution was used with a 30 G needle (Max-i-Probe, Hawe-Neos, DENTSPLY, Bioggio, Switzerland). Irrigation was performed at the start of the instrumentation, between the changes of instrument, and at the end of the biomechanical preparation, by rinsing with 17% EDTA for one minute followed by a final NaOCl rinse after cleaning the mesial canals. In all groups, the instrument was lightly coated with an EDTA gel as a lubricant. All instruments were used to enlarge 2 canals only and then discarded.
The Pro-Taper Universal Rotary System
In the Pro-Taper group, Pro-Taper SX, S1 and S2 were used to flare the orifice, coronal and middle third of the root canals and to get straightline access. A glide path was established preparing the canals with K-file size 15 and size 20 to working length. Shaping of the canals was continued using S1, S2, F1, F2 and F3 to working length. Once the instrument had negotiated the root canal and had rotated freely, it was removed.
The Revo-S system
Shaper® & Cleaner 1(SC1) N° 25/0.06, L 21 mm, (SC2) N° 25/0.04, L 25 mm, Shaper® universal (SU) N° 25/0.06, L 25 mm. Apical Shaper® 30 N° 30 /0.06, L 25 mm. During preparation, the canals were assessed for patency and gross preparation errors, i.e., instrument fracture, perforation, ledge and loss of working length. These data were tabulated along with changes in canal curvature.
The Hero Shaper rotary system
The coronal two thirds of the root canal were instrumented with 20/0.06 file and 20, 25 and 30 files, with a 0.04 taper, were then used to prepare the canal to the working length.
CBCT
Initial CBCT images with 120 kVp by 120 kVp. and 46.72 mA were obtained before root canal preparation. The specimens were fitted into a Fox scale (Bio Art Equi-pamentos Odontológicos, São Carlos, SP, Brazil) and adapted to a Cone Beam I-Cat tomography. The images were captured in a small field of view (6 cm) with 40 s of exposure time and a matrix of 800×800 pixels. Xoran-Cat software was used (Imaging Sciences International. Hatfield, PA, USA) for image reconstruction, totaling 277 slices in the axial direction. Teeth were scanned before and post mechanical preparation with i-CAT CBCT scanner (Imaging Sciences International) with the following parameters: 120 kVp, 5 mA, exposure time 26 seconds, field of view 80 mm, and voxel size 0.125 mm (Fig. 2A).
Fig. 2. Cone beam computed tomography scanning.

A: Canal preparation pre and post instrumentation. B: The volumes of interest in the mesiobuccal and mesiolingual canal are shown as superimpositions of unprepared (green) and prepared (black) canal areas.
The measurements of the non-instrumented areas and the measurements after root canal preparation were done voxel by voxel, whereas M1 was the measurement of the quantity of voxels from the external surface of the mesial portion of the root to the mesial wall of the non-instrumented canal (Fig. 2B). M2 was the measurement of the quantity of voxels from the external root surface of the mesial portion of the root to the wall of the canal after instrumentation. D1 was the measurement of the quantity of voxels of the external surface of the distal portion of the root to the distal wall of the no instrumented canal. D2 was the measurement of the quantity of voxels from the external surface of the distal portion of the root to the distal surface of the canal after instrumentation. Canal transportation (CT) was calculated from the following equation[38]:
 |
Regarding transportation direction, CT equal to 0 (zero) meant lack of transportation; a negative value represented transportation to the distal direction, and a positive value transportation towards the mesial direction. Centralization ability ratio was calculated using the values obtained during the measurement of transportation for both methods with the equation[50]:
 |
This equation was chosen according to the numerator value, which was always the lowest result obtained by the differences. A result equal to 1.0 µm indicated perfect centralization. When this value was closer to zero, it was considered that the instrument had a lower capacity to maintain itself in the central axis of the canal. In order to standardize images, orientation of teeth was done in the three orthogonal planes (the coronal, sagittal, and axial plane), gutta percha pieces were used as a reference to fix the selected cuts and window level and window width were also fixed.
Assessment of root canal preparation
Root canal preparations were completed by one operator, while the assessment of the canal curvatures prior to and after instrumentation was carried out by a second examiner who was blind about all experimental groups. For working safety, the number of fractured instruments during instrumentation was documented.
Shaping ability
Based on the canal curvatures assessed before and after instrumentation, canal straightening was determined as the difference between canal curvature prior to and after instrumentation. Root curvature was done on the sagittal cuts (the mesio-distal curvature) in mesio-buccal and mesio-ligual canals.
Measurement of dentin thickness and surface area
Dentin thickness was measured on the axial cuts from the periphery of the pulp space to the outer surface of the tooth in the four directions at the three levels (cervical, middle, and apical). The distances from the canal wall to the root surface at the first 3 cut-planes at the coronal level (below the orifice of the mesiobuccal canal) were measured at the buccal, mesial, lingual and distal dentin sides of each root by image analysis software. For measurement of dentin surface area, from the axial images, the ratio between the canal surface area and the root surface area were determined before and after preparation at 3 levels (cervical-middle-apical). The volume of prepared root canals was analyzed by using Software: SimPlant, Materialize Dental, Belgium. Volumetric method by tracing the canal outline at 14 different horizontal cut-planes, the volume was then automatically calculated. The volume of dentin removed was determined for each canal by subtracting the preinstrumentd canal volume from the instrumented canal volume. The volume of each root canal was determined in cubic centimeters.
Statistical analysis
Data were presented as mean and standard deviation (SD) values. Data showed non-normal (non-parametric) distribution so that Kruskal-Wallis test was used to compare the three systems. Mann-Whitney U test was used for pair-wise comparisons between the systems when Kruskal-Wallis test was significant. The significance level was set at P≤0.05. Statistical analysis was performed with the IBM® SPSS® Statistics Version 20 for Windows.
RESULTS
Changes in canal curvature and canal transportation
Table 1 shows no statistically significant difference among the ProTaper Universal Rotary System, HERO Shaper rotary system, and REVO- S rotary system (P≥0.05). Furthermore, there was no statistically significant difference in bucco-lingual canal transportation using the three systems at the cervical, middle and apical levels (P = 0.757, 0.573 and 0.577, respectively) (Table 2). Additionally, there was no statistically significant difference between mesio-distal canal transportation using the three systems at the cervical, middle and apical levels (P = 0.111, 0.401 and 0.986, respectively) (Table 2).
Table 1. Degree of straightening by the three systems.
| Protaper Revo-S (n = 27) | Revo-S (n = 27) | Hero Shaper (n = 27) | |
| Mean | 4.07 ± 2.53 | 3.22 ± 2.38 | 2.81 ± 1.14 |
| P-value | 0.226 |
Table 2. Mean and standard deviations of transportation of the three systems.
| Transportation | Protaper Revo-S (n = 27) | Revo-S (n = 27) | Hero shaper (n = 27) | P-value (n = 27) |
| Bucco-lingual canal | ||||
| Cervical | 0.11 ± 0.13 | 0.12 ± 0.09 | 0.12 ± 0.10 | 0.757 |
| Middle | 0.12 ± 0.14 | 0.12 ± 0.10 | 0.14 ± 0.11 | 0.573 |
| Apical | 0.15 ± 0.14 | 0.11 ± 0.11 | 0.11 ± 0.08 | 0.577 |
| Mesio-distal canal | ||||
| Cervical | 0.12 ± 0.12 | 0.19 ± 0.15 | 0.16 ± 0.14 | 0.111 |
| Middle | 0.14 ± 0.11 | 0.14 ± 0.22 | 0.13 ± 0.12 | 0.401 |
| Apical | 0.11 ± 0.12 | 0.10 ± 0.10 | 0.12 ± 0.13 | 0.986 |
Centering ratio
There was no statistically significant difference in the degree of straightening between bucco-lingual centering ratio after using the 3 systems at the cervical, middle and apical levels (P-value = 0.760, 0.175 and 0.804, respectively) Table 3. Also, there was no statistically significant difference between mesio-distal centering ratio after using the three systems at the cervical, middle and apical levels (P-value = 0.317, 0.313 and 0.213, respectively) Table 3.
Table 3. Mean and standard deviations of the centering ratio of the three systems.
| Centering | Protaper Revo-S (n = 27) | Revo-S (n = 27) | Hero shaper (n = 27) | P-value |
| Bucco-lingual centering rate | ||||
| Cervical | 0.09 ± 0.24 | 0.19 ± 0.34 | 0.15 ± 0.27 | 0.760 |
| Middle | 0.48 ± 0.41 | 0.28 ± 0.38 | 0.38 ± 0.38 | 0.175 |
| Apical | 0.42 ± 0.36 | 0.51 ± 0.54 | 0.47 ± 0.35 | 0.804 |
| Mesio-distal centering rate | ||||
| Cervical | 0.24 ± 0.37 | 0.33 ± 0.38 | 0.18 ± 0.31 | 0.317 |
| Middle | 0.34 ± 0.40 | 0.49 ± 0.43 | 0.44 ± 0.43 | 0.313 |
| Apical | 0.52 ± 0.43 | 0.32 ± 0.41 | 0.43 ± 0.41 | 0.213 |
Ratio of the canal area to the root area
Pre-preparation
There was no statistically significant difference between ratios of the canal area to the root area after the 3 systems were used at the cervical and middle levels (P-value = 0.076 and 0.600, respectively) (Table 4). At the apical level, there was a statistically significant difference among the systems (P= 0.014); pair-wise comparisons among the systems revealed that Hero Shaper showed the highest mean ratio, which was also statistically significant. There was no statistically significant difference between Protaper and Revo-S systems; both showed the statistically significant lowest mean ratios (Table 4).
Table 4. Mean and standard deviations of the centering ratio of the three systems.
| Ratio of the canal area value to the root area | Protaper Revo-S (n = 27) | Revo-S (n = 27) | Hero Shaper (n = 27) | P-value |
| Pre-preparation | ||||
| Cervical | 0.019 ± 0.01 | 0.024 ± 0.02 | 0.028 ± 0.02 | 0.076 |
| Middle | 0.021 ± 0.01 | 0.021 ± 0.02 | 0.022 ± 0.01 | 0.600 |
| Apical | 0.023 ± 0.01 | 0.016 ± 0.01* | 0.021 ± 0.005* | 0.014 |
| Post-preparation | ||||
| Cervical | 0.025 ± 0.01* | 0.038 ± 0.02* | 0.041 ± 0.03* | 0.014 |
| Middle | 0.032 ± 0.02 | 0.036 ± 0.02 | 0.031 ± 0.01 | 0.859 |
| Apical | 0.035 ± 0.01 | 0.032 ± 0.01 | 0.032 ± 0.01 | 0.549 |
| Ratio of canal area to root area (Post/Pre) | ||||
| Cervical | 1.44 ± 0.49* | 1.78 ± 0.58* | 1.57 ± 0.46* | 0.047 |
| Middle | 1.78 ± 0.74 | 1.93 ± 0.68 | 1.48 ± 0.50 | 0.058 |
| Apical | 1.62 ± 0.52* | 2.61 ± 1.52* | 1.50 ± 0.44* | 0.004 |
*P ≤0.05.
Post-preparation
At the cervical level, there was a statistically significant difference among the systems (P = 0.014); pair-wise comparisons among the systems revealed that there was no statistically significant difference between Revo-S and Hero Shaper; both showed the statistically significant highest mean ratios. Protaper showed the statistically significant lowest mean ratio (Table 4). There was no statistically significant difference in the ratios after the 3 systems were used at the middle and apical levels (P= 0.859 and 0.546, respectively) (Table 4).
Post preparation /Pre preparation
At the cervical and apical levels, there was statistically significant difference between the systems (P = 0.047 and 0.004, respectively); pair-wise comparisons between the systems revealed that Revo-S showed statistically significant highest mean ratio. There was no statistically significant difference between Protaper and Hero Shaper; both showed the statistically significant lowest mean ratios (Table 4). There was no statistical significant difference between ratios after the 3 systems were used at the middle level (P-value = 0.058) (Table 4).
DISCUSSION
One of the main goals of root canal preparation is to increase the canal's apical-to-cervical taper while maintaining its original overall shape[48]. A number of procedural errors, such as apical transportation, may occur during the shaping of curved canals[46]. To investigate the efficiency of the instruments and techniques developed for root canal preparation, a number of methods have been used to compare canal shape before and after preparation. One such method is digital radiographic imaging[7],[43]. Given the complex root canal anatomy and the variability in dentin hardness, the use of extracted teeth compromises standardization to a certain extent, but, more importantly, using extracted human teeth provides conditions close to the clinical situation[29],[34]. In endodontic therapy, the quality and quantity of information obtained from radiographic examinations are very important because they affect the diagnosis, treatment planning and prognostic stability. Radiological examination is an essential part of the diagnosis and management of endodontic disease. At present, radiological examination is usually limited to two-dimensional periapical images. Crucially, essential information of the three-dimensional anatomy of the tooth/teeth and adjacent anatomy is not visible, even with the best intentions and paralleling techniques. CBCT should provide an effective and safe way to overcome some of these problems and may, in time, change the way in which the outcome of endodontic treatment is assessed[39]. The use of CT provides additional, beneficial information not available from dental radiographs for treatment planning in apical surgery of mandibular premolars and molars. When the mandibular canal cannot be detected in dental radiographs, or is in close proximity to the lesion or root apex, CT should be considered before endodontic surgery. The presence, extent, and location of the lesion and its relation to the mandibular canal can be predictably evaluated in a CT scan of the area[40].
CBCT allows detailed three-dimensional (3D) observation of those forms and shapes, and its usefulness in endodontic therapy has been reported[21]. The advent of new strategies for root canal preparation and evaluation of the quality of the outcome has modified the perception of instrumentation and the operator's skills. CBCT has been used in endodontic therapy for the study of root canal anatomy, evaluation of root canal preparation and filling, retreatment, and experimental endodontics. CBCT images provide a significantly faster image acquisition and reconstruction scheme, offering high-resolution images that allow more accurate identification of apical periodontitis than periapical radiographs[41],[42].
Numerous in vitro and in vivo experiments have already demonstrated improved canal shapes with NiTi rotary instruments, even though it is not clear whether this correlates to improved clinical outcomes. On the basis of the results of this study, it seems reasonable to recommend the use of NiTi rotary instruments, for example, GT or ProTaper files, in the pre-doctoral clinical setting[43].
CBCT imaging modalities is an effective technique to evaluate and measure dentin thickness, canal curvature, apical transportation, and canal centering, as it provides images in orthogonal planes as well as in oblique planes. If we consider the low radiation dose, fast scan, sub-millimetric resolution, and interactive software that allow re-orientation of the scan according to the inclination of each tooth, it will be an incredible tool in endodontic evaluation in the future[10],[43]. In the present study, CBCT images permitted observations of the root canal in 3D planes (the axial, transverse and tangent planes). The axial slice from CBCT images constituted an important tool to identify root curvatures and canal transportation[44].
Various studies investigated rotary root canal preparations versus manual preparation. They concluded that NiTi maintained original canal shape better than stainless steel files[3],[7],[13],[16],[21]. Therefore, in this study, we made comparisons only between the rotary systems. Similar apical preparation diameters are required for the comparison of the shaping and cleaning ability of different root canal instruments[22],[23],[25],[26]. Thus, in all investigated groups in the present investigation, the final apical preparation diameter was size 30. Moreover, to reduce the wide range of variations in 3D root canal configuration, the present study used mesial root canals of the first and second mandibular molars. These teeth reveal root canal curvatures in most cases. Consequently, the measured degrees of the root canal curvature were categorized into three groups according to a modified method described by Schneider[11]; this matched-group design allowed for minimization of high variations in the degree of curvature between the groups.
El Ayout et al.[36] concluded that increased apical enlargement of curved canals did not result in a complete apical preparation, whereas it did lead to unnecessary removal of dentin. A 30-G needle used for irrigation is most effective in removing debris in the apical one-third of canals, and, thus, it has been suggested that the minimum apical size of a prepared canal should be an International Standard Organization #30 in order to allow proper chemo-mechanical cleansing of the canals with irrigants. In the present study, 3 systems with different taper/flexibility were used. None of the instrumentation systems was able to completely prepare the canal at the apex, and the more rigid the instrument was, the more dentin was unnecessarily removed.
The NiTi files used in this study were designed to improve various aspects of the properties required for root canal preparation instruments, including less canal transportation, less instrument separation and fewer procedural steps. However, few articles in the literature studied the effect of Revo-s on the final shape of the curved canal. All tested NiTi instruments had in common the triangular cross-section geometry with different designs in each group. This similarity in results may be attributed to the similar cross-section geometry of tested NiTi instruments. The lowest defect number was seen in the RS group. A literature search did not reveal any previous studies regarding this file system. However, manufacturers suggest that RS provides less stress on the instrument because of the asymmetrical cross-section and the extended cutting part in the coronal region, which increases instrument flexibility[45].
In most studies the straightening effect has been radiographically analyzed in the bucco-lingual direction only[27]. Limited data are available about 3D morphological changes during preparation. The pre- and postoperative acquisitions of MCT scanning can be precisely superimposed to the nearest voxel so that volumes and areas can be easily computed and compared using customized computer software. MCT scanning is noninvasive, and, therefore, multiple scans can be performed on the same specimen[46]. A difficult variable to control in any study using human teeth is the wide variation in canal morphology[45]. In this study, a quantitative analysis was performed through observation of changes between pre-instrumentation and post-instrumentation curvature. Previous studies demonstrated the reliability of the experimental method used and its effectiveness in representing changes in canal curvature and in extrapolating the results[20],[30].
Because dentin is a dense and resilient material, instruments with a positive rake angle actually work like a shaver on the dentin surface. In contrast, instruments that have a negative rake angle are less efficient and require more energy to cut dentin[47],[48]. Câmara et al.[49] studied the cutting efficiency of the Hero Shaper and recommended further studies to evaluate canal transportation, which is another important aspect that needs to be clarified. The fact that an instrument is able to cut efficiently does not mean that it will shape the root canal accordingly. The frequent use of curved canals as specimens in research can possibly be explained by the fact that these canals pose a greater challenge to instrumentation. This difficulty has been correlated with the observation of performance differences between different instrument systems. Furthermore, the evaluation of changes in canal curvatures after instrumentation has been widely used to assess the tendency of a given technique or of the mechanical properties of a certain instrument to maintain the original anatomy of the canal or rectify its curvatures[49].
In the present study, ProTaper NiTi rotary instruments were used, and the canals were enlarged to F3 at WL, corresponding to a size 30 taper master file. Zhang et al.[50] stated that the shaping files of ProTaper have an increasing taper (from 3.5 % at D to 19 % at D. The super-elasticity of the instrument safely flares the coronal part of the canal without transportation. The specimens were selected, on the basis of having a moderate curvature. The frequency of procedural errors was low, with no impact created by the level of experience and knowledge of the operators[44].
With regard to our study on extracted teeth, the amount of dentin removed by Pro-Taper was statistically significantly greater than that by Hero Shaper, which is in agreement with Bergmans et al.[51], but the amount of dentin removed by Pro-Taper was measurably greater than that reported in the study by Peters et al.[52], presumably because of the last instrument used. Those researchers finished their instrumentation with the file F2, whereas the last file used in this study was F3. Although it is known that even F1 can be sufficient for apical preparation of curved canals, the reasoning behind use of all files for Pro-Taper in the present study was to achieve the same apical enlargement with all tested instruments, thereby enabling comparisons.
The comparison of the pre- and postoperative photographs of root canal cross-sections enables conclusions on shaping ability as well as mechanical cleaning ability. The prepared root canal should include the original root canal dimensions and no unprepared areas should remain. In the present investigation, analysis of the pre- and postoperative cross-sections showed that the manual technique using stainless steel instruments as well as the rotary NiTi systems left uninstrumented root canal walls in all regions. While the coronal and middle cross-sections demonstrated sufficient shaping outcomes with only minor untreated areas, the percentage of uninstrumented root canal walls in the apical cross-section was significantly affected by the instrumentation system.
In conclusion, within the limitations of this in vitro study, it can be concluded that all instruments in this study maintained the original canal curvature well with no significant differences between the different files. During preparation there was failure of only one file, which was in the protaper group.
References
- 1.Bystrom A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Inter Endodont J. 1985;18:35–40. doi: 10.1111/j.1365-2591.1985.tb00416.x. [DOI] [PubMed] [Google Scholar]
- 2.Gulabivala K, Ng YL, Gilbertson M, Eames I. The fluid mechanics of root canal irrigation. Physiol Meas. 2010;31:R49–84. doi: 10.1088/0967-3334/31/12/R01. [DOI] [PubMed] [Google Scholar]
- 3.Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endodont. 2004;30:559–67. doi: 10.1097/01.don.0000129039.59003.9d. [DOI] [PubMed] [Google Scholar]
- 4.Adcock W, Trout NA, Vercoe D, Taylor DK, Shiner VJ, Jr, Sorensen TS. Solvolysis of (Z)-5-trimethylstannyl 2- adamantly p-bromobenzenesulfonate: mechanistic implications of a record-breaking secondary alpha-deuterium kinetic isotope effect for an SN1 substrate. J Org Chem. 2003;68:5399–402. doi: 10.1021/jo0300892. [DOI] [PubMed] [Google Scholar]
- 5.De-Deus G, Souza EM, Barino B, et al. The self-adjusting file optimizes debridement quality in oval-shaped root canals. J Endodont. 2011;37:701–5. doi: 10.1016/j.joen.2011.02.001. [DOI] [PubMed] [Google Scholar]
- 6.Peters OA, Paque F. Root canal preparation of maxillary molars with the self-adjusting file: a micro-computed tomography study. J Endodont. 2011;37:53–7. doi: 10.1016/j.joen.2010.08.047. [DOI] [PubMed] [Google Scholar]
- 7.Paqué F, Al-Jadaa1 A, Kfir A. Hard-tissue debris accumulation created by conventional rotary versus self-adjusting file instrumentation in mesial root canal systems of mandibular molars. Inter Endodont J. 2012;45:413–8. doi: 10.1111/j.1365-2591.2011.01991.x. [DOI] [PubMed] [Google Scholar]
- 8.Hof R, Perevalov V, Eltanani M, Zary R, Metzger Z. The self-adjusting file (SAF). Part 2: mechanical analysis. J Endodont. 2010;36:691–6. doi: 10.1016/j.joen.2009.12.028. [DOI] [PubMed] [Google Scholar]
- 9.Versiani MA, Pecora JD, de Sousa-Neto MD. Flat-oval root canal preparation with Self-adjusting File instrument: a micro-computed tomography study. J Endodont. 2011;37:1002–7. doi: 10.1016/j.joen.2011.03.017. [DOI] [PubMed] [Google Scholar]
- 10.Estrela C, Bueno MR, Sousa-Neto MD, P-cora JD. Method for Determination of Root Curvature Radius Using Cone-Beam Computed Tomography Images. Braz Dent J. 2008;19:114–8. doi: 10.1590/s0103-64402008000200005. [DOI] [PubMed] [Google Scholar]
- 11.Schneider W. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32:271–5. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- 12.Schilder H, Yee FS. Canal debridement and disinfection. In: Cohen S, Burns RC, editors. Pathways of the pulp. St. Louis: The CV Mosby Company; 1984. p. 175. [Google Scholar]
- 13.Thompson SA, Dummer PMH. Shaping ability of ProFile .04 Taper Series 29 rotary nickel-titanium instruments in simulated root canals. Part 2. Int Endod J. 1997;30:8–15. doi: 10.1111/j.1365-2591.1997.tb01092.x. [DOI] [PubMed] [Google Scholar]
- 14.Lopes HP, Moreira EJL, Elias CN, Almeida RA, Neves MS. Cyclic fatigue of protaper instruments. J Endod. 2008;33:55–7. doi: 10.1016/j.joen.2006.09.003. [DOI] [PubMed] [Google Scholar]
- 15.Pécora JD, Capelli A, Guerisoli DMZ, Spanó JCE, Estrela C. Influence of cervical preflaring on apical file size determination. Int Endod J. 2005;38:430–5. doi: 10.1111/j.1365-2591.2005.00946.x. [DOI] [PubMed] [Google Scholar]
- 16.Schäfer E, Florek H. Efficiency of rotary nickel-titanium K3 instruments compared with stainless steel hand K-Flexo-file. Part 1. Shaping ability in simulated curved canals. Int Endod J. 2003;36:199–207. doi: 10.1046/j.1365-2591.2003.00643.x. [DOI] [PubMed] [Google Scholar]
- 17.Cimis GM, Boyler TF, Pelleu GR., Jr Effect of three files studies of canal curvatures in the mesial roots of mandibular molars. J Endod. 1988;14:441–4. [Google Scholar]
- 18.Hülsmann M, Schade M, Schäfers F. A comparative study of root canal preparation with Hero 642 and Quantec SC rotary Ni-Ti instruments. Int Endod J. 2001;34:538–46. doi: 10.1046/j.1365-2591.2001.00431.x. [DOI] [PubMed] [Google Scholar]
- 19.Vaudt J, Bitter K, Neumann K, Kielbassa AM. Ex vivo study on root canal instrumentation of two rotary nickel-titanium systems in comparison to stainless steel hand instruments. Int Endod J. 2009;42:22–33. doi: 10.1111/j.1365-2591.2008.01489.x. [DOI] [PubMed] [Google Scholar]
- 20.Schäfer E, Lau R. Comparison of cutting efficiency and instrumentation of curved canals with nickel-titanium and stainless-steel instruments. J Endod. 1999;25:427–30. doi: 10.1016/S0099-2399(99)80272-6. [DOI] [PubMed] [Google Scholar]
- 21.Kim HC, Lee MH, Yum J, Versluis A, Lee CJ, Kim BM. Potential relationship between design of nickel-titanium rotary instruments and vertical root fracture. J Endod. 2010;36:1195–9. doi: 10.1016/j.joen.2010.02.010. [DOI] [PubMed] [Google Scholar]
- 22.Sattapan B, Palamara JEA, Messer HH. Torque during canal instrumentation using rotary nickel-titanium files. J Endod. 2000;26:156–60. doi: 10.1097/00004770-200003000-00007. [DOI] [PubMed] [Google Scholar]
- 23.Boessler C, Peters OA, Zehnder M. Impact of lubricant parameters on rotary instrument torque and force. J Endod. 2007;33:280–3. doi: 10.1016/j.joen.2006.11.007. [DOI] [PubMed] [Google Scholar]
- 24.Da Silva FM, Kobayashi C, Suda H. Analysis of forces developed during mechanical preparation of extracted teeth using RaCe rotary instruments and ProFiles. Int Endod J. 2005;38:17–21. doi: 10.1111/j.1365-2591.2004.00890.x. [DOI] [PubMed] [Google Scholar]
- 25.Peters OA, Peters CI, Schö Neuberger K, et al. ProTaper rotary root canal preparation: assessment of torque and force in relation to canal anatomy. Int Endod J. 2003;36:93–9. doi: 10.1046/j.1365-2591.2003.00628.x. [DOI] [PubMed] [Google Scholar]
- 26.Blum JY, Machtou P, Ruddle C, et al. Analysis of mechanical preparations in extracted teeth using proTaper rotary instruments: value of the safety quotient. J Endod. 2003;29:567–75. doi: 10.1097/00004770-200309000-00007. [DOI] [PubMed] [Google Scholar]
- 27.Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J. 2006;39:203–12. doi: 10.1111/j.1365-2591.2006.01075.x. [DOI] [PubMed] [Google Scholar]
- 28.Rödig T, H-lsmann M, Kahlmeier C. Comparison of root canal preparation with two rotary NiTi instruments: ProFile .04 and GT Rotary. Int Endod J. 2007;40:553–62. doi: 10.1111/j.1365-2591.2007.01270.x. [DOI] [PubMed] [Google Scholar]
- 29.Hülsmann M, Peters O, Dummer PMH. Mechanical preparation of root canals. Shaping goals, techniques and means. Endod Topics. 2005;10:30–76. [Google Scholar]
- 30.Alves Vde O, Bueno CE, Cunha RS, Pinheiro SL, Fontana CE, de Martin AS. Comparison among Manual Instruments and Path File and Mtwo Rotary Instruments to Create a Glide Path in the Root Canal Preparation of Curved Canals. J Endod. 2012;38:117–20. doi: 10.1016/j.joen.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 31.Southard DW, Oswald RJ, Natkin E. Instrumentation of curved molar root canals with the Roane technique. J Endod. 1987;13:479–89. doi: 10.1016/S0099-2399(87)80015-8. [DOI] [PubMed] [Google Scholar]
- 32.Bramante CM, Berbert A, Borges RP. A methodology for evaluation of root canal instrumentation. J Endod. 1987;13:243–5. doi: 10.1016/S0099-2399(87)80099-7. [DOI] [PubMed] [Google Scholar]
- 33.Weine FS, Kelly RF, Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975;1:255–62. doi: 10.1016/S0099-2399(75)80037-9. [DOI] [PubMed] [Google Scholar]
- 34.Pique F, Ganahl D, Peters OA. Effects of root canal preparation on apical geometry assessed by micro-computed tomography. J Endod. 2009;35:1056–9. doi: 10.1016/j.joen.2009.04.020. [DOI] [PubMed] [Google Scholar]
- 35.Hartmann MSM, Barletta FB, Fontanella VRC, Vanni JR. Canal transportation after root canal instrumentation: a comparative study with computed tomography. J Endod. 2007;33:962–5. doi: 10.1016/j.joen.2007.03.019. [DOI] [PubMed] [Google Scholar]
- 36.El Ayouti A, Dima E, Judenhofer L-st C, Pichler BJ. Increased Apical Enlargement Contributes to Excessive Dentin Removal in Curved Root Canals: A Stepwise Microcomputed Tomography Study. J Endod. 2011;37:1580–4. doi: 10.1016/j.joen.2011.08.019. [DOI] [PubMed] [Google Scholar]
- 37.Câmara AC, Aguiar CM, de Figueiredo JA. Evaluation of the root dentine cutting effectiveness of the HERO 642, HERO Apical and HERO Shaper rotary systems. Aust Endod J. 2008;34:94–100. doi: 10.1111/j.1747-4477.2007.00086.x. [DOI] [PubMed] [Google Scholar]
- 38.Gambill M, Alder M, Del Rio E. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369–75. doi: 10.1016/S0099-2399(96)80221-4. [DOI] [PubMed] [Google Scholar]
- 39.Patel S, Dawood A, Pitt Ford T. The potential applications of cone beam computed tomography in the management of endodontic problems. Inter Endod J. 2007;40:818–30. doi: 10.1111/j.1365-2591.2007.01299.x. [DOI] [PubMed] [Google Scholar]
- 40.Velvart P, Hecker H, Tillinger G. Detection of the apical lesion and the mandibular canal in conventional radiography and computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:682–8. doi: 10.1067/moe.2001.118904. [DOI] [PubMed] [Google Scholar]
- 41.Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007;33:1121–32. doi: 10.1016/j.joen.2007.06.011. [DOI] [PubMed] [Google Scholar]
- 42.Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod. 2008;34:273–9. doi: 10.1016/j.joen.2007.11.023. [DOI] [PubMed] [Google Scholar]
- 43.Gekelman D, Ramamurthy R, Mirfarsi S, Peters OA. Rotary Nickel-Titanium GT and ProTaper Files for Root Canal Shaping by Novice Operators: A Radiographic and Micro-Computed Tomography Evaluation. J Endod. 2009:35. doi: 10.1016/j.joen.2009.07.018. [DOI] [PubMed] [Google Scholar]
- 44.de Alencar AHG, Dummer PMH, Oliveira HCM, Pécora JD, Estrela C. Procedural Errors During Root Canal Preparation Using Rotary NiTi Instruments Detected by Periapical Radiography and Cone Beam Computed Tomography. Braz Dent J. 2010;21:543–9. doi: 10.1590/s0103-64402010000600011. [DOI] [PubMed] [Google Scholar]
- 45.Versü mer J, Hü lsmann M, Schä fer F. A comparative study of root canal preparation using ProFile .04 and Light speed rotary Ni-Ti instruments. Int Endod J. 2002;35:37–46. doi: 10.1046/j.1365-2591.2002.00454.x. [DOI] [PubMed] [Google Scholar]
- 46.El Batouty KM, Elmallah WE. Comparison of Canal Transportation and Changes in Canal Curvature of Two Nickel-Titanium Rotary Instruments. J Endod. 2011;37:1290–2. doi: 10.1016/j.joen.2011.05.024. [DOI] [PubMed] [Google Scholar]
- 47.Himel T, McSpadden J, Goodis E. Instrument, materials and devices. In: Cohen S, Hargreaves K, Keiser K, editors. Pathways of the pulp. 9th ed. St Louis: Mosby; 2006. pp. 233–89. [Google Scholar]
- 48.Jeon S, Spangberg W, Yoon C, Kazemi B, Kum Y. Smear layer production by 3 rotary reamers with different cutting blade designs in straight root canals: a scanning electron microscopic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:601–7. doi: 10.1016/s1079-2104(03)00303-2. [DOI] [PubMed] [Google Scholar]
- 49.Gergi R, Rjeily JA, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J Endod. 2010;36:904–7. doi: 10.1016/j.joen.2009.12.038. [DOI] [PubMed] [Google Scholar]
- 50.Zhang L, Luo HX, Zhou XD, Tan H, Huang DM. The shaping effect of the combination32-of two rotary nickel-titanium instruments in simulated S-shaped canals. J Endod. 2008;34:456–8. doi: 10.1016/j.joen.2008.01.007. [DOI] [PubMed] [Google Scholar]
- 51.Bergmans L, Van Cleynenbreugel J, Wevers M, Lambrechts P. Mechanical root canal preparation with NiTi rotary instruments: rationale, performance and safety: status report for the American Journal of Dentistry. Am J Dent. 2001;14:324–38. [PubMed] [Google Scholar]
- 52.Peters OA, Laib A, Gohring TN, Barbakow F. Changes in root canal geometry after preparation assessed by high-resolution computed tomography. J Endod. 2001;27:1–6. doi: 10.1097/00004770-200101000-00001. [DOI] [PubMed] [Google Scholar]