

Abstract
Introduction:
Orthodontic treatment is based on the principle that if prolonged pressure is applied to the tooth, tooth movement will occur as the bone around the tooth re-models. In this study osteotomy of buccal alveolar plate and undermining of interseptal bone was performed at premolar extraction site and rate of en-masse retraction and canine retraction was evaluated.
Materials and Methods:
Patients between the age of 18 and 25 years, requiring retraction of anterior teeth are selected for the study. Osteotomy with undermining of interseptal bone at the extraction site was performed. The procedure was performed on all four quadrants.
Results:
The average retraction in the maxillary arch was 0.98 mm/quadrant in 3 weeks, i.e., a total retraction of 5.89 mm in a span of 9 weeks. The average retraction in the mandibular arch was 0.96 mm/quadrant in 3 weeks, i.e., a total retraction of 5.75 mm in a span of 9 weeks.
Conclusion:
This method of achieving faster en masse retraction immediately after extraction definitely reduced the initial retraction time. We recommend that such procedure must be carried out with appropriate anchorage conservation methods.
Keywords: Adjunctive surgery, corticotomy, retraction
Orthodontic treatment is based on the principle that if prolonged pressure is applied to the tooth, tooth movement will occur as the bone around the tooth re-models. Patients who seek orthodontic treatment often desire that their treatment be completed in a short period of time. Many methods were tried to reduce the overall treatment time which included various surgical procedures.
Liou and Huang[1] performed rapid canine retraction through distraction of the periodontal ligament. Periodontal distraction was performed using a distraction device. Complete canine retraction was done in 3 weeks with minimal root resorption, but the distraction device was bulky and cumbersome and had poor patient acceptability.
In this study osteotomy of buccal alveolar plate and undermining of interseptal bone was performed at premolar extraction site and rate of en-masse retraction and canine retraction was evaluated.
This study is an attempt to find the effectiveness of this procedure in anterior retraction using the Preadjusted edgewise appliance (PEA) appliance.
Surgical procedure
Incisions were placed at the region of the premolar to be extracted. One crevicular incision was made in relation to the premolar intended to be extracted. Vertical incision was placed to aid in the reflection of the flap to expose the cortical bone covering the tooth at the cervical region of the tooth. Finally undermining of interseptal bone was done at mesial wall of alveolar socket [1–3].
Figure 1.

Crevicular incision to expose the alveolar bone
Figure 3.

Undermining of interseptal bone
Figure 2.

Osteotomy cuts placed
Materials and Methods
Patients between the age of 18 and 25 years, requiring retraction of anterior teeth are selected for the study. Osteotomy with undermining of interseptal bone at the extraction site was performed. The procedure was performed on all four quadrants.
Intra oral periapical radiographs of the upper and lower first premolar regions of both right and left sides were taken to assess adequate availability of cortical bone and root anatomy.
Initial measurements were done after extraction using a vernier caliper at point zero. The same procedure was performed in all four quadrants. In the mandibular arch, the vertical cuts was extended 3-4 mm from the apex of the premolar roots due the proximity of the premolar roots to the mental foramen. By doing this damage to the mental nerves and vessels is prevented. The retraction of the anterior teeth (en masse) was started immediately after extraction. In group 1 en-masse retraction was carried out using 200 g Nickel - titanium (Ni - Ti) springs in. In group 2 retraction was carried out using elastomeric chains. A force of 400 g was applied. In group 3 en-masse retraction was carried out using active tie backs in all four quadrants.
The distance between the contact point of the canine and the second premolar is measured at 3 week intervals until the 9th week with a vernier calliper to measure the amount of retraction. These intervals are termed as were termed as T1, T2 and T3.
Results
Data was analyzed using Repeated Measures ANOVA, paired t-test for overall data. Kruskal Wallis test was used to compare mean retraction between groups. SPSS version 17 and excel was used to analyze the data. P < 0.05 was considered to be significant.
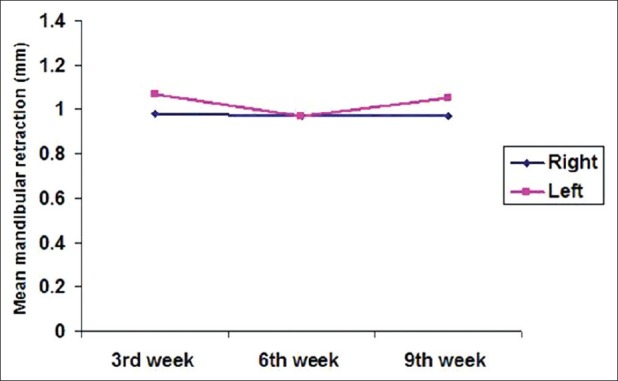
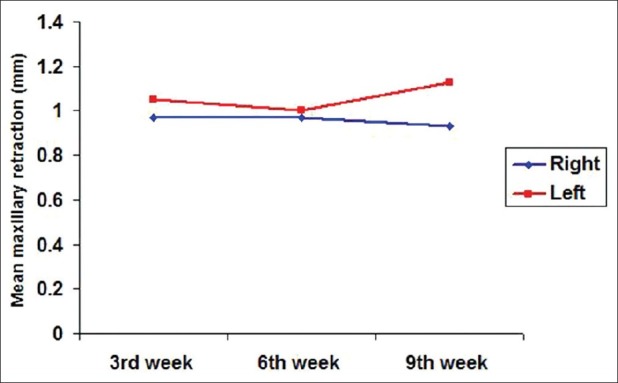
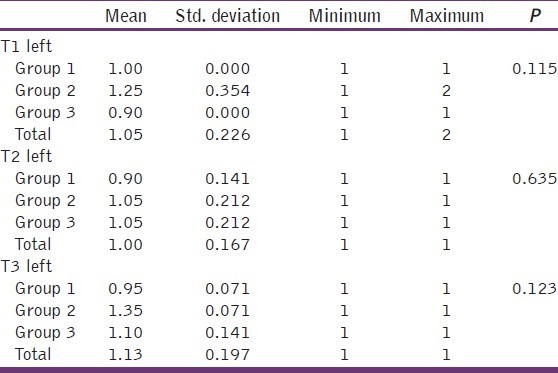
The average retraction in the maxillary arch was 0.98 mm/quadrant in 3 weeks, i.e., a total retraction of 5.89 mm in a span of 9 weeks. The average retraction in the mandibular arch was 0.96 mm/quadrant in 3 weeks, i.e., a total retraction of 5.75 mm in a span of 9 weeks. The retraction on the left side was more when compared to the retraction on the right side as shown in Figures 4 and 5 [Table 1–3].
Figure 4.
Mean retraction in the maxillary arch
Figure 5.
Mean retraction in the mandibular arch
Table 1.
Comparison of retraction between groups in the maxillary arch (right side) at various intervals
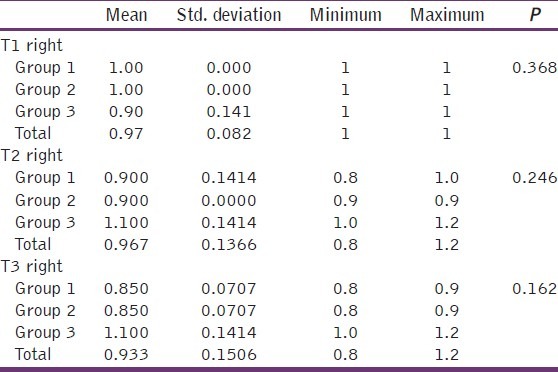
Table 3.
Mean anchor loss in maxillary and mandibular arch
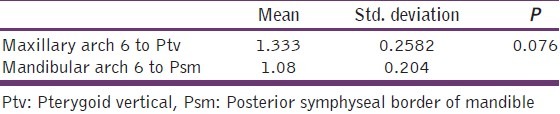
Table 2.
Comparison of retraction between groups in the maxillary arch (left side) at various intervals
Maxillary arch showed more anchor loss than mandibular arch but statistically insignificant. Mean anchor loss in the maxillary arch was 1.33 mm whereas in the mandibular arch was 1.08 mm [Table 4].
Table 4.
Mean anchor loss in maxillary and mandibular arch in between groups
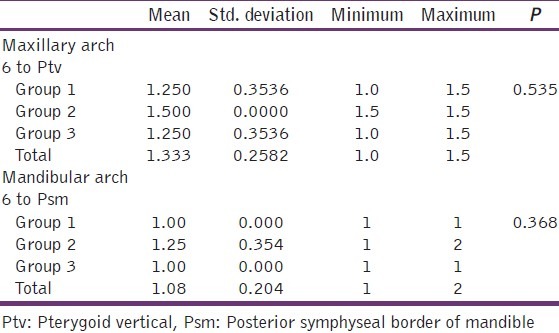
Although anchor loss was more in the maxillary arch than mandibular arch it is statistically insignificant. Furthermore, with elastomeric chain (grp 2), anchor loss was more than the other two groups.
Discussion
The duration of orthodontic treatment is largely dependent on treatment objectives. It is also dependent on tissue reaction, i.e., rate of bone remodeling and osseous turnover. Different force levels induce different tissue reaction, but the overall rate of tooth movement is largely the same. Faster tooth movement can be achieved by altering the biologic environment as suggested by various studies.
Regional accelerated phenomenon was first suggested by Robert Frost. Wilcko et al.[2] have noted that orthodontic tooth movement is accelerated by the increase of bone turnover and decrease of bone density because osteoclasts and osteoblasts are increased by a regional acceleratory phenomenon after the corticotomy. Therefore, orthodontic tooth movement after the corticotomy may be accelerated even without using heavier orthodontic forces. The increase in the rate of retraction can be attributed to regional accelerated phenomenon.
In this study after osteotomy of buccal alveolar plate and undermining of interseptal bone in premolar extraction site was done. Retraction was carried out using Ni - Ti coil springs, E-chain and active tie-backs. Tidy[3] found that Nitinol and titanium molybdenum alloy (TMA) produced more friction than the stainless steel wires. Hence the 0.019″ × 0.25″ rectangular stainless steel wire is used in the present study for retraction as recommended by Mclaughlin bennet trevesi (MBT).[4]
More retraction was seen in the maxillary arch than in the mandibular arch. Reitan[5] revealed that the structure and density of bone has more influence on the rate of the orthodontic tooth movement than applied force. According to Roberts E, the rate of tooth movement is inversely related to bone density. This means that more retraction was recorded in the maxillary arch due to the lesser density of bone in the maxilla. The retraction in the maxillary arch is 5.89 mm which is more than retraction in the mandibular arch which is 5.75 mm at the end of 8 weeks of retraction.
The retraction on the left side was more when compared to the retraction on the right side. The reason for increased retraction on the left side could be due to the habitual mastication on the left side of the patients′ arches being the functional occlusal side. In a study by Singh and Shetty,[6] it was found that space closure was faster on the side where masticatory function is more.
This method of achieving faster en masse retraction immediately after extraction definitely reduced the initial retraction time. We recommend that such procedure must be carried out with appropriate anchorage conservation methods. Use of temporary anchorage devices (TADs) with such procedures would be appropriate in critical anchorage cases to prevent anchor loss and will ensure better treatment results.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Liou EJ, Huang CS. Rapid canine retraction through distraction of the periodontal ligament. Am J Orthod Dentofacial Orthop. 1998;114:372–82. doi: 10.1016/s0889-5406(98)70181-7. [DOI] [PubMed] [Google Scholar]
- 2.Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21:9–19. [PubMed] [Google Scholar]
- 3.Tidy DC. Frictional forces in fixed appliances. Am J Orthod Dentofacial Orthop. 1989;96:249–54. doi: 10.1016/0889-5406(89)90462-9. [DOI] [PubMed] [Google Scholar]
- 4.McLaughlin RP, Bennett JC, Trevisi . A systemized orthodontic treatment mechanics. Edinburgh: Mosby Publications; 2001. pp. 12–3. [Google Scholar]
- 5.Reitan K. Some factors determining the evaluation of forces in Orthodontics. Am J Orthod. 1957;43:32–45. [Google Scholar]
- 6.Singh G, Shetty VS. Extraction space closure in the stage II of Begg technique. J Indian Orthod Soc. 1999;32:58–64. [Google Scholar]