

Abstract
The three-dimensional orientation of dental implant is transferred to a model by means of transfer device and impression material. If more than one implant is inserted and fixtures are not perfectly parallel, the impression may become distorted when removed from the mouth. In this case, a transfer that can be disengaged from the internal implant-abutment connection and removed together with the tray could be useful. An impression transfer device composed of a proper transfer, an inner hexagon and a central screw is described. When the central screw and the hexagon are removed, the proper transfer is free to move horizontally and the tray can be removed from the mouth without distortion of the impression material.
Keywords: Implant, Transfer, Parallel, Impression, Analog
1. Introduction
In two-piece implants (i.e. implant plus abutment), the transfer is used worldwide to replicate either: (i) the three-dimensional position of fixture in alveolar bone, and (ii) anatomical structures surrounding abutment to facilitate manufacturing the prosthetic component (Wenz and Hertrampf, 2008). Therefore, the accuracy of impression that transfer implant position and surrounding structures from mouth to cast model continues to be a problem, especially when more then one fixture has to be rehabilitated and implants are not perfectly parallel (Assuncao et al., 2004).
Accurate recording of spatial implant position is required to obtain a proper support to definitive restoration with passive fitting (Conrad et al., 2007). Optimal positioning of implant analog in the master cast depends on: (i) the transfer technique, and (ii) the ability of the system to maintain precise rotational orientation of the transfer components (Swallow, 2004). Thus, non-parallel implants may result in nonaccurate impressions with subsequent defects in the definitive cast because the impression material is deformed when the tray is removed from the mouth.
The splinted transfer technique was developed 20 years ago. It improves the accuracy of the framework fit in external implant-abutment connection (Swallow, 2004). Likewise, there was no report about internal implant-abutment connection.
In order to avoid the deformation of impression material when tray is removed from mouth in case of non-parallel two-piece internal connection implants, a special transfer was invented (patent reference number PCT/IB2006/003799).
2. Medical device
The proposed impression transfer is composed of 3 concentric and removable pieces (Figs. 1 and 2): (i) a proper transfer (PT), a tubular element that remain blocked in the impression material, (ii) an inner hexagon which is located inside the PT and engages the internal implant-abutment connection thus blocking the rotation of the PT, and (iii) a central screw passing inside the hexagon and pulling together PT and hexagon to implant.
Figure 1.

From left to right, the inner screw, the hexagon (up), the analog (down) and the proper transfer.
Figure 2.
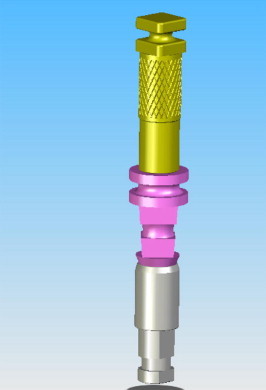
The transfer (3 pieces) screwed to the analog (lower part).
Therefore, a hexagon can freely translate along the PT but cannot rotate with respect to it and to the implant. When the impression material is set, the central screw and the hexagon are removed. Consequently, the PT is free to move horizontally and the tray can be removed from the mouth without distortion of the impression (Figs. 3–5).
Figure 3.

Impression transfers inserted on the upper jaw: implants are not parallel.
Figure 4.

The custom tray containing the impression transfers.
Figure 5.

The tray with proper transfers and the impression material that has no distortion.
3. Discussion
Normally, an impression transfer is composed of two pieces: (i) a retention element with variable shape to be included in the impression material, and (ii) a fixation screw. The identification of the perfect implant position depends on several variables like the impression material, the implant parallelism and the ability of the dental technicians assembling dental models (Vigolo et al., 2003).
The present transfer is useful in case of non-parallel fixtures with internal implant-abutment connection. In fact, when the inner screw and hexagon are removed, the PT is disengaged from the internal implant-abutment connection and can move horizontally. Thus, PT can be removed together with the tray without impression material distortion nor error due to inappropriate repositioning of transfer into the impression.
Vigolo et al. (2003) established that the movement of pick-up type impression copings inside the impression material during clinical and laboratory phases may cause inaccuracy in transferring the spatial position of implants from the oral cavity to the master cast. As a consequence, the laboratory technician may fabricate a restoration that requires corrective procedures. With the new transfer, the impression distortion caused by the removal of the transfer from the impression tray is avoided because the PT is disengaged from the implant.
Another feature of the present transfer is the low vertical encumbrance. The enlarged head of the inner screw is easy to be griped by the clinician. The enlarged head allows screwing/unscrewing easily the inner screw without the need of using specific key, which requires considerable additional vertical space.
4. Conclusion
An impression transfer device composed of a proper transfer, an inner hexagon and a central screw were described. It is useful device when implant is inserted not perfectly parallel to teeth or other fixtures as it can be disengaged from the internal implant-abutment connection and removed together with the tray.
References
- Assuncao W.G., Filho H.G., Zaniquelli O. Evaluation of transfer impressions for osseointegrated implants at various angulations. Implant Dent. 2004;13(4):358–366. doi: 10.1097/01.id.0000144509.58901.f7. [DOI] [PubMed] [Google Scholar]
- Conrad H.J., Pesun I.J., DeLong R., Hodges J.S. Accuracy of two impression techniques with angulated implants. J. Prosthet. Dent. 2007;97(6):349–356. doi: 10.1016/S0022-3913(07)60023-7. [DOI] [PubMed] [Google Scholar]
- Swallow S.T. Technique for achieving a passive framework fit: a clinical case report. J. Oral Implantol. 2004;30:83–92. doi: 10.1563/0.694.1. [DOI] [PubMed] [Google Scholar]
- Vigolo P., Majzoub Z., Cordioli G. Evaluation of the accuracy of three techniques used for multiple implant abutment impressions. J. Prosthet. Dent. 2003;89(2):186–192. doi: 10.1067/mpr.2003.15. [DOI] [PubMed] [Google Scholar]
- Wenz H.J., Hertrampf K. Accuracy of impressions and casts using different implant impression techniques in a multi-implant system with an internal hex connection. Int. J. Oral Maxillofac. Implants. 2008;23(1):39–47. [PubMed] [Google Scholar]