

Abstract
Objective
To describe and analyze the cephalometric dento-skeletal characteristics associated with Angle’s Class II, division 1 malocclusion in Saudi population living in the western region.
Materials and methods
The material examined included 149 lateral head radiographs comprising two series: (1) 85 films of children with Class II, division 1 malocclusion and (2) 62 films of children with “normal” occlusion. Age range of the representing children was 10–13 years.
Results
In Class II division 1 subjects, the maxilla was prognathic in relation to anterior cranial base. The mandible was normally positioned in relation to anterior cranial base. Upper incisors were proclined and lower incisors were normally positioned. The cranial base angle was not different between the two groups.
Conclusions
In the western region of Saudi Arabia, Class II division 1 malocclusion has specific characteristics. The presence of prognathic maxilla, in this sample, indicates that the use of head gear therapy might be more appropriate than functional appliances when treating Class II division 1 malocclusion in Saudis living in the Western region.
Keywords: Cephalometrics, Class II, Malocclusion, Saudi
1. Introduction
A thorough knowledge of the skeletal and dental components that contribute to a malocclusion is essential as these elements may influence the treatment approach.
Angle defined Class II malocclusion as characterized by a distal relation of the lower to the upper permanent first molar to the extent of more than one-half the width of one cusp and the maxillary incisors being protrusive (Angle, 1899). The Class II malocclusion is a common malocclusion with a prevalence ranging between 5% and 29% (Massler and Frankel, 1951; Woodside, 1968). In a Saudi sample, Class II was estimated at 12% of patients who seek treatment (Al-Balkhi and Al-Zahrani, 1994). Two thirds of the patients with Class II division 1 malocclusion were reported to have an associated significant skeletal discrepancy (Woodside, 1968). The dentoskeletal morphology of subjects exhibiting Class II malocclusion has been reported in several studies (Drelich, 1948; Craig, 1951; Riedel, 1952; Fisk et al., 1953; Rothstein, 1971; Harris et al., 1972; Hitchcock, 1973; Moyers et al., 1980; McNamara, 1981; Carter, 1987; Karlsen, 1994; Rosenblum, 1995; Pancherz et al., 1997).
Some reports have indicated that the maxilla in Class II division 1 patients was more protrusive and the mandible was normal in size and position (Rosenblum, 1995). Other studies found that the maxilla was in a normal position in relation to the cranial base while the mandible was retrusive (Craig, 1951; Hitchcock, 1973; McNamara, 1981). Others found that Class II skeletal pattern is due to both maxillary protrusion and mandibular retrusion (Gilmore, 1950; Henery, 1957; Rosenblum, 1995; Pancherz et al., 1997). It seems that ethnic backgrounds of the sample used in these studies have played a role in determining the craniofacial characteristics of the Class II pattern.
The objective of this study was to assess the dentofacial characteristics of a sample of Saudi children, living in the western region, having Class II division 1 malocclusion and to compare it with another sample of Saudi children having Class I ideal occlusion.
2. Materials and methods
A total of 85 lateral cephalograms of Saudi children (41 females and 44 males, aged 10–13 years) having full cusp Class II molar relationship, increased overjet (more than 5 mm), no history of orthodontic treatment and in the early permanent dentition stage were selected to be included in the study group (Class II group). A control group of 62 lateral cephalograms of Saudi children (33 females and 29 males, aged 9–12) having acceptable profiles, Class I molar relationship, minimum overbite and overjet, minimum or no crowding, and no previous orthodontic treatment was used for comparison (Class I group) (Table 1). The subjects in both groups were Saudi children living in the western region, selected through the public health program conducted at King Abdulaziz University for the primary and intermediate public school students in 2004–2005.
Table 1.
Age and gender distribution of the samples.
| Group | N | Mean (year) | SD |
|---|---|---|---|
| Class II, division 1 | |||
| Female | 41 | 10.53 | 1.23 |
| Male | 44 | 10.67 | 1.12 |
| Total | 85 | 10.75 | 1.17 |
| Class I | |||
| Female | 33 | 10.44 | 1.18 |
| Male | 29 | 10.32 | 1.20 |
| Total | 62 | 10.38 | 1.29 |
2.1. Cephalometric tracings
The radiographs were traced and analyzed manually by a single examiner. Magnification was recorded for each cephalometric head film and the readings were adjusted accordingly. Eighteen linear and angular measurements were calculated for each group (Fig. 1 and Table 2).
Figure 1.
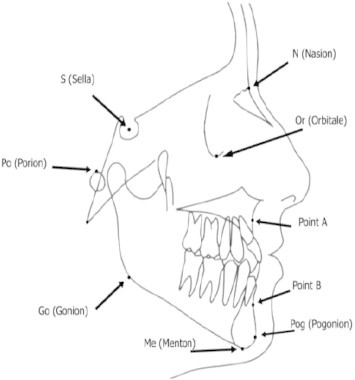
Cephalometric reference points. Different reference points used in the present study and their abbreviations.
Table 2.
Different cephalometric measurements used in the study.
| Measurement | Interpretation |
|---|---|
| N–Pog–FH (°) | Intersection between N–Pog plane and Frankfort horizontal plane |
| N–Pog to SN (°) | Intersection between N–Pog plane and SN plane |
| SNA (°) | Maxillary apical base relationship to anterior cranial base |
| SNB (°) | Mandibular apical base relationship to anterior cranial base |
| ANB (°) | Apical base relationship |
| NA–A–Pog (°) | Angle of convexity |
| MP–FH (°) | Inclination of mandibular plane to FH |
| MP–SN (°) | Inclination of mandibular plane angle to anterior cranial base |
| OP–SN (°) | Inclination of occlusal plane to anterior cranial base |
| Y-axis (°) | Angle made between SN and N-Gn line |
| LAFH% | Lower face height (Anterior nasal spine-Menton) |
| U1–SN (°) | Inclination of maxillary incisors to anterior cranial base |
| U1–NA (°) | Inclination of maxillary incisors to NA |
| U1–NA (mm) | Protrusion of maxillary incisors to NA |
| U1–L1 (°) | Inclination of maxillary incisors to mandibular incisors |
| L1–MP (°) | Inclination of mandibular incisors to mandibular plane |
| L1–NB (°) | Inclination of mandibular incisors to NB |
| L1–NB (mm) | Position of maxillary incisors relative to NB |
| L1–A–Pog (°) | Inclination of mandibular incisors to A–Pog plane |
| L1–A–Pog (mm) | Position of mandibular incisors relative A–Pog plane |
2.2. Statistical analysis
The mean and standard deviation for each measurement were calculated using the Statistical Package for Social Sciences (SPSS, Version 15.0 Inc., Chicago, IL) for Windows. The variables in the two groups were compared using the independent t-test (p < .05 and p < .001).
2.3. Method error
To asses tracing errors, 20 films were retraced after 1 month. The method error was calculated using Dahlberg’s double determination formula (Dahlberg, 1940). Results are summarized in Table 3. The error ranged from 0.14° to 1°.
Table 3.
The results of the tracing errors as calculated using Dahlberg’s double determination formula.
| Variable | Method error |
|---|---|
| N–Pog–FH (°) | 0.95 |
| N–Pog–SN (°) | 0.44 |
| SNA (°) | 0.60 |
| SNB (°) | 0.33 |
| ANB (°) | 0.45 |
| N–A to A–Pog (°) | 0.57 |
| MP/FH (°) | 0.91 |
| MP/SN (°) | 0.45 |
| OP/SN (°) | 0.27 |
| Y-axis (°) | 0.85 |
| U1–SN (°) | 0.71 |
| U1–L1 (°) | 1 |
| L1–MP (°) | 0.35 |
| L1–NB (°) | 0.21 |
| L1–NB mm | 0.33 |
| L1–A–Pog (°) | 0.14 |
| LAFH% | 0.83 |
| N–S–BA (°) | 0.59 |
3. The results
Table 4 presents the mean and standard deviation values for the angular and linear measurements for the Class II group. Table 5 presents a comparison between the Class II group and Class I group.
Table 4.
Different cephalometric measurements of patients with Class II division1 malocclusion.
| Measurement | Mean | Std. deviation |
|---|---|---|
| N–Pog to FH (°) | 85.07 | 3.14 |
| N–Pog to SN (°) | 75.20 | 7.90 |
| SNA (°) | 81.32 | 3.12 |
| SNB (°) | 75.25 | 2.99 |
| ANB (°) | 6.00 | 2.33 |
| N–A to A–Pog (°) | 9.55 | 4.65 |
| MP to FH (°) | 27.84 | 3.82 |
| MP to SN (°) | 36.35 | 3.71 |
| OP to SN (°) | 19.94 | 3.10 |
| Y-axis (°) | 70.00 | 3.09 |
| U1–SN (°) | 109.66 | 5.78 |
| U1–L1 (°) | 120.15 | 8.52 |
| L1–MP (°) | 96.67 | 6.16 |
| L1–NB (°) | 28.12 | 4.78 |
| L1–NB (mm) | 6.02 | 1.67 |
| L1–A–Pog (°) | 25.34 | 4.71 |
| LAFH% | 54.54 | 3.04 |
| N–S–BA (°) | 131.04 | 2.45 |
Table 5.
Comparisons between means of the measured variables in Class II group and their corresponding variables in Class I.
| Measurement | Class | N | Mean | Std. deviation | Std. error mean | P | t |
|---|---|---|---|---|---|---|---|
| N–Pog–FH (°) | I | 62 | 86.52 | 3.16 | .395 | .006 | 2.779 |
| II | 85 | 85.07 | 3.14 | .341 | |||
| N–Pog–SN (°) | I | 62 | 75.95 | 3.21 | .401 | .432 | .789 |
| II | 85 | 75.20 | 7.90 | .857 | |||
| SNA (°) | I | 62 | 79.75 | 2.59 | .324 | .001⁎ | −3.352 |
| II | 85 | 81.32 | 3.12 | .338 | |||
| SNB (°) | I | 62 | 75.64 | 2.60 | .326 | .401 | .843 |
| II | 85 | 75.25 | 2.99 | .324 | |||
| ANB (°) | I | 62 | 4.10 | 1.97 | .246 | .000⁎⁎ | −5.393 |
| II | 85 | 6.00 | 2.33 | .252 | |||
| N–A to A–Pog (°) | I | 62 | 6.18 | 3.11 | .388 | .000⁎⁎ | −5.280 |
| II | 85 | 9.55 | 4.65 | .505 | |||
| MP/FH (°) | I | 62 | 26.84 | 4.34 | .543 | .145 | −1.468 |
| II | 85 | 27.84 | 3.82 | .414 | |||
| MP/SN (°) | I | 62 | 36.32 | 4.13 | .516 | .963 | −.047 |
| II | 85 | 36.35 | 3.71 | .403 | |||
| OP/SN (°) | I | 62 | 19.91 | 7.30 | .912 | .978 | −.028 |
| II | 85 | 19.94 | 3.10 | .336 | |||
| Y-axis (°) | I | 62 | 70.16 | 3.25 | .406 | .756 | .311 |
| II | 85 | 70.00 | 3.09 | .335 | |||
| U1–SN (°) | I | 62 | 105.27 | 8.16 | 1.020 | .000⁎⁎ | −3.668 |
| II | 85 | 109.66 | 5.78 | .627 | |||
| U1–L1 (°) | I | 62 | 121.52 | 9.33 | 1.166 | .362 | .915 |
| II | 85 | 120.15 | 8.52 | .924 | |||
| L1–MP (°) | I | 62 | 94.96 | 7.81 | .977 | .153 | −1.438 |
| II | 85 | 96.67 | 6.16 | .668 | |||
| L1–NB (°) | I | 62 | 27.62 | 6.17 | .771 | .589 | −.542 |
| II | 85 | 28.12 | 4.78 | .519 | |||
| L1–NB mm | I | 62 | 5.87 | 2.39 | .299 | .673 | −.424 |
| II | 85 | 6.02 | 1.67 | .181 | |||
| L1–A–Pog (°) | I | 62 | 26.32 | 4.82 | .603 | .221 | 1.231 |
| II | 85 | 25.34 | 4.71 | .511 | |||
| LAFH% | I | 62 | 55.04 | 3.12 | .391 | .332 | .974 |
| II | 85 | 54.54 | 3.04 | .330 | |||
| N–S–BA (°) | I | 62 | 131.04 | 2.45 | .265 | .114 | 2.509 |
| II | 85 | 132.62 | 4.60 | .575 |
Significant difference between the two groups; p < 0.05.
Significant difference between the two groups; p < 0.001.
Compared to the subjects in the control group, those in the Class II group have significantly increased ANB and N–A–Pog angles (p < 0.001). Maxilla was significantly more prognathic in Class II group as indicated by the increased SNA angle (p < 0.001). There was no significant difference in the mean position of the mandible (SNB, SN–Pog) between the two groups (p > 0.05). Mandibular plane angle was also similar in both groups. Dentally, upper incisors were significantly more proclined in the Class II group (p < 0.001). No statistically significant difference was found between the two groups in mandibular plane angle (p > 0.05).
4. Discussion
The Class II group sample in this study included Saudi children taken form a larger randomly collected sample from school children. In addition, comparison group consisted of subjects taken from the records used previously to establish Saudi norms in the western region of Saudi Arabia (Hassan, 2006). These randomly selected samples represent the Saudi population in the western region of Saudi Arabia. Class II division 2 was not addressed in this study due to the limited number of children with this type of malocclusion seen in the specified school sample.
The Class II malocclusion may result from several combinations of skeletal and dental components (Wylie, 1947; Drelich, 1948; Craig, 1951; Moyers et al., 1980; McNamara, 1981). In the present study, the subjects in the Class II groups had skeletal Class II relationship, due to prognathic maxilla in the presence of normal mandible in most of the cases. This is in agreement with several studies (Renfroe, 1948; Pancherz et al., 1997) and in contrary to Karlsen and Krogstad (1999) and Sayin and Turkkahraman (2005) who found the maxilla to be normally positioned in Class II division 1 malocclusion. The mean angle of SNB was similar in both groups and this is in contrast to several studies (Gilmore, 1950; Craig, 1951; Hitchcock, 1973; McNamara, 1981; Pancherz et al., 1997) that indicated mandibular retrusion as a common characteristic of Class II malocclusion.
Treatment modalities for Class II division 1 children aim at modifying maxillo-mandibular growth using either functional appliance or headgear. The results of the present study support the need to harness maxillary growth or at least distalize upper dentition, in most of the Saudi patients. Therefore, headgear appliance could be a major alternative in the majority of growing Class II division 1 patients. In addition, camouflage treatment via extraction of maxillary premolars could be another good alternative for the treatment of those patients. Lower incisor inclination was also similar in both groups and this is in agreement with Henery (1957) and in contrast to Al-Khateeb and Al-Khateeb (2009) who found the lower incisors to be more proclined in Class II division 1.
The relationship between the cranial base angle and malocclusion is controversial in the literature. In the present study, cranial base angle was similar in both groups and this is in agreement with several reports (Bacon et al., 1992; Renfroe, 1948; Menezes, 1974; Guyer et al., 1986) and disagrees with several other reports that indicated a correlation between cranial base angulation and malocclusion (Anderson and Popovich, 1983; Bjork, 1955; Kasai et al., 1995).
Future studies are required to evaluate the skeletal and dental features of Saudis living in the other regions of Saudi Arabia and to compare the results with the present data. In addition, three dimensional skeletal and dental evaluations of the different types of malocclusion in Saudis are also required. Finally the characteristics of Class II division 2 malocclusion are also needed to be evaluated in the Saudi population.
5. Conclusion
Class II division 1 malocclusion in Saudi children living in the western region is characterized by the following: significantly increased ANB angle, more prognathic maxilla, normal mandibular position and proclined upper incisors. These features may favor specific treatment concepts, such as harnessing maxillary growth, or camouflage dental treatment when treating Saudi children living in the western region with Class II division 1 malocclusion.
References
- Al-Balkhi K.M., Al-Zahrani A.M. The pattern of malocclusions in Saudi Arabian patients attending for orthodontic treatment at The College of Dentistry, King Saud University, Riyadh. Saudi Dental J. 1994;6(3):138–144. [Google Scholar]
- Al-Khateeb S.N., Al-Khateeb A. Anteroposterior and vertical components of Class II division 1 and division 2 malocclusion. Angle Orthod. 2009;79:859–866. doi: 10.2319/062208-325.1. [DOI] [PubMed] [Google Scholar]
- Anderson D., Popovich F. Relation of cranial base flexure to cranial form and mandibular position. Am. J. Phys. Anthropol. 1983;61(2):181–187. doi: 10.1002/ajpa.1330610206. [DOI] [PubMed] [Google Scholar]
- Angle E.H. Classification of malocclusion. Dent Cosmos. 1899;41:248–264. [Google Scholar]
- Bacon W., Eiller V., Hildwein M., Dubois G. The cranial base in subjects with dental and skeletal Class II. Eur. J. Orthod. 1992;14(3):224–228. doi: 10.1093/ejo/14.3.224. [DOI] [PubMed] [Google Scholar]
- Bjork A. Cranial base development. Am. J. Orthod. 1955;41:198–225. [Google Scholar]
- Carter N.E. Dentofacial changes in untreated Class II division 1 subjects. Br. J. Orthod. 1987;14(4):225–234. doi: 10.1179/bjo.14.4.225. [DOI] [PubMed] [Google Scholar]
- Craig C.E. The skeletal patterns characteristic of Class I and Class II, Division I malocclusions in norma lateralis. Angle Orthod. 1951;21(1):44–56. doi: 10.1043/0003-3219(1951)021<0044:TSPCOC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Dahlberg G. George Allen and Unwin Ltd.; London, UK: 1940. Statistical Methods for Medical and Biological Students. pp. 122–132. [Google Scholar]
- Drelich R. A cephalometric study of untreated Class II, Division 1 Malocclusion. Angle Orthod. 1948;18:70–75. [Google Scholar]
- Fisk G.V., Culbert M.R., Grainger R.M., Hermrend B., Moyers R.E. The morphology and physiology of distoocclusion. Am. J. Orthod. 1953;39:3–12. [Google Scholar]
- Gilmore W.A. Morphology of the adult mandible in Class II, Division 1 malocclusion and in excellent occlusion. Angle Orthod. 1950;20(3):137–146. doi: 10.1043/0003-3219(1950)020<0137:MOTAMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Guyer E.C., Ellis E.E., 3rd., McNamara J.A., Jr., Behrents R.G. Components of class III malocclusion in juveniles and adolescents. Angle Orthod. 1986;56(1):7–30. doi: 10.1043/0003-3219(1986)056<0007:COCIMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Harris J.E., Kowalski C.J., Walker G.F. Discrimination between normal and Class II individuals using Stiener’s analysis. Angle Orthod. 1972;42:212–220. doi: 10.1043/0003-3219(1972)042<0212:DBNACI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Hassan A.H. Cephalometric norms for Saudi adults living in the western region of Saudi Arabia. Angle Orthod. 2006;76:109–113. doi: 10.1043/0003-3219(2006)076[0109:CNFSAL]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Henery R. A classification of class II division 1 malocclusion. Angle Orthod. 1957;27:83–92. [Google Scholar]
- Hitchcock H.P. A cephalometric description of Class II, Division 1 malocclusion. Am. J. Orthod. 1973;63(4):414–423. doi: 10.1016/0002-9416(73)90146-2. [DOI] [PubMed] [Google Scholar]
- Karlsen A.T. Craniofacial morphology in children with Angle Class II-1 malocclusion with and without deepbite. Angle Orthod. 1994;64(6):437–446. doi: 10.1043/0003-3219(1994)064<0437:CMICWA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Karlsen A.T., Krogstad O. Morphology and growth in convex profile facial patterns: a longitudinal study. Angle Orthod. 1999;69(4):334–344. doi: 10.1043/0003-3219(1999)069<0334:MAGICP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- Kasai K., Moro T., Kanazawa E., Iwasawa T. Relationship between cranial base and maxillofacial morphology. Eur. J. Orthod. 1995;17:403–410. doi: 10.1093/ejo/17.5.403. [DOI] [PubMed] [Google Scholar]
- Massler M., Frankel J.M. Prevalence of malocclusion in children aged 14 to 18 years. Am. J. Orthod. 1951;37(10):751–768. doi: 10.1016/0002-9416(51)90047-4. [DOI] [PubMed] [Google Scholar]
- McNamara J.A., Jr. Components of class II malocclusion in children 8–10 years of age. Angle Orthod. 1981;51(3):177–202. doi: 10.1043/0003-3219(1981)051<0177:COCIMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Menezes D. Comparison of craniofacial features of English children with Angle class II division 1 and Angle class I occlusions. J. Dent. 1974;2:250–254. doi: 10.1016/0300-5712(74)90027-x. [DOI] [PubMed] [Google Scholar]
- Moyers R.E., Riolo M.L., Guire K.E., Wainright R.L., Bookstein F.L. Differential diagnosis of class II malocclusions. Part 1. Facial types associated with class II malocclusions. Am. J. Orthod. 1980;78(5):477–494. doi: 10.1016/0002-9416(80)90299-7. [DOI] [PubMed] [Google Scholar]
- Pancherz H., Zieber K., Hoyer B. Cephalometric characteristics of Class II division 1 and Class II division 2 malocclusions: a comparative study in children. Angle Orthod. 1997;67(2):111–120. doi: 10.1043/0003-3219(1997)067<0111:CCOCID>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- Renfroe E. A study of the facial patterns associated with Class I, Class II division 1 and Class II division 2 malocclusions. Angle Orthod. 1948;19:12–15. [Google Scholar]
- Riedel R. The relation of maxillary structures to cranium in malocclusion and normal occlusion. Angle Orthod. 1952;22:142–145. [Google Scholar]
- Rosenblum R.E. Class II malocclusion: mandibular retrusion or maxillary protrusion? Angle Orthod. 1995;65(1):49–62. doi: 10.1043/0003-3219(1995)065<0049:CIMMRO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Rothstein T.L. Facial morphology and growth from 10 to 14 years of age in children presenting Class II, Division 1 Malocclusion: a comparative roentgenographic cephalometric study. Am. J. Orthod. 1971;60(6):619–620. doi: 10.1016/0002-9416(71)90202-8. [DOI] [PubMed] [Google Scholar]
- Sayin M.O., Turkkahraman H. Cephalometric evaluation of nongrowing females with skeletal and dental Class II, division 1 malocclusion. Angle Orthod. 2005;75(4):656–660. doi: 10.1043/0003-3219(2005)75[656:CEONFW]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Woodside D.G. The present role of the general practitioner in orthodontics. Dent. Clin. North. Am. 1968;1:483–508. [PubMed] [Google Scholar]
- Wylie W. The assessment of anteroposterior dysplasia. Angle Orthod. 1947;17:97–109. [Google Scholar]