

Abstract
Objective
The aim of the present study was to study the etiologies and patterns of maxillofacial fractures in patients treated in Riyadh City, Saudi Arabia, between 2007 and 2011.
Patients and methods
Data were obtained through a retrospective review of 237 patients admitted to the King Saud Medical City Dental Department with a diagnosis of maxillofacial trauma. After excluding patient files with incomplete or unclear records, and cases in which computed tomography showed no evidence of fracture, the files of 200 patients with a diagnosis of maxillofacial fracture were included in the study. For each case, patient’s sex and age, pattern of facial fractures, and cause of injury were recorded on a data sheet. The data were transferred to an SPSS (ver. 16.0; SPSS Inc., Chicago, IL, USA) spreadsheet for statistical analysis. The chi-square test was used to test the association between two categorical variables or factors (age group, cause) with p value set at p<0.05, and t-test value at <0.05 and independent.
Results
Motor vehicle accidents were the most common cause of maxillofacial fractures in most age groups, especially in males. Within the study sample, mandibular fractures were significantly more common than middle-third facial fractures (56.4% vs. 43.6%; p=0.006). Among mandibular fractures, parasymphyseal fractures were most common (47%), followed by condylar fractures (35.3%). Most (77.2%) middle-third facial fractures involved the zygomatic complex, and the incidence of such fractures differed significantly between male and female patients. p=0.72, not significant.
Conclusion
Males were more prone to maxillofacial fractures, perhaps as a result of the conservative nature of Saudi society, as the rules of Saudi Arabia do not allow the females to drive. Motor vehicle accidents were the most common cause of maxillofacial fractures in patients aged 10–29 years, indicating the high demand for the application of stricter traffic rules to reduce the rate of such accidents.
Keywords: Maxillofacial trauma, Pattern of facial fractures, Etiology of maxillofacial fractures
1. Introduction
The causes of maxillofacial fracture have changed continuously over the past three decades, and they continue to do so. The main causes of this fracture type worldwide are traffic accidents, assaults, falls, and sport-related injuries. Many studies have examined the incidence and causes of maxillofacial injury (Adekeye, 1980; Afzelius and Rosen, 1980; Hagan and Huelke, 1961; Khalil and Shaladi, 1981; Motamedi, 2003; Van Hoof et al., 1977).
The epidemiology of facial fractures varies among populations with respect to type, severity, and cause (Girotto et al., 2001). An understanding of maxillofacial trauma aids the assessment of behavioral patterns in people in different countries and helps to establish effective measures for injury prevention and treatment (Maliska et al., 2009).
The patterns of maxillofacial trauma in Saudi Arabia are poorly studied. To our knowledge, only two studies have focused on this subject (Al Ghamdi, 1998; Ansari et al., 2000; Ministry of Interior, 1997). Thus, the aim of the present study was to examine the etiologies and patterns of maxillofacial fractures in patients treated in Riyadh City, Saudi Arabia between 2007 and 2011.
2. Patients and methods
This study was approved by the College of Dentistry Research Center, King Saud University. Data were obtained through a retrospective review of 237 patients admitted to the King Saud Medical City (KSMC) Dental Department in Riyadh City between January 2007 and September 2011 with a diagnosis of maxillofacial trauma. KSMC is one of the main hospitals with maxillofacial facilities affiliated with the Ministry of Health of Saudi Arabia and is considered to be the primary trauma center in Riyadh.
After excluding patient files with incomplete or unclear records, and cases in which computed tomography (CT) showed no evidence of fracture, the files of 200 patients with a diagnosis of maxillofacial fracture were included in the study. The following data were recorded for each patient: sex and age; facial fracture pattern (orbital, nasal, maxillary, mandibular, zygomatic), determined using CT images and operative reports; cause of injury; and time of admission.
Patients were divided into six age groups (0–9, 10–19, 20–29, 30–39, 40–49, and 50–59 years). Data were recorded on a special data sheet and transferred to an SPSS (ver. 16.0; SPSS Inc., Chicago, IL, USA) spreadsheet for statistical analysis. The chi-square test was used to test the association between two categorical variables or factors (age group, cause) with p value set at p<0.05, and t-test value at <0.05 and independent.
3. Results
In the present study, data from the files of 200 patients [172 males (86%), 28 females (14%)] with 211 maxillofacial fractures were analyzed. Mandibular fractures (119/211, 56.4%) were significantly more common than middle-third facial fractures (92/211, 43.6%; p = 0.008). Among mandibular fractures, parasymphyseal fractures were most common (56/199, 47%), followed by condylar fractures (42/119, 35.3%), but the incidence did not differ significantly (p = 0.063). Most (71/92, 77.2%) middle-third facial fractures involved the zygomatic complex, and the incidence of such fractures differed significantly between male and female patients (p = 0.72, not significant). The distribution of fractures by anatomic site and patient sex is shown in Tables 1 and 2 and Figs. 1 and 2.
Table 1.
Anatomical distribution of mandibular fractures and gender distribution.
| Gender |
Total | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| Mandibular | Condyle | Count | 34 | 8 | 42 |
| Angle | Count | 29 | 4 | 33 | |
| Body | Count | 26 | 4 | 30 | |
| Symphysis | Count | 10 | 2 | 12 | |
| Dentoalveolar | Count | 8 | 3 | 11 | |
| Ramus | Count | 2 | 0 | 2 | |
| Coronoid | Count | 2 | 1 | 3 | |
| Parasymphysis | Count | 48 | 8 | 56 | |
| Total | Count | 102 | 17 | 119 | |
Table 2.
Anatomical distribution of maxillary fractures and gender distribution.
| Gender |
Total | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| Mid Faciala | Maxillary | Count | 2 | 0 | 2 |
| ZOC | Count | 63 | 8 | 71 | |
| Nasal | Count | 5 | 1 | 6 | |
| Dentoalveolar | Count | 11 | 2 | 13 | |
| Le Fort I | Count | 13 | 1 | 14 | |
| Le Fort II | Count | 6 | 0 | 6 | |
| Le Fort III | Count | 2 | 0 | 2 | |
| Total | Count | 81 | 11 | 92 | |
Figure 1.
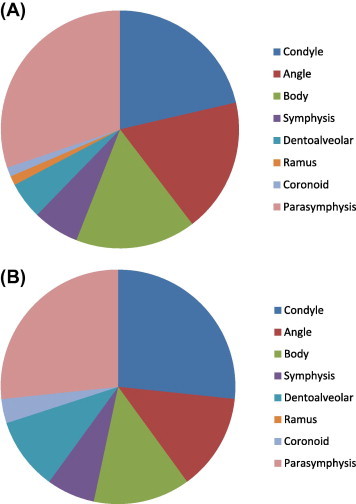
Anatomic distribution of mandibular fractures in male (A) and female (B) patients.
Figure 2.
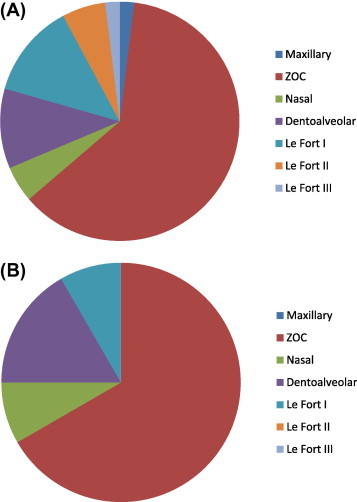
Anatomical distribution of middle-third facial fractures in male (A) and female (B) patients.
Causes of maxillofacial fracture in each age group are shown in Table 3 and Fig. 3. Among males, motor vehicle accidents were the most frequent cause of injury (86.1%) in all age groups except those aged 0–9 years, among whom falls were the most common cause (50%). In female patients aged 10–19 (75%) and 20–29 years (77.8%), motor vehicle accidents were the most common cause of injury; in those aged 0–9 (60%) and 30–39 years (66.7%), falls were the most common cause (Table 4, Fig. 4). Whereas, falls were not the main cause for other groups. The numbers of males and females with fractures caused by motor vehicle accidents differed significantly (p = 0.00). Other causes of fracture are shown in Tables 3,4 and Figures 3,4. Significant differences by age group were seen in the entire sample.
Table 3.
Causes of maxillofacial fractures in relation to age groups in male patients.
| Gender | Cause |
Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| MVA | Falls | Violent Assaults | Sports | Others | |||||
| Male | Age | Age 0–9 | Count | 3 | 4 | 1 | 0 | 0 | 8 |
| % within age | 37.5% | 50.0% | 12.5% | .0% | .0% | 100.0% | |||
| % within Cause | 2.9% | 13.3% | 4.5% | .0% | .0% | 4.7% | |||
| Age 10–19 | Count | 38 | 10 | 5 | 7 | 1 | 61 | ||
| % within age | 62.3% | 16.4% | 8.2% | 11.5% | 1.6% | 100.0% | |||
| % within Cause | 36.2% | 33.3% | 22.7% | 63.6% | 25.0% | 35.5% | |||
| Age 20–29 | Count | 45 | 10 | 9 | 4 | 1 | 69 | ||
| % within age | 65.2% | 14.5% | 13.0% | 5.8% | 1.4% | 100.0% | |||
| % within Cause | 42.9% | 33.3% | 40.9% | 36.4% | 25.0% | 40.1% | |||
| Age 30–39 | Count | 12 | 3 | 5 | 0 | 1 | 21 | ||
| % within age | 57.1% | 14.3% | 23.8% | .0% | 4.8% | 100.0% | |||
| % within Cause | 11.4% | 10.0% | 22.7% | .0% | 25.0% | 12.2% | |||
| Age 40–49 | Count | 5 | 3 | 2 | 0 | 1 | 11 | ||
| % within age | 45.5% | 27.3% | 18.2% | .0% | 9.1% | 100.0% | |||
| % within Cause | 4.8% | 10.0% | 9.1% | .0% | 25.0% | 6.4% | |||
| Age 50–59 | Count | 2 | 0 | 0 | 0 | 0 | 2 | ||
| % within age | 100.0% | .0% | .0% | .0% | .0% | 100.0% | |||
| % within Cause | 1.9% | .0% | .0% | .0% | .0% | 1.2% | |||
| Total | Count | 105 | 30 | 22 | 11 | 4 | 172 | ||
| % within age | 61.0% | 17.4% | 12.8% | 6.4% | 2.3% | 100.0% | |||
| % within Cause | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | |||
Figure 3.
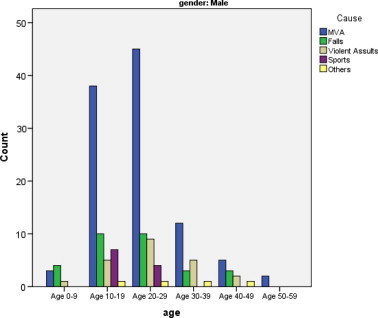
Causes of maxillofacial fracture in male patients by age group.
Table 4.
Causes of maxillofacial fractures in relation to age groups in female patients.
| Gender | Cause |
Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| MVA | Falls | Violent assaults | Sport | Others | |||||
| Female | Age | Age 0–9 | Count | 2 | 3 | 0 | – | – | 5 |
| % within age | 40.0% | 60.0% | .0% | – | – | 100.0% | |||
| % within Cause | 11.8% | 30.0% | .0% | – | – | 17.9% | |||
| Age 10–19 | Count | 6 | 2 | 0 | – | – | 8 | ||
| % within age | 75.0% | 25.0% | .0% | – | – | 100.0% | |||
| % within Cause | 35.3% | 20.0% | .0% | – | – | 28.6% | |||
| Age 20–29 | Count | 7 | 2 | 0 | – | – | 9 | ||
| % within age | 77.8% | 22.2% | .0% | – | – | 100.0% | |||
| % within Cause | 41.2% | 20.0% | .0% | – | – | 32.1% | |||
| Age 30–39 | Count | 1 | 2 | 0 | – | – | 3 | ||
| % within age | 33.3% | 66.7% | .0% | – | – | 100.0% | |||
| % within Cause | 5.9% | 20.0% | .0% | – | – | 10.7% | |||
| Age 40–49 | Count | 1 | 1 | 1 | – | – | 3 | ||
| % within age | 33.3% | 33.3% | 33.3% | – | – | 100.0% | |||
| % within Cause | 5.9% | 10.0% | 100.0% | – | – | 10.7% | |||
| Total | Count | 17 | 10 | 1 | – | – | – | 28 | |
| % within age | 60.7% | 35.7% | 3.6% | – | – | – | 100.0% | ||
| % within Cause | 100.0% | 100.0% | 100.0% | – | – | – | 100.0% | ||
Figure 4.
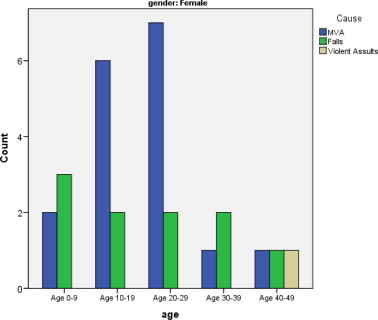
Causes of maxillofacial fracture in female patients by age group.
4. Discussion
The etiology and incidence of maxillofacial fracture vary by country, socioeconomic status, and cultural characteristics (Adhikari et al., 2012; Haung et al., 1990). Examination of the epidemiology of this type of fracture within a given country is important to determine what is needed to improve the quality of life and health of its citizens (Maliska et al., 2009).
Our finding that mandibular fractures were the most common type of maxillofacial fracture (56.4%) is comparable to the results of two 4 year retrospective studies of the etiologies and patterns of facial fractures in the United Arab Emirates (UAE; 53%) (Klenk and Kovacs, 2003) and in Sharjah, UAE (51%) (Al Ahmed et al., 2004). This comparability reflects the similar geographic locations and cultural habits of Saudi Arabia and the UAE, and the similar time periods during which the studies were conducted. Moreover, despite differences in geographic location and cultural properties, our result also agrees with that of Maliska et al. (2009), who found that mandibular fractures accounted for 54.6% of maxillofacial fractures in Brazil. Our result was slightly higher than those obtained in a 5 year retrospective study in Brazil (44.2%) (Brasileiro and Passeri, 2006) and a 1 year retrospective study in a hospital in Belo Horizonte, Brazil (39.97%) (Chrcanovic et al., 2004).
In contrast to our results, a 10 year review in Austria (Gassner et al., 2003) showed that the most common facial injury site was the middle-third of the face. This difference reflects the main etiologies of fracture in the studies, which were motor vehicle accidents in the present study and activities of daily life and falls in Gassner et al. (2003).
In the present study, motor vehicle accidents (60.85% of the whole sample) were the main etiological factor in maxillofacial injury in males (61% males, 60.7% females), except those aged 0–9 years. This finding is in agreement with those of many studies (Al Ahmed et al., 2004; Bataineh, 1998; Olasoji et al., 2002; Tanaka et al., 1994), and can be explained by the large increase in the number of vehicles and expansion of road networks within and between cities as a result of rapid economic growth since the oil era began to increase the motorization rate in 1973 (Al Ahmed et al., 2004; Ansari et al., 2000; Ministry of Interior, 1997). In contrast to our study results, other studies have reported that assault was the main etiological factor in maxillofacial injury (Al Ahmed et al., 2004; Oikarinen et al., 1993; Strom et al., 1991). This difference may be explained by the conservative nature of Saudi culture and cultural differences among countries. The females are not allowed to drive in Saudi Arabia. Moreover, assault between the husband and wife is difficult to be recorded in some cases as the family refuses to say truly, the cause of trauma in case if it was from the husband to his wife. Our finding that the main etiological factor in maxillofacial injury among patients aged 0–9 years was not motor vehicle accidents shows improvement in Saudi citizens’ behavior with respect to traffic rules, as the transport of many young children unrestrained in front passenger seats was reported previously in Gulf countries (Al Ahmed et al., 2004; Bener and Jadaan, 1992; Jadaan et al., 1992; Strom et al., 1991).
The male to female ratio in our study (6.1:1) was higher than those reported by many authors, which has ranged from 3:1 to 5.4:1 (Bener and Jadaan, 1992; Chrcanovic et al., 2004; Gassner et al., 2003; Van Hoof et al., 1977), but was in agreement with the ratio (males 92%, females 8%) reported by Al Ahmed et al. (2004). This result reflects the conservative and religious nature of Gulf country societies, which is more pronounced in Saudi Arabia than in the UAE and other Gulf countries; for example, women are not allowed to drive in Saudi Arabia.
Limitations of this study include, a lot of cases were not recorded properly, so they were excluded from the study, and the assault between the husband and wife is difficult to be recorded in some cases as the family refuses to say truly, the cause of trauma in case if it was from the husband to his wife.
5. Conclusion
-
●
Mandibular fractures were the most common maxillofacial fractures among patients treated in Riyadh City, Saudi Arabia.
-
●
Parasymphyseal fractures were the most common type of mandibular fracture, followed by condylar fractures.
-
●
Zygomatic fractures were the most common type of middle-third facial fracture.
-
●
Males were more prone than females to maxillofacial fractures, perhaps due to the conservative nature of Saudi society.
-
●
Motor vehicle accidents were the most common cause of maxillofacial fractures in most age groups, especially in males and those aged 10–29 years.
-
●
The study findings highlight the high demand for the application of stricter traffic rules to reduce the rate of motor vehicle accidents.
Conflict of interest
The authors have no conflict of interest to declare.
Acknowledgment
The authors thank the College of Dentistry Research Center, Dental College, King Saud University, and the King Saud Medical City Dental Department for their help and support.
Footnotes
Peer review under responsibility of King Saud University.

References
- Adekeye E.O. The pattern of fractures of the facial skeleton in Kaduna, Nigeria: a survey of 1447 cases. Oral Surg. Oral Med. Oral Pathol. 1980;49:491. doi: 10.1016/0030-4220(80)90068-7. [DOI] [PubMed] [Google Scholar]
- Adhikari R.B., Karmacharya A., Malla N. Pattern of mandibular fractures in western region of Nepal. Nepal J. Med. Sci. 2012;1(1):45–48. [Google Scholar]
- Afzelius L.E., Rosen C. Facial fractures: a review of 368 cases. Int. J. Oral Surg. 1980;9:25. doi: 10.1016/s0300-9785(80)80003-2. [DOI] [PubMed] [Google Scholar]
- Al Ahmed H.E., Jaber M.A., Salem H., Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004;98:166–170. doi: 10.1016/j.tripleo.2004.01.020. [DOI] [PubMed] [Google Scholar]
- Al Ghamdi, A., 1998. Road traf®c accidents in Saudi Arabia causes, effects and solutions 1418H. General traf®c Department, Saudi Arabia.
- Ansari S., Akhdar F., Mandoorah M., Moutaery K. Causes and effects of road traf®c accidents in Saudi Arabia. Pub. Health. 2000;114:37–39. doi: 10.1038/sj.ph.1900610. [DOI] [PubMed] [Google Scholar]
- Bataineh A.B. Etiology and incidence of maxillofacial fractures in the North of Jordan. Oral Surg. Oral Med. Oral Pathol. Oral Rehabil. Radiol. Endod. 1998;86(1):31–35. doi: 10.1016/s1079-2104(98)90146-9. [DOI] [PubMed] [Google Scholar]
- Bener A., Jadaan K.S. A study on pedestrian accidents in some Gulf Countries. J. Traffic Med. 1992;21:74–78. [Google Scholar]
- Brasileiro B.F., Passeri L.A. Epidemiological analysis of maxillofacial fractures in Brazil: a 5 year prospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006;102(1):28–34. doi: 10.1016/j.tripleo.2005.07.023. [DOI] [PubMed] [Google Scholar]
- Chrcanovic B.R., Freire-Maia B., Souza L.N., Araújo V.O., Abreu M.H. Facial fractures: a 1 year retrospective study in a hospital in Belo Horizonte. Braz. Oral Res. 2004;18(4):322–328. doi: 10.1590/s1806-83242004000400009. [DOI] [PubMed] [Google Scholar]
- Gassner R., Tuli T., Hachl O., Rudisch A., Ulmer H. Craniomaxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J. Craniomaxillofac. Surg. 2003;31(1):51–61. doi: 10.1016/s1010-5182(02)00168-3. [DOI] [PubMed] [Google Scholar]
- Girotto J.A., MacKenzie E., Fowler C., Redett R., Robertson B., Manson P.N. Long-term physical impairment and functional outcomes after complex facial fractures. Plast. Reconstr. Surg. 2001;108(2):312–327. doi: 10.1097/00006534-200108000-00005. [DOI] [PubMed] [Google Scholar]
- Hagan E.H., Huelke D.E. An analysis of 319 case reports of mandibular fractures. J. Oral Surg. 1961;19:93. [PubMed] [Google Scholar]
- Haung R.H., Prather J., Indrsano T. An epidemiological survey of facial fractures and concomitant injuries. J. Oral Maxillofac. Surg. 1990;48:926–932. doi: 10.1016/0278-2391(90)90004-l. [DOI] [PubMed] [Google Scholar]
- Jadaan K.S., Bener A., Al-Zahrani A. Some aspects of road user behavior in selected Gulf countries. J. Traffic Med. 1992;20:129–135. [Google Scholar]
- Khalil A.F., Shaladi O.A. Fractures of the facial bones in Eastern region of Libya. Br. J. Oral Surg. 1981;19:300. doi: 10.1016/0007-117x(81)90051-2. [DOI] [PubMed] [Google Scholar]
- Klenk G., Kovacs A. Etiology and patterns of facial fractures in the United Arab Emirates. J. Craniomaxillofac. Surg. 2003;14(1):78–84. doi: 10.1097/00001665-200301000-00014. [DOI] [PubMed] [Google Scholar]
- Maliska M.C.S., Lima Júnior S.M., Gil J.N. Analysis of 185 maxillofacial fractures in the state of Santa Catarina. Braz. Oral Res. 2009;23(3):268–274. doi: 10.1590/s1806-83242009000300008. [DOI] [PubMed] [Google Scholar]
- Ministry of Interior, 1997. Traffic statistics: statistical publications from 1391H ± 1417H (1971 ± 1997). Ministry of Interior, General Traf®c Department, Riyadh.
- Motamedi K.H.M. An assessment of maxillofacial fractures: a 5 Year study of 237 patients. J. Oral Maxillofac. Surg. 2003;61:61–64. doi: 10.1053/joms.2003.50049. [DOI] [PubMed] [Google Scholar]
- Oikarinen K., Ignatius E., Kauppi H., Silvennoinen U. Mandibular fractures in Northern Finland in the 1980s—a 10 year study. Br. J. Oral Maxillofac. Surg. 1993;31(1):23–27. doi: 10.1016/0266-4356(93)90092-b. [DOI] [PubMed] [Google Scholar]
- Olasoji H.O., Tahir A., Arotiba G.T. Changing pictures of facial fractures in Northern Nigeria. Br. J. Oral Maxillofac. Surg. 2002;40(2):140–143. doi: 10.1054/bjom.2001.0716. [DOI] [PubMed] [Google Scholar]
- Strom C., Nordenram A., Fischer K. Jaw fractures in the county of Kopparberg and Stockholm 1979–1988. A retrospective comparative study of frequency and cause with special reference to assault. Swed. Dent. J. 1991;15(6):285–289. [PubMed] [Google Scholar]
- Tanaka N., Tomitsuka K., Shionoya K., Andou H., Kimijima Y., Tashiro T. Aetiology of maxillofacial fracture. Br. J. Oral Maxillofac. Surg. 1994;32(1):19–23. doi: 10.1016/0266-4356(94)90166-x. [DOI] [PubMed] [Google Scholar]
- Van Hoof R.F., Merkx C.A., Stekelenbrug E.C. The different patterns of fractures of the facial skeleton in four European countries. Int. J. Oral Surg. 1977;6(1):3–11. doi: 10.1016/s0300-9785(77)80066-5. [DOI] [PubMed] [Google Scholar]