

Abstract
Objectives
To test the short term clinical effectiveness of commercially available 0.07%.cetylpyridinium chloride mouth rinse in patients undergoing fixed orthodontic treatment as compared to a placebo mouth rinse and patients using toothbrush and toothpaste.
Method
Forty-five subjects for this double blind study were assigned randomly into three groups of 15 each. Gingival inflammation, plaque accumulation, and bleeding on probing, were recorded at baseline (10 days after prophylaxis), and at the end of one month in all the three groups and compared.
Results
Paired t test showed significant differences in bleeding index for pre and post treatment recordings for cetylpyridinium group. Modified gingival index showed no significant difference in the cetylpyridinium group. For plaque index significant difference was found for cetylpyridinium and control groups.
Conclusion
Cetylpyridinium mouth rinse 0.7% was found to be effective in reducing the bleeding and plaque index scores. It was not effective in reducing the modified gingival index scores. Cetylpyridinium mouth rinse 0.07% improves the oral hygiene of orthodontic patients when used as an adjunct to normal oral hygiene measures.
Keywords: Cetylpyridinium chloride, Fixed orthodontics, Gingival index, Placebo, Control group
1. Introduction
Oral hygiene maintenance is of supreme importance in patients undergoing fixed orthodontic treatment. Tooth brushing is a skill that is difficult to perfect. Orthodontic appliances protect the dental plaque from the mechanical action of brushing and mastication (Brightman et al., 1991). Patients undergoing fixed orthodontic appliance treatment have elevated levels of Streptococcus mutans (Rosenbloom and Tinanoff, 1991), Candida species and Enterobacteriaceae (Hägg et al., 2004). Undisturbed supragingival plaque initiates gingival inflammation further leading to gingivitis and gingival hyperplasia (Morrow et al., 1992).
Various chemical agents are used during the active phase of orthodontic treatment to reduce the bacterial plaque accumulation and decrease the occurrence of periodontal disease in these patients. These chemical agents are used adjunctively for orthodontic patients who have difficulty maintaining plaque control by mechanical means alone (Brightman et al., 1991). Some commonly used chemical plaque control agents are chlorhexidine, cetylpyridinium chloride, listerine, triclosan, etc.
Cetylpyridinium chloride is a quaternary ammonium compound and is used in a wide variety of antiseptic mouth rinse products at a concentration of 0.07%. Daily rinsing with cetylpyridinium significantly reduces the clinical evidence of gingival inflammation (Kiszely and et al., 2007). However, the effect of cetylpyridinium used as an adjunct with regular oral hygiene procedures in patients undergoing fixed orthodontic treatment has been lacking.
2. Aims and objectives
To test the short term clinical effectiveness of commercially available 0.07% cetylpyridinium chloride mouth rinse in patients undergoing fixed orthodontic treatment as compared to a placebo mouth rinse and patients using toothbrush and toothpaste.
2.1. Materials and method
Forty-five subjects for this study were selected from Department of Orthodontics and Dentofacial Orthopedics, in Outpatient Department, Dental College.
The following inclusion criteria were used for patient selection:
-
a.
Patients in 11–25 year age group.
-
b.
Initial leveling and alignment completed.
-
c.
Patient undergoing fixed orthodontic treatment with brackets on their anterior teeth and bands on their molars.
The following exclusion criteria were used for patient selection:
-
a.
No evidence of decalcification of teeth should be present.
-
b.
No known hypersensitivity to cetylpyridinium (CI).
-
c.
No known medical problem or taking any medication that may have an effect on oral tissues.
-
d.
No anterior composites should be present.
Prior consent was taken from all the subjects participating in the study. They were also given one month free supply of mouth rinse at the end of the study.
2.2. Experimental design
The study was a double blind study. Two tables of random numbers, one for the male population and one for the female population were used, and the subjects were assigned to one of the treatment groups, i.e., cetylpyridinium Group-1, Placebo Group-2 and Brushing Group-3 after they have received a thorough dental prophylaxis which included removal of plaque, calculus and stains. Mean age for subjects in the study was calculated to be 14.8 years. There were 25 female and 20 male patients.
2.3. Preparation of the placebo mouth wash
Placebo mouthwash was prepared according to the under mentioned formula:
| a. | Glycerin | 40 ml |
| b. | Peppermint water | 0.5 ml |
| c. | Ethylene blue | 0.3 ml |
| d. | Distilled water | up to 60 ml |
These ingredients in the quantities mentioned are sufficient to produce 100 ml of mouthwash (Fig. 1).
Figure 1.

Ingredients for preparation of placebo mouth wash.
2.4. Dosage regimen
Each patient in this study was provided with one orthodontic toothbrush (Stim-MB), one tube of Colgate (Total) toothpaste with fluoride and three 200 ml bottles of cetylpyridinium chloride. These quantities were determined to be sufficient for a one month investigation (Fig. 2).
Figure 2.
Stim Ortho MB toothbrush (A). Colgate total toothpaste (B). Crest pro health mouthwash (C).
The patients were instructed to brush only with Colgate toothpaste with fluoride and Stim orthodontic toothbrush once in the morning after breakfast and once in the evening before bed time. They were instructed to brush a minimum of 3 min to ensure thorough brushing. They were then given a cooperation table on which they marked only the times that they completed mouth rinsing. They were told not to mark the table if they forgot to use the mouth rinse.
The mouth rinses were used by different groups after tooth brushing according to the following regimen:
| Dose-1 | Dose-2 | |
|---|---|---|
| Group-1 | 10 ml of cetylpyridinium (Crest pro health) for 60 s 30 min after breakfast | 10 ml of cetylpyridinium (Crest pro health) for 60 s before bedtime |
| Group-2 | Brushing with toothpaste and toothbrush for 3 min after breakfast | Brushing with toothpaste and toothbrush for 3 min before bedtime |
| Group-3 | 10 ml of placebo for 60 s after breakfast | 10 ml of placebo for 60 s before bedtime |
The subjects were instructed not to take any liquid or food into the mouth for at least 30 min after using the prescribed mouth rinse.
2.5. Reports and records
Gingival inflammation, plaque accumulation, and bleeding on probing were recorded at baseline (10 days after prophylaxis), and at the end of one month by a clinical examiner who is an assistant professor in Periodontics. This was done to avoid errors in recording these indices (Fig. 3).
Figure 3.
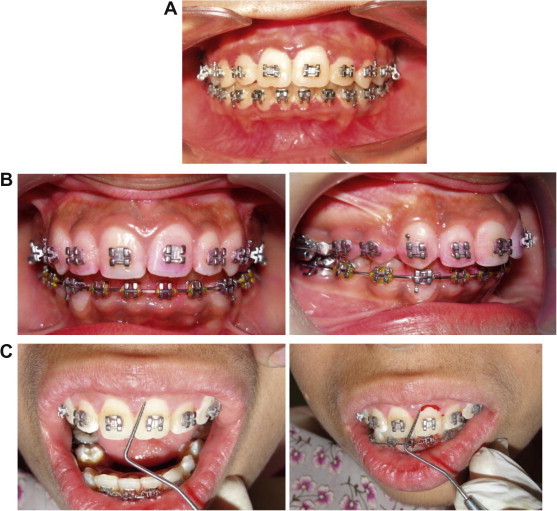
Inflammation of the marginal gingiva (A). Plaque deposits become visible after the application of disclosing solution (B). Blunt periodontal probe being used to check bleeding on probing (C).
The modified gingival index was used to determine the health and degree of inflammation of the marginal gingiva. The labial/facial and lingual surface of the gingival margins and the interdental papillae of six teeth (16, 12, 24, 36, 32 and 44) were scored as described by Lobene et al. (1986) (if first premolars were extracted for orthodontic purposes then second premolars were considered).
The plaque index (PI) was used to determine the amount of plaque on the tooth surface. The mesiofacial, facial, distofacial, and lingual surfaces of the same teeth used in the gingival index were scored as described by Silness and Loe (1964).
The gingival bleeding index was used to determine the presence or the absence of bleeding. The same six teeth that were assessed in the gingival and plaque indices were assessed for this index as described by Ainamo and Bay (1975).
The statistical analysis was carried out using Microsoft Excel 2003 software. The 5% level of significance was adopted for the present study:
| p < 0.05 | Statistically significant |
| p > 0.05 | Statistically not significant |
The statistical data was summarized in table form, analyzed and interpreted.
3. Results
Base line data for the mean gingival bleeding index (Table 1A) mean modified gingival index (Table 1B) and the mean plaque index (Table 1C) show that the three groups were well matched and were the same at the beginning of the study.
Table 1.
Descriptive statistics of gingival bleeding index, modified gingival index, and plaque index of different groups at baseline (10 days after prophylaxis).
| Group | No of subjects (N) | Mean | STD | Sum | S.E.M. |
|---|---|---|---|---|---|
| (A) | |||||
| Cetylpyridinium | 15 | 0.19 | 0.090 | 2.85 | 0.0232 |
| Toothbrush/toothpaste | 15 | 0.268 | 0.871 | 4.02 | 0.225 |
| Control | 15 | 0.154 | 0.078 | 2.31 | 0.020 |
| (B) | |||||
| Cetylpyridinium | 15 | 1.099 | 0.1844 | 16.49 | 0.0476 |
| Toothbrush/toothpaste | 15 | 1.0425 | 0.368 | 8.34 | 0.095 |
| Control | 15 | 0.9733 | 0.2237 | 14.6 | 0.0577 |
| (C) | |||||
| Cetylpyridinium | 15 | 1.0226 | 0.0894 | 15.34 | 0.0230 |
| Toothbrush/toothpaste | 15 | 0.734 | 0.3470 | 11.01 | 0.0895 |
| Control | 15 | 0.95 | 0.1571 | 14.25 | 0.0405 |
Paired ‘t’ test for gingival bleeding index (Table 2A) showed significant difference between pre and post treatment observations at 0.05% and 0.01% level of significance with respect to cetylpyridinium groups and no significant difference were found for the toothbrush/toothpaste group and the control group.
Table 2.
Paired t test for gingival bleeding index (A), modified gingival index (B) and for plaque index (C).
| Group | Mean ± S.D. Scores | “t” Value | At 0.05 level | At 0.01 level |
|---|---|---|---|---|
| (A) | ||||
| Cetylpyridinium | −0.15 ± 0.088721 | 6.5502 | S∗ | S∗ |
| Toothpaste/toothbrush | −0.05533 ± 0.194784 | 1.0994 | NS | NS |
| Control | 0.028 ± 0.046935 | 2.3141 | NS | NS |
| (B) | ||||
| Cetylpyridinium | −0.25867 ± 0.152262 | 1.4832 | NS | NS |
| Toothpaste/toothbrush | 0.141333 ± 0.333785 | 1.6396 | NS | NS |
| Control | 0.028667 ± 0.070495 | 1.5751 | NS | NS |
| (C) | ||||
| Cetylpyridinium | −0.25867 ± 0.152262 | 1.4832 | NS | NS |
| Toothpaste/toothbrush | 0.141333 ± 0.333785 | 1.6396 | NS | NS |
| Control | 0.028667 ± 0.070495 | 1.5751 | NS | NS |
Paired ‘t’ test for modified gingival index (Table 2B) showed no significant difference between pre and post treatment observations at 0.05% and 0.01% level of significance with respect to cetylpyridinium, toothbrush/toothpaste group and the control group.
Paired ‘t’ test for plaque index (Table 2C) showed significant difference between pre and post observations at 0.05% and 0.01% level of significance with respect to cetylpyridinium, and the control group and no significant difference was found for the toothbrush/toothpaste group.
Anova for post treatment gingival bleeding index (Table 3A) among groups showed significant difference among all the three groups. Fcal was found to be greater than Ftab at 0.05 level of significance.
Anova for post treatment Modified gingival index (Table 3B) among groups showed no significant difference among all the three groups. Fcal was found to be less than Ftab at 0.05% and 0.01% level of significance.
Anova for post treatment plaque index (Table 3C) among groups showed significant difference among all the three groups. Fcal was found to be greater than Ftab at 0.05% and 0.01% level of significance.
Graphical representation (Graph 1A) in the mean bleeding index scores at the end of one month shows that cetylpyridinium and toothbrush/toothpaste were able to reduce the scores after one month of use by the subjects resulting in an improvement in gingival health.
Graph 1.
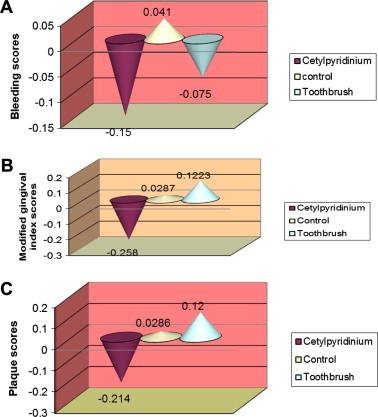
Mean change in bleeding index scores at the end of one month (A). Mean change in Modified gingival index scores at the end of one month (B). Mean change in plaque index scores at the end of one month (C).
Graphical representation (Graph 1B) in the mean Modified index scores at the end of one month shows that cetylpyridinium was able to reduce the scores after one month of use by the subjects. In control and toothbrush/toothpaste group there was an increase in scores indicating no improvement in gingival health.
Graphical representation (Graph 1C) in the mean plaque index scores at the end of one month shows that cetylpyridinium was able to reduce the scores after one month of use by the subjects. In control and toothbrush/toothpaste group there was an increase in scores indicating no improvement in plaque control.
4. Discussion
One of the objectives of orthodontic treatment is to promote better dental health and prolong the life of the dentition by creating an ideal occlusion thereby easing the task of maintaining a high level of oral hygiene (Ainamo and Bay, 1975). However, the presence of the fixed appliances in the oral cavity creates difficulty in maintenance of the oral hygiene by tooth brushing alone (Brightman et al., 1991). To overcome this, various chemical agents are used during the active phase of orthodontic treatment to reduce the bacterial plaque accumulation and decrease the occurrence of periodontal disease in these patients. Present study was done to ascertain the role of cetylpyridinium chloride as an adjunct to regular oral hygiene measures in improving oral hygiene in patients undergoing fixed appliance orthodontic treatment as compared to tooth brushing alone and to a control.
Cetylpyridinium chloride (CPC) is a member of the quaternary ammonium compounds and is the active agent in several commercially-available mouth rinses (Hancock, 1998). One of the advantages of cetylpyridinium chloride is that it is mono cationic at oral Phand adsorbs readily and quantitatively to a greater extent than chlorhexidine, to oral surfaces (Quirynen et al., 2005). Cetylpyridinium binds to the phosphate groups of lipids in cell walls of bacteria. It penetrates the cell and causes general membrane damage (Sreenivasan and Gaffar, 2002). Cell membrane damage leads to leakage of cell components, disruption of bacterial metabolism, inhibition of cell growth, and finally cell death (Quirynen et al., 2005).
Side effects of quaternary ammonium compound include staining, alteration of taste and burning sensation (Ciancio, 1992). The effect of cetylpyridinium chloride at concentrations of 1:1000 and 1:2000 on gingivitis and plaque were studied over a 21 day period by Lobene, 1979). Subjects practiced customary tooth brushing and rinsed with 20 ml of cetylpyridinium chloride for 20 s, twice daily for 21 days. Witt et al. Witt et al. (2005) did a study on the antibacterial and antiplaque effects of a novel, alcohol free oral rinse with cetylpyridinium chloride. They concluded that the cetylpyridinium mouth rinse showed a wide spectrum of antimicrobial activity.
This study evaluated the clinical effectiveness of 0.07% cetylpyridinium chloride mouth rinses in orthodontic patients 11–25 year age group, during a one month period of twice daily use. All the subjects were brought to baseline by giving them a thorough prophylaxis and they were given oral hygiene instructions at the beginning of the study.
The outcome of the current study indicate that the use of chemical mouth rinses as adjuncts to regular oral hygiene practice was effective in reducing plaque and gingivitis thereby improving the oral health during the experimental period of 30 days. It is important to point out that the study was a double blind study and the study population of all the three groups was determined by random assignment.
Cetylpyridinium improved the bleeding scores (an indicator of gingival health) when used in addition to regular oral hygiene practice. These results seem to be in agreement with the previous studies where cetylpyridinium was used (Mankodi et al., 2005; Roberts and Addy, 1981). There was no improvement in the bleeding scores in the control and the tooth brushing group.
Cetylpyridinium chloride did not appear to improve inflammation of the marginal gingiva. This finding is in agreement with that of Holbeche et al. (1975). This finding needs to be studied further by undertaking a long term study. One of the possible reasons could be the low substantivity of cetylpyridinium chloride.
Tooth brushing and the control group did not show any significant improvement in the gingival index scores as is apparent from the post treatment mean plaque scores and as evidenced by the paired t test. These findings were as expected.
Use of cetylpyridinium chloride resulted in a significant reduction in the plaque scores as measured by the plaque index. This was in agreement with the earlier findings of Holbeche et al. (1975), Mankodi et al. (2005), and Kiszely and et al., 2007.
The control group also showed an improvement in the plaque scores and the results of the statistical analysis were found to be significant which is in contrast to the expected result. A possible explanation for improvement in the plaque scores could be because of the so called ‘Hawthorne effect’ (Newman et al., 2006) (the term was coined by Henry A. Landsberger in 1955) when he was analyzing older experiments from 1924 to 1932 at the Hawthorne works factory. The Hawthorne effect is a form of reactivity whereby subjects improve an aspect of their behavior being experimentally measured simply in response to the fact that they are being studied, not in response to any particular experimental manipulation. There was no improvement in the plaque scores of tooth brushing group and these results are as expected.
The establishment of a long term preventive program has been suggested in the literature, taking into account the difficult task of plaque control especially in the younger age group. In a longitudinal study done by Zachrisson and Zachrisson (1972) on the gingival conditions of the young patients (ages 11–13 years) treated with fixed orthodontic appliances, it was found that despite repeated motivation in brushing technique and sodium fluoride rinses twice weekly, most of the subjects developed generalized hyperplastic gingivitis within one to two months after placement of appliances. Therefore, a thorough homecare program that includes direct involvement with the youth’s parents is desirable as has been suggested by Kloehn and Pfeiffer (1974).
Finally, the use of chemical agents can be used as a motivating factor for patients as has been suggested by Ainamo (1977). It would make patients aware of sensation of cleanliness so they could learn to develop their mechanical abilities for maintaining oral hygiene.
Long term effects of cetylpyridinium chloride have not been evaluated in orthodontic patients. Therefore it is suggested to assess the long term significance of using cetylpyridinium chloride in orthodontic patients.
5. Conclusion
The following conclusions were drawn from the study:
-
1.
Supplementing oral hygiene with a chemical plaque control agent in addition to regular oral hygiene measures in all cases undergoing fixed orthodontic treatment resulted in an improvement in the reduction in plaque scores and thereby an improvement in the health of the periodontium.
-
2.
Cetylpyridinium mouth rinse 0.07% was found to be effective in reducing the bleeding and plaque index scores. It was not effective in reducing the modified gingival index scores.
-
3.
Control and tooth brushing groups did not show any significant improvement in the bleeding, modified gingival index and the plaque scores.
Further research is recommended to study the long term effects of chemical plaque control agents in improving the oral hygiene of patients undergoing fixed appliance therapy.
Acknowledgment
Sincere thanks for providing unending support during the study to Dr. Ashvarya Sahni, Physical Therapist, Skilled Nursing Facility, Lawrence Health Care Center, Tom Ball, Texas, USA.
References
- Ainamo J. Control of plaque by chemical agents. J. Clin. Periodontol. 1977;4:23–25. doi: 10.1111/j.1600-051x.1977.tb00049.x. [DOI] [PubMed] [Google Scholar]
- Ainamo J., Bay I. Problems and proposals for recording gingivitis and plaque. J. Clin. Periodontol. 1975;25(4):229–236. [PubMed] [Google Scholar]
- Brightman L.J., Terezhalmy G.T., Greenwell H., Jacobs M., Enlow D.H. The effects of 0.12% chlorhexidine Gluconate mouthrinse on orthodontic patients aged 11 through 17 with established gingivitis. Am. J. Orthod. Dentofac. Orthop. 1991;100:380–388. doi: 10.1016/0889-5406(91)70069-9. [DOI] [PubMed] [Google Scholar]
- Ciancio S.G. Agents for the management of plaque and gingivitis. J. Dent. Res. 1992;71:1450–1454. doi: 10.1177/00220345920710071701. [DOI] [PubMed] [Google Scholar]
- Hägg U., Kaveewatcharanont P., Samarnayake Y.H., Samarnayake L.P. The effect of fixed orthodontic appliances on the oral carriage of Candida species and Enterobacteriaceae. Eur. J. Orthod. 2004;26:623–629. doi: 10.1093/ejo/26.6.623. [DOI] [PubMed] [Google Scholar]
- Hancock E.B. Prevention. J. Periodontol. 1998;1:223–249. doi: 10.1902/annals.1996.1.1.223. [DOI] [PubMed] [Google Scholar]
- Holbeche J.D., Ruljancich M.K., Reade P.C. A clinical trial of the efficacy of a cetylpyridinium chloride mouthwash: effect on plaque accumulation and gingival condition. Aust. Dent. J. 1975;6:397–404. doi: 10.1111/j.1834-7819.1975.tb04390.x. [DOI] [PubMed] [Google Scholar]
- Kiszely A. Comparison of the effects of cetylpyridinium chloride with an essential oil mouthrinse on dental plaque and gingivitis – a six month randomized control trial. J. Clin. Periodontol. 2007;34:658–667. doi: 10.1111/j.1600-051X.2007.01103.x. [DOI] [PubMed] [Google Scholar]
- Kloehn J.S., Pfeiffer J.S. The effect of orthodontic treatment on the periodontium. Angle Orthod. 1974;44:127–134. doi: 10.1043/0003-3219(1974)044<0127:TEOOTO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Lobene R.R. Clinical studies of plaque control agents: an overview. J. Dent. Res. 1979;58(12):2381–2388. doi: 10.1177/00220345790580120902. [DOI] [PubMed] [Google Scholar]
- Lobene R.R., Weatherford T., Ross N.M., Menaker R.A. Amodified gingival lindex for use in clinical trials. Clin. Prev. Dent. 1986;8(1):3–6. [PubMed] [Google Scholar]
- Mankodi S., Bauroth K., Witt J.J., Bsoul S., He T., Gibb R., Dunavent J., Hamilton A. A six month clinical trial to study the effects of a cetylpyridinium chloride mouthrinse on gingivitis and plaque. Am. J. Dent. 2005;18:9A–14A. [PubMed] [Google Scholar]
- Morrow D., Wood P.D., Speechley M. Clinical effect of subgingival chlorhexidine irrigation on gingivitis in adolescent orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 1992;101:408–413. doi: 10.1016/0889-5406(92)70113-O. [DOI] [PubMed] [Google Scholar]
- Newman M.G., Takei H.H., Klokkevold P.R., Carranza F.A. 10th ed. Saunders; 2006. Clinical Periodontology. pp. 471–481. [Google Scholar]
- Quirynen M., Soers C., Desnyder M., Pauwels M., Steenberghe D.V. A 0.05% cetylpyridinium chloride/chlorhexidine mouthrinse during maintenance phase after initial periodontal therapy. J. Clin. Periodontol. 2005;32:390–400. doi: 10.1111/j.1600-051X.2005.00685.x. [DOI] [PubMed] [Google Scholar]
- Roberts W.R., Addy M. Comparison of the in vivo and in vitro antibacterial properties of antiseptic mouthrinse containing chlorhexidine, alexidine, cetylpyridinium chloride and hexitidine. Relevance to mode of action. J. Clin. Periodontol. 1981;8(4):295–310. doi: 10.1111/j.1600-051x.1981.tb02040.x. [DOI] [PubMed] [Google Scholar]
- Rosenbloom R.G., Tinanoff N. Salivary Streptococcus mutans levels in patients before during and after orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1991;100:35–37. doi: 10.1016/0889-5406(91)70046-Y. [DOI] [PubMed] [Google Scholar]
- Silness J., Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol. Scand. 1964;22:121–135. doi: 10.3109/00016356408993968. [DOI] [PubMed] [Google Scholar]
- Sreenivasan P., Gaffar A. Antiplaque biocides and bacterial resistance: a review. J. Clin. Periodontol. 2002;29:965–974. doi: 10.1034/j.1600-051x.2002.291101.x. [DOI] [PubMed] [Google Scholar]
- Witt J., Ramji N., Gibb R., Dunavent J., Flood J., Barnes J. Antibacterial and antiplaque effects of a novel, alcohol free oral rinse with cetylpyridinium chloride. J. Contemp. Dent. Pract. 2005;6:15. [PubMed] [Google Scholar]
- Zachrisson S., Zachrisson B.U. Gingival condition associated with orthodontic treatment. Angle Orthod. 1972;42:26–34. doi: 10.1043/0003-3219(1972)042<0026:GCAWOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]