

Abstract
Diverticular disease of the colon is a common disease, mainly in the population over 50 years of age. In acute forms of presentation, we considered home treatment in those patients that were classified as having uncomplicated forms by means of clinical presentation and a computed tomography of the abdomen. According to these criteria, we treated 38 patients at home and admitted 18 patients to the hospital during the same period of time. No severe complications developed in the home-treatment patients. Home treatment is an effective alternative treatment for patients with uncomplicated acute diverticulitis. In uncomplicated acute diverticulitis, home treatment benefits the patient, over hospitalization, by allowing better management of resources and by keeping the patient in a familiar environment where there is no risk of a nosocomial infection.
Keywords: Diverticular disease of the colon, Home treatment, Sigmoid diverticulitis, Ertapenem, Retrospective study
Diverticular disease of the colon (DDC) has a prevalence of 5% to 25% in the population over 40 years of age and rises to 60% at age 60. Twenty percent of patients with DDC will present with an episode of acute diverticulitis (AD) during their lifetime.1–4
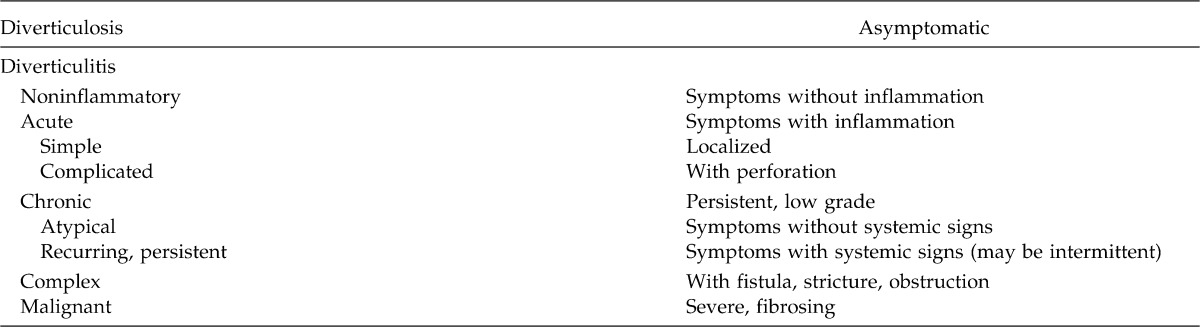
University Hospital's Joan XXIII General Surgery Department treats both acute and chronic DDC, as well as the recurring manifestations needing treatment. The DDC includes the acute forms, both simple and complicated. For the past 10 years, the Home Care Unit (HCU) of our hospital has undertaken ambulatory treatment of patients affected by medical and surgical pathologies. AD in its uncomplicated forms is included in the diseases to be treated on an outpatient basis. To select patients, we used the American Society of Colorectal Surgeons classification, which includes patients with mild or moderate acute diverticulitis (Table 1). The purpose of this article is to confirm the effectiveness of outpatient care of uncomplicated AD.
Table 1.
The classification of diverticular disease by the American Society of Colorectal Surgeons
Materials and Methods
A retrospective study was performed of cases of AD treated in the Joan's XXIII Hospital of Tarragona General Surgery Service Department, from October 2008 to December 2010. We reviewed 56 cases of which 38 had been treated at home through the Home Care Unit and 18 had been hospitalized.
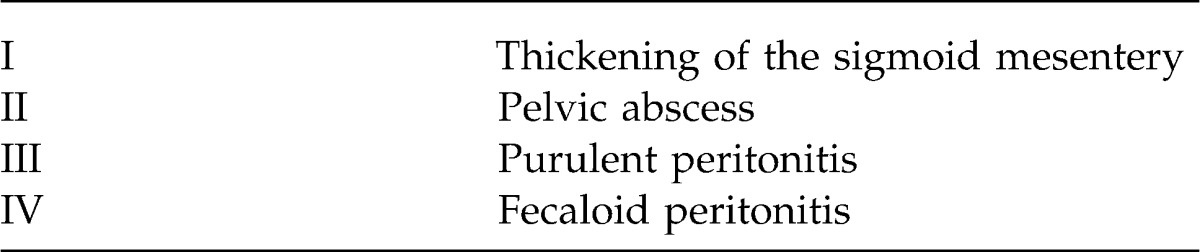
Patients presented with clinical signs compatible with AD. Abdominal pain in the left iliac fossa with or without associated fever was the most frequent reason for consultation. Among the complementary tests were a complete analysis with complete blood count (CBC), coagulation, and biochemistry; simple chest and abdomen X-rays to rule out intestinal obstruction and pneumoperitoneum; and a computed tomography (CT) scan of the abdomen to confirm the diagnosis of AD. To classify diverticulitis, we used the Hinchey classification: candidates for home care had a Hinchey I or II (Table 2).5 Both groups (home-treatment and hospitalized patients) received the same antibiotic dosage: Ertapenem 1 g intravenous every 24 hours.
Table 2.
Hinchey's classification
Sixteen variables were evaluated by univariate and multivariate analysis. We used the statistical program SPSS 18th version. The protocol for the inclusion of patients in the Home Care Unit was as follows:
Age: Patients younger than 80 years of age who presented in good general health.
ASA I–II.
Patients presented with clinical signs suggesting the existence of AD and absence of clinical signs of complications such as peritonitis, vomiting, or severe abdominal distention.
CT indicating Hinchey I to II.
Social: Family could provide proper environment.
Patient's will: The patient agreed to receive home care and understood that they maintained contact with the hospital with this treatment modality.
Results
Analysis included sex, age, and duration of treatment. Regarding the sex variables, there was no significant difference in sex distribution between treatment modalities. There was a significantly higher incidence of the disease in women in both groups (Fig. 1). The average age of treated patients was 61.33 years for hospitalized patients and 63.97 years for home-treatment patients, with no significant differences between them (Fig. 2). Younger patients were hospitalized in greater numbers. Regarding treatment days, no differences were found between the groups; the average treatment was approximately 10 days. However, analysis revealed that the hospitalized patients received treatment for more days, while the HCU patients had an average of 10 days. This finding leads us to believe that the selection criteria for home care are appropriate (Fig. 3).
Fig. 1.
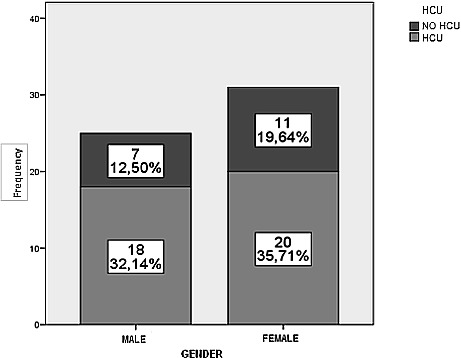
Sex and frequency. HCU, home care unit; No HCU, patients admitted to the hospital.
Fig. 2.
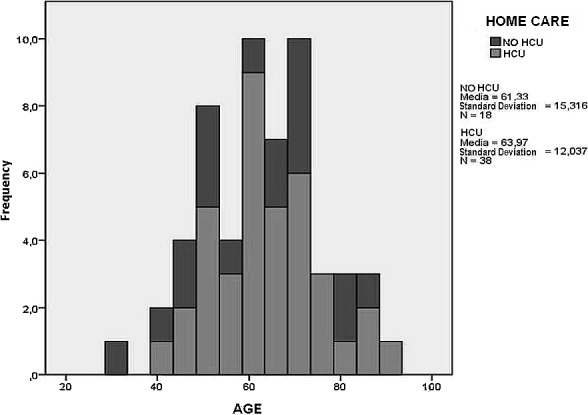
Age and frequency.
Fig. 3.
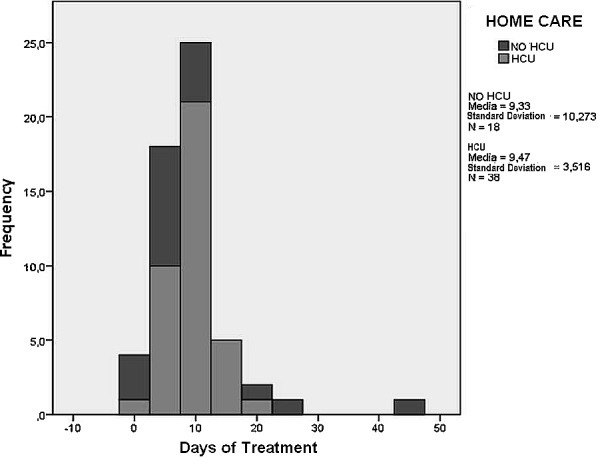
Days of treatment and frequency.
We attempted an analysis of the possible factors for readmission of these patients. The percentage of patients from both treatment groups who were readmitted to the hospital is similar, approximately 20% (Table 3), with no significant differences between them (Fig. 4). In analyzing the comorbidities present in patients, we examined those that seemed to influence the severity of the diverticulitis. Chronic renal failure, diabetes mellitus, ischemic heart disease, chronic obstructive pulmonary disease, and treatment with corticosteroids appear to be the most relevant. The percentage of absolute numbers in our series is very small; to achieve better statistic effectiveness, we have grouped it into a single variable called “comorbidity” (Fig. 5). Doing a multivariate analysis, we can see in both groups (home-treatment and hospitalized patients) that age could be a favoring factor to readmission. The same occurs with the fever variable (Table 4). On this premise, we arbitrarily defined a cutoff line at 70 years of age and analyzed the results. When considering both groups, the home-treatment group and the hospitalized group, together, the proportion of hospital readmissions is higher in patients over 70 years of age (Fig. 6). Even if we consider only home-treatment patients, there is a higher proportion of hospital readmissions in the patients over 70 years of age (Fig. 7).
Table 3.
Readmissions considered in both groups: admitted versus home-treatment patients

Fig. 4.
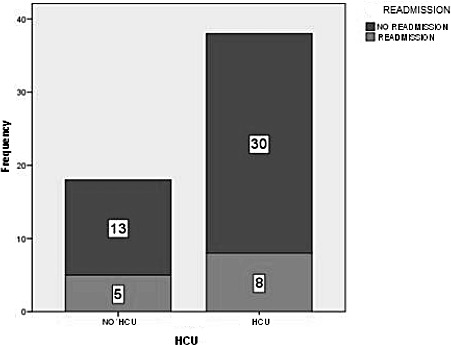
No readmission versus readmission.
Fig. 5.
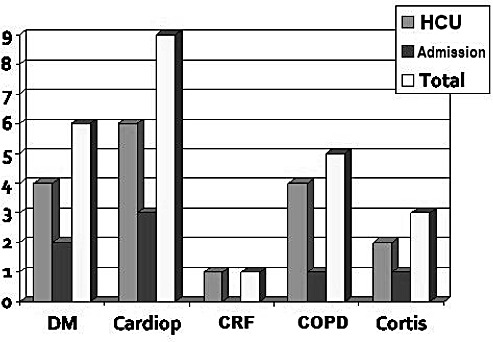
Comorbidities. DM, diabetes mellitus; cardiop, heart disease; CRF, chronic renal failure; COPD, chronic obstructive pulmonary disease; cortis, patients in treatment with steroids.
Table 4.
Multivariate analysis in both groups: age and fever could be a favoring factor to reentry
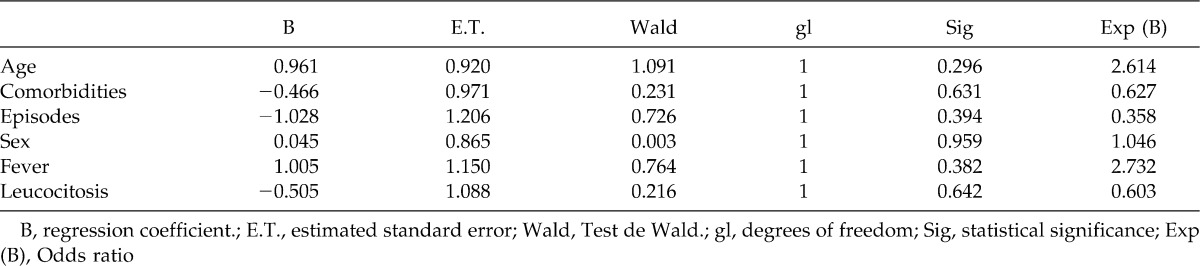
Fig. 6.
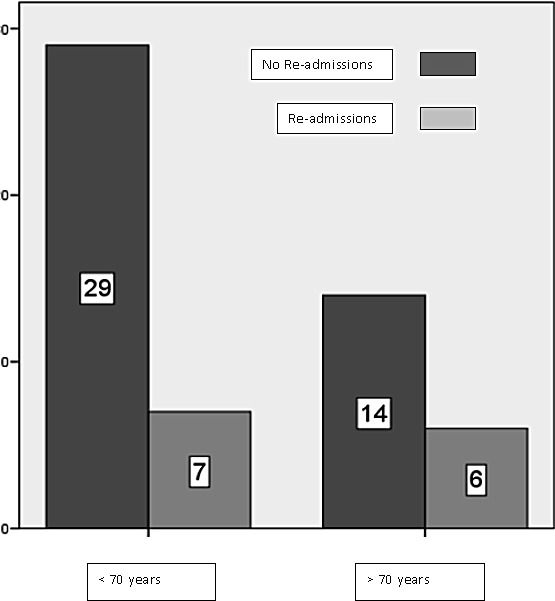
Readmissions, comparing patients under 70 years of age with those over 70. Both groups, home-treatment and hospitalized, considered together.
Fig. 7.
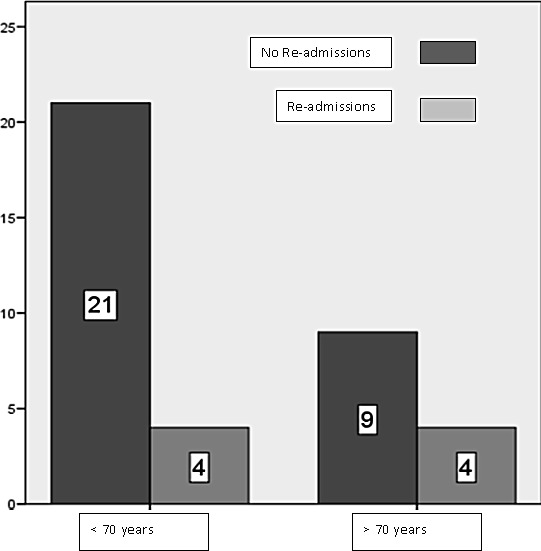
Readmissions, considering only home-treatment patients.
Discussion
Uncomplicated acute diverticulitis is the most common complication of DDC.1,3,4 In our hospital, which has a Home Care Unit, patients with complicated forms of acute diverticulitis can receive ambulatory treatment.
The results of our analysis show that the patients' readmission rate is approximately 20% to 30% in both treatment groups, consistent with the results estimated as acceptable in the literature.6,7 We found that younger patients often required hospitalization more often, either for diagnostic purposes, or because they presented with more severe forms of the disease.8 We analyzed the predictors for readmission, but because our series is small, no trend reached statistical significance. It is possible that a larger series, in the future, will allow us to select the variables that constrain or facilitate readmission so that strategies can be developed to avoid them.
Despite the lack of consensus on the indications of elective surgery after the second or third episode of AD, the need for surgery is highly predictable in those patients who present with their first episode when they are approximately 40 years of age, especially if they are male. In the same way, patients who relapse with progressively more aggressive forms should be candidates for elective surgery if their comorbidities allow it.
Recently, a prospective randomized trial was conducted comparing a shorter-term antibiotic therapy with Ertapenem. Four days therapy was as effective as the standard therapy of 7 days for treatment of uncomplicated sigmoid diverticulitis.9
We conclude that home treatment is an effective alternative for patients with uncomplicated acute diverticulitis. It benefits the patient by better management of resources and by providing a familiar environment where the patient feels safe and has no risk of a nosocomial infection.
References
- 1.Alonso S., Pera M., Parés D., et al. Outpatient treatment of patients with uncomplicated acute diverticulitis. Colorectal Dis. 2010;12(10):e278–e282. doi: 10.1111/j.1463-1318.2009.02122.x. Available at: http://onlinelibrary.wiley.com/doi/10.1111/j.1463-1318.2009.02122.x/full. Accessed Month day, year. [DOI] [PubMed] [Google Scholar]
- 2.Rodríguez-Cerrillo M., Poza-Montoro A., Fernandez-Diaz E., Iñurrieta-Romero A., Matesanz-David M., et al. Patients with uncomplicated diverticulitis and comorbidity can be treated at home. Eur J Int Med. 2010;21(6):553–554. doi: 10.1016/j.ejim.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 3.Martin Gil J., Serralta of Colsa D., García Marín A., Vaquero Rodríguez A., Rey Valcárcel C., Pérez Díaz M. D., et al. Efficiency and safety of outpatient treatment of acute diverticulitis. Gastroenterol Hepatol. 2009;32(2):83–87. doi: 10.1016/j.gastrohep.2008.10.005. [DOI] [PubMed] [Google Scholar]
- 4.Peláez N., Pera M., Courtiera R., Sánchez J., José Gil M., Parés D., Grande L., et al. Applicability, safety and efficacy of a protocol of outpatient treatment of uncomplicated acute diverticulitis [in Spanish] Cir Esp. 2006;80(6):369–372. doi: 10.1016/s0009-739x(06)70989-7. [DOI] [PubMed] [Google Scholar]
- 5.Dozois E. J. Operative treatment of complicated or recurrent diverticulitis. J Gastrointest Surg. 2008;12(8):1321–1323. doi: 10.1007/s11605-008-0488-9. [DOI] [PubMed] [Google Scholar]
- 6.Salem T. A., Molloy R. G., O'Dwyer P. J. Prospective study on the management of patients with complicated diverticular disease. Colorectal Dis. 2006;8(3):173–176. doi: 10.1111/j.1463-1318.2005.00865.x. [DOI] [PubMed] [Google Scholar]
- 7.Stollman N. H., Raskin J. B. Diagnosis and management of diverticular disease of the colon in adults. Am J Gastroenterology. 1999;94(11):3110–3121. doi: 10.1111/j.1572-0241.1999.01501.x. [DOI] [PubMed] [Google Scholar]
- 8.Thorson A. G., Goldberg . Benign colon: diverticular disease. In: Beck D. E., Roberts P. L., Saclarides T. J., Senagore A. J., Stamos M. J., Wexner S. D., editors. The ASCRS Textbook of Colon and Rectal Surgery. New York Dordretch Heidelberg, London: Springer Science and Business Media, LLC; 2011. pp. 375–393. [Google Scholar]
- 9.Schug-Pass C., Geers P., Hügel O., Lippert H., Köckerling F. Prospective randomized trial comparing short-term antibiotic therapy versus standard therapy for acute uncomplicated sigmoid diverticulitis. Int J Colorectal Dis. 2010;25(6):751–759. doi: 10.1007/s00384-010-0899-4. [DOI] [PubMed] [Google Scholar]