

Abstract
Background/Aims
Acute complicated diverticulitis can be subdivided into moderate diverticulitis and severe diverticulitis. Although there have been numerous studies on the risk factors for complicated diverticulitis, little research has focused on severe diverticulitis. This study was designed to identify the risk factors for severe diverticulitis in an acute diverticulitis attack using the modified Hinchey classification.
Methods
Patients were included if they had any evidence of acute diverticulitis detected by computed tomography. The patients were subdivided into severe diverticulitis (Hinchey class ≥Ib; abscesses or peritonitis) and moderate diverticulitis (Hinchey class Ia; pericolic inflammation) groups.
Results
Of the 128 patients, 25 exhibited severe diverticulitis, and 103 exhibited moderate diverticulitis. In a multivariate analysis, age >50 years (odds ratio [OR], 5.27; p=0.017), smoking (OR, 3.61; p=0.044), comorbidity (OR, 4.98; p=0.045), leukocytosis (OR, 7.70; p=0.003), recurrence (OR, 4.95; p=0.032), and left-sided diverticulitis (OR, 6.92; p=0.006) were significantly associated with severe diverticulitis.
Conclusions
This study suggests that the risk factors for severe diverticulitis are age >50 years, smoking, comorbidity, leukocytosis, recurrent episodes, and left-sided diverticulitis.
Keywords: Diverticulitis, Severity, Computed tomography, Hinchey classification
INTRODUCTION
Acute colonic diverticulitis is a disease with a wide range of clinical presentations ranging from mild, subclinical inflammation to generalized peritonitis. Most cases of acute diverticulitis are simple, uncomplicated, and recover well with restriction of oral intake and antibiotics. However, 25% of acute diverticulitis cases progress to complicated diverticulitis with risk of phlegmon, abscess, fistula, obstruction, bleeding, or perforation.1 Among complicated diverticulitis, the mortality rate of diverticulitis with abscess or perforation reaches 2.3%, while the mortality rate of phlegmonous diverticulitis is essentially zero.2,3 Complicated diverticulitis with abscess or perforation usually requires more intensive management such as percutaneous drainage or operative intervention, and prolonged hospital stays. Therefore, complicated diverticulitis could be subdivided into moderate diverticulitis (MD; phlegmonous type) and severe diverticulitis (SD; abscess or perforation type) with regard to patient management and prognosis.
Numerous studies have attempted to identify risk factors for poor outcome in acute diverticulitis. These studies, however, employed different clinical categories and various diagnostic methods for complicated diverticulitis instead of examining single, well-defined conditions.4 These discrepancies make it difficult to comprehensively compare the results of studies.
Computed tomography (CT) imaging is the most preferable diagnostic method in acute colonic diverticulitis, with a high sensitivity of 93% to 97% and specificity of up to 100%.5,6 Intramural inflammation, the degree of pericolic and intraperitoneal inflammation, abscess, and perforation can all be captured on CT scan. CT can also be predictive of future complications after initial medical treatment and can predict the need for surgical intervention following acute presentation. Therefore, CT is very important in surgical planning.7 Hinchey classification is commonly used in grading the severity of acute diverticulitis on CT scan; stage Ia is indicative of confined pericolic inflammation (phlegmon), whereas stages Ib, II, III, and IV indicate the presence of an abscess or peritonitis. The morbidity and mortality gradually increase with stage. Mortality is as low as 5% in stages I or II, but it increases to 13% in stage III and 43% in stage IV.8 This study was designed to identify the risk factors associated with SD and operated diverticulitis in acute diverticulitis confirmed by CT using the modified Hinchey classification system.
MATERIALS AND METHODS
1. Data collection
We performed a search of the electronic medical and radiological records of patients admitted to Korea University Medical Center for acute colonic diverticulitis between January 1, 2005 and December 31, 2009. Patients were initially included if there was evidence of complicated diverticulitis as diagnosed by abdominal CT. Patients were excluded from analysis based on the following criteria: no evidence of diverticulitis on CT, diverticulitis diagnosis without CT, age under 18 years, final diagnosis with colon cancer, appendicitis, focal colitis with ischemia, or appendagitis diagnosed with the help of radiologists. A total of 412 patients were diagnosed with acute colonic diverticulitis over the study period. After exclusion criteria were applied, 128 patients with CT-confirmed acute colonic diverticulitis were identified and the cases were analyzed. Data including age, gender, body mass index (BMI), current smoking, comorbidity, leukocytosis, location of diverticulitis, number of diverticulum, recurrence of diverticulitis, grade of modified Hinchey classification, and surgical intervention were collected. Diverticulitis was defined as right-sided when it occurred at the cecum, ascending colon, hepatic flexure, or transverse colon. And diverticulitis was defined as left-sided when it was located between the splenic flexure and the rectum. Preexisting comorbidity was defined as cardiovascular, pulmonary, endocrinologic, neurologic, connective tissue diseases, and malignancy. Recurrence of diverticulitis was defined as abdominal pain, fever, and leukocytosis with consistent CT findings after treatment of primary diverticulitis.
All abdominal CT scans were interpreted retrospectively by two expert radiologists blinded to clinical information. The severity of diverticulitis was graded using the modified Hinchey classification. The modified Hinchey classification defines the following stages: stage Ia, pericolic inflammation (phlegmon); stage Ib, pericolic abscess; stage II, distant intraabdominal or retroperitoneal abscess; stage III, generalized peritonitis; and stage IV, fecal peritonitis. In case of disagreement with the initial interpretation about severity, the second interpretation was made with the help of another experienced radiologist. Degree of diverticulitis severity was finally made when thee radiologists reached a consensus interpretation.
2. Definition of severity
The degree of severity of acute colonic diverticulitis was defined as either moderate or severe, using the modified Hinchey classification. MD was defined as Hinchey stage Ia (pericolic inflammation), and SD was defined as Hinchey stage Ib or higher (abscess or peritonitis).
3. Statistical analysis
Analysis was performed using SPSS version 18 for Windows (IBM Co., Armonk, NY, USA). For univariate analysis, categorical variables were analyzed by the chi-squared test and continuous variables were analyzed by Student t-test. For multivariate analysis, logistic regression with forward selection (Wald) was used. The p-values <0.05 were considered significant.
RESULTS
1. Baseline patient characteristics
Patients' baseline characteristics are listed in Table 1. In 128 patients with complicated diverticulitis, the age range was 24 to 81 years (mean, 46.4±14.2 years). Forty-eight patients were older than 50 years (37.5%), and the average duration of follow-up was 5.1 years. Seventy-six patients were male (59.3%) and 52 patients were female (40.9%). Additionally, comorbidity, leukocytosis, and recurrent diverticulitis were present in 13.2%, 38.5%, and 13.2% of patients, respectively. Right-sided diverticulitis occurred in 84.3% of patients (n=108) and left-sided diverticulitis was found in 15.7% of patients (n=20). Among the 23 patients who underwent surgical intervention, six were operated on because of disease recurrence.
Table 1.
Baseline Characteristics of Patients with Computed Tomography-Confirmed Acute Diverticulitis
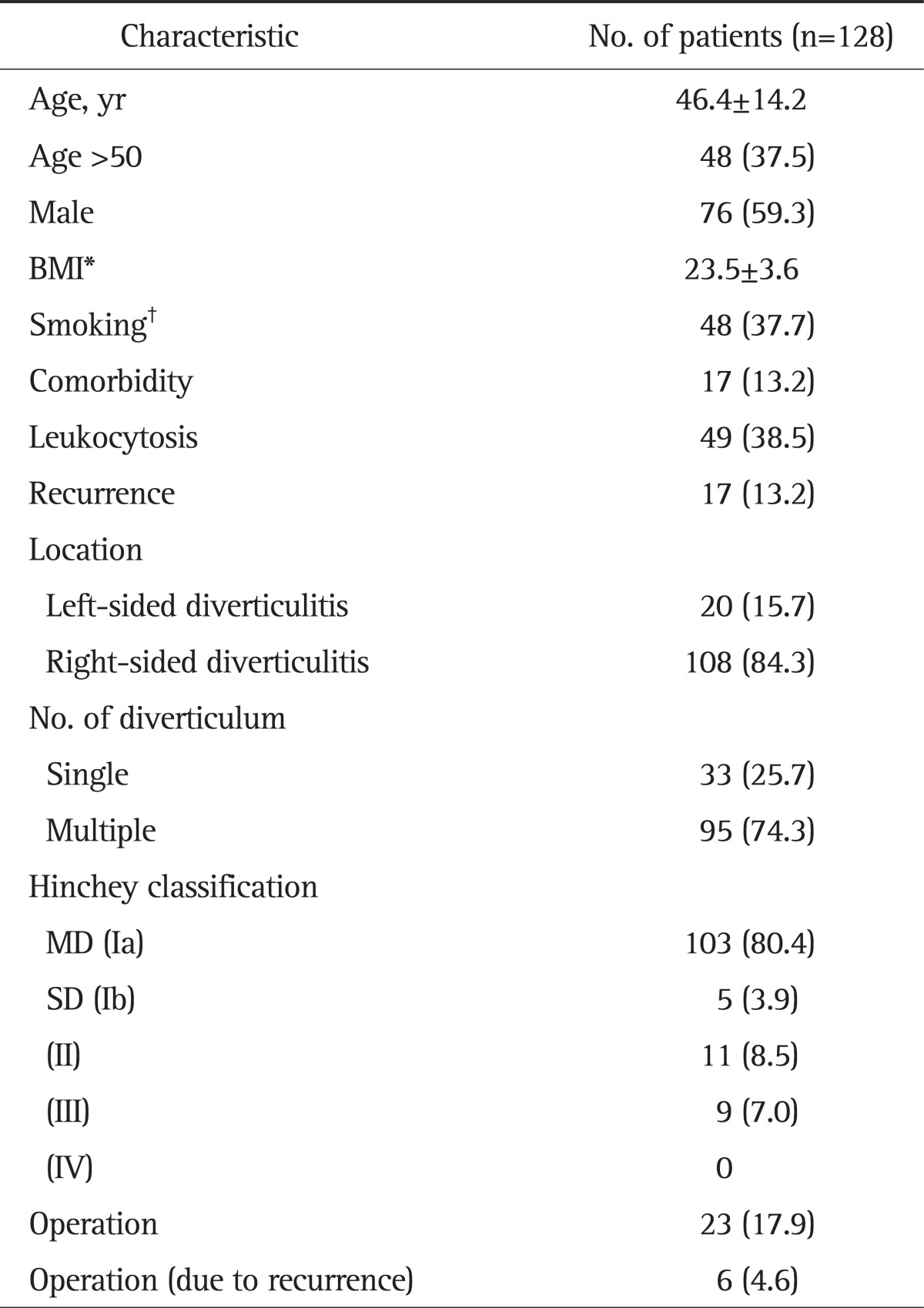
Data are presented as mean±SD or number (%).
BMI, body mass index; MD, moderate diverticulitis; SD, severe diverticulitis.
*Available number of patients, 124 (MD=100, SD=24); †Available number of patients, 127 (MD=102, SD=25).
2. Risk factors for SD
There were 103 patients with MD (80.5%) and 25 patients with SD (19.5%). In the SD group, five patients (3.9%) were diagnosed with stage Ib disease, 11 patients (8.5%) had stage II disease, and nine patients (7.0%) had stage III disease. The mean age was significantly higher in the SD group than in the MD group (56.6±18.0 vs 44.0±11.9, p=0.003) (Table 2). Patient gender, however, did not significantly differ between the two groups (p=0.6). The presence of comorbidity was found to be significantly associated with SD (32% vs 8.7%, p=0.005), and left-sided diverticulitis was also significantly more prevalent in the SD group (44% vs 8.7%, p<0.001). There was a statistically significant relationship between disease severity and both leukocytosis (60% vs 33%, p=0.014) and operation (48% vs 10.6%, p<0.001). However, BMI (p=0.72), smoking (p=0.475), recurrence (p=0.1), and the number of diverticulum (p=0.079) did not differ significantly between the two groups.
Table 2.
Risk Factors for Severe Diverticulitis in a Univariate Analysis
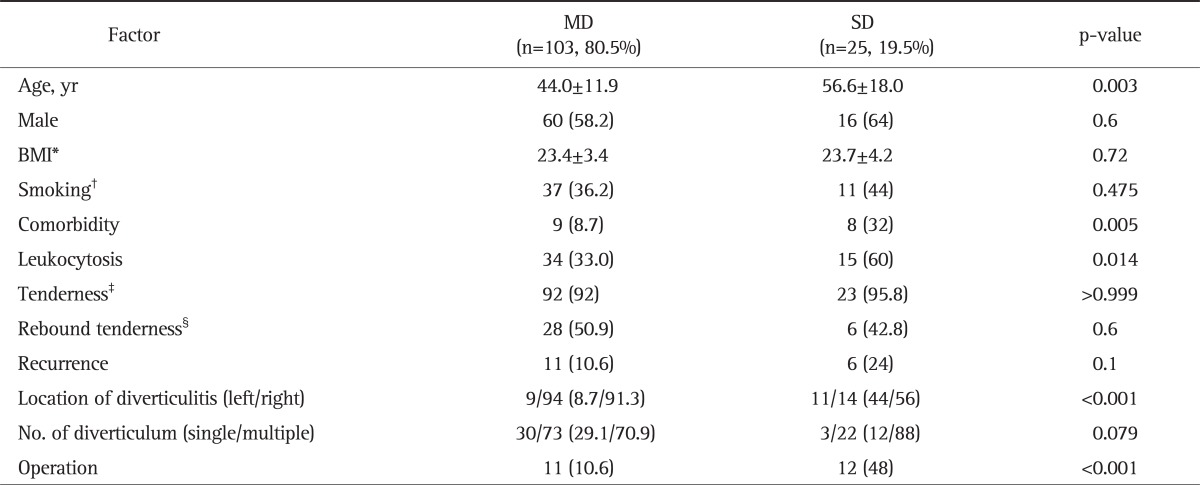
Data are presented as mean±SD or number (%).
MD, moderate diverticulitis; SD, severe diverticulitis; BMI, body mass index.
*Available number of patients, 124 (MD=100, SD=24); †Available number of patients, 127 (MD=102, SD=25); ‡Available number of patients, 124 (MD=100, SD=24); §Available number of patients, 69 (MD=55, SD=14).
The results of multivariate analysis between MD and SD are presented in Table 3. Age greater than 50 years was found to be a significant risk factor for SD (odds ratio [OR], 5.27; 95% confidence interval [CI], 1.347 to 20.682; p=0.017). Statistical significance was also noted in patients with a smoking history (OR, 3.61; 95% CI, 1.037 to 12.623; p=0.044), comorbidity (OR, 4.98; 95% CI, 1.034 to 24.053; p=0.045), leukocytosis (OR, 7.70; 95% CI, 1.980 to 29.946; p=0.003), recurrence (OR, 4.95; 95% CI, 1.144 to 21.448; p=0.032), and left-sided diverticulitis (OR, 6.92; 95% CI, 1.752 to 27.407; p=0.006). Gender, BMI, and the number of diverticulum did not demonstrate statistical significance in the multivariate analysis.
Table 3.
Risk Factors for Severe Diverticulitis in a Multivariate Analysis
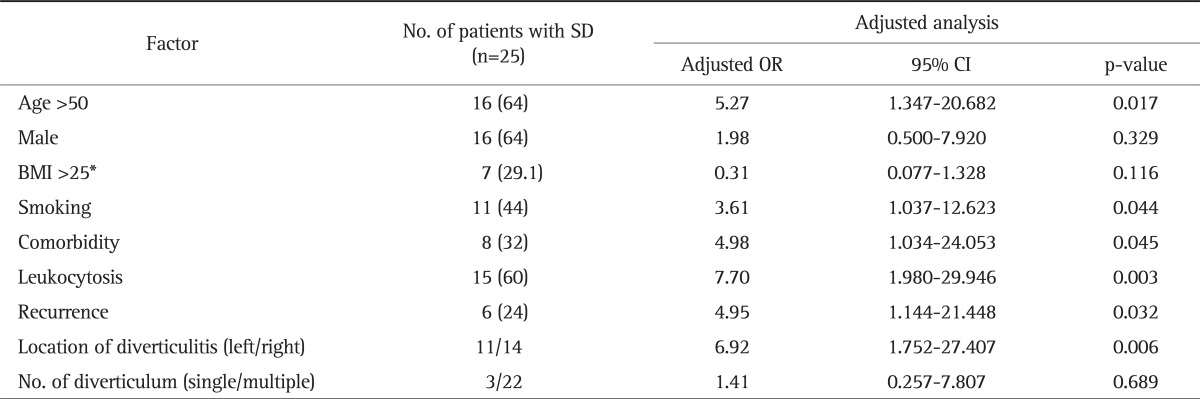
Data are presented as number (%).
SD, severe diverticulitis; OR, odds ratio; CI, confidence interval; BMI, body mass index.
*Available number of patients, 24.
3. Risk factors for operation
In addition to identifying the risk factors for SD in an episode of acute diverticulitis, we analyzed the risk factors associated with colectomy, which was performed emergently or after the failure of initial medical treatment (Table 4). Among 25 cases of SD, 23 patients underwent surgery except two subjects who refused it. Six patients were operated on due to recurrent attacks of diverticulitis even though the degree of diverticulitis was not severe. Therefore they were excluded in the analysis of the risk factors associated with colectomy. Of the 17 cases included in the analysis, eight patients were operated on emergently, and nine patients were not. Modified Hinchey classification >Ib (OR, 7.708; 95% CI, 2.209 to 26.894; p=0.001) and left-sided diverticulitis (OR, 5.140; 95% CI, 1.396 to 18.922; p=0.014) were found to be statistically significant risk factors for colectomy in episodes of acute diverticulitis.
Table 4.
Risk Factors for Operation in a Multivariate Analysis
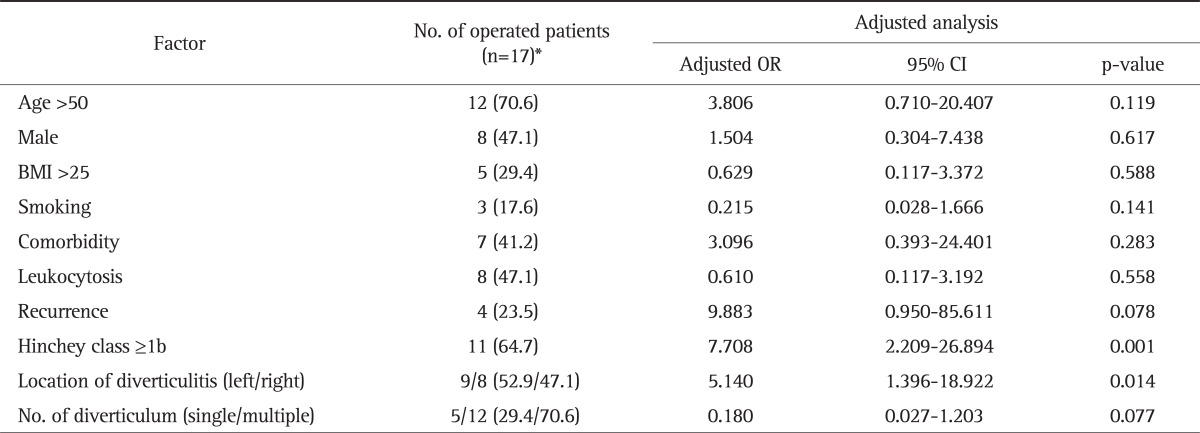
Data are presented as number (%).
OR, odds ratio; CI, confidence interval; BMI, body mass index.
*Excludes operations performed due to recurrence, n=6.
DISCUSSION
In the present study we retrospectively analyzed the risk factors for SD and operated diverticulitis in subjects who underwent abdominal CT scans, applying the modified Hinchey classification criteria. The factors related to SD were found to be age over 50 years, smoking, comorbidity, leukocytosis, recurrence, and left-sided diverticulitis. There is a considerable difference between these results and those in Western populations. In Western countries where diverticulitis is much more prevalent than in Asia and there are well-established guidelines and practice parameters for acute diverticulitis,9,10 risk factors for severe clinical manifestations were found to be younger age, smoking, obesity, nonsteroidal anti-inflammatory drugs or corticosteroid use, multiple comorbidities (including immunosuppression), and right-sided diverticulitis.11-20
The analysis of risk factors suggested that the association of location of diverticulitis with severity was different between Asian and Western populations. In Western countries where sigmoid colonic diverticulitis is more prevalent, right-sided diverticulitis is usually thought to run a more complicated course.13 On the contrary, the current study showed that left-sided diverticulitis was more severe than right-sided diverticulitis with an OR of 6.92 (95% CI, 1.752 to 27.407; p=0.006). This result is consistent with most other Asian studies, which showed that left-sided diverticulitis was considered a major risk factor for complicated diverticular disease and poor prognosis, though those studies did not analyze SD.21,22 One recent retrospective study that stratified the severity of diverticulitis with clinical categories determined that left-sided colonic diverticulitis was a risk factor for SD, with an odds ratio of 6.23.23 In another study, Komuta et al.24 reported the outcome of medical therapy for patients with acute right colonic diverticulitis. The authors concluded that medical management is effective because of the disease's benign course. Therefore, in contrast to Western countries, it is hypothesized that left-sided diverticulitis is closely associated with the development of SD in Asian countries.
The current study showed that smoking, comorbidity, and leukocytosis were also risk factors for SD, and this is largely in accordance with findings reported in the Western literature. However, while most Western studies have described diverticulitis in young patients as more aggressive and virulent with an increased risk of perforation and recurrence,11,25 old age (>50) was found to be a risk factor for SD in this study. This result supports the findings of other Asian researchers that diverticulitis in older patients is usually more complicated. Kim et al.21 reported that patients with right-sided diverticulitis in Korea were significantly younger and had lower complication rates. In another study conducted in Hong Kong, right-sided diverticulitis was associated with younger age, and correlated with low mortality and morbidity.22 Therefore, it is likely that diverticulitis in older patients has a more severe and virulent course in Asian countries, suggesting that there is a geographic difference in the impact of age on diverticulitis severity.
The present study also analyzed the relationship between diverticulitis severity and disease recurrence. While some reports suggest an increased risk of complications and a higher mortality rate in recurrent episodes,26-28 no link between recurrence and complicated diverticulitis was noted in newer studies.29-31 In this study, there were 17 patients (13.2%) with recurrent diverticulitis, and the OR for SD was 4.95. It is not certain whether this discrepancy originates from differences of inclusion criteria or diagnostic method, because the present study enrolled patients who undertook CT. Further large-scale studies using CT evidence of diverticulitis are required to identify the association between severity and recurrence of disease.
One important consideration in acute diverticulitis is the need for surgical management. Therefore, we intended to identify the risk factors for predicting operative intervention. There were 23 total patients (17.9%) who underwent colectomy, and of these, six patients (26%) underwent surgery because of disease recurrence. Recent reports, however, have consistently recommended against surgical intervention for repeated episodes of uncomplicated diverticulitis.32,33 Moreover, the new edition of the practice parameters of the American Society of Colon and Rectal Surgeons from 2006 no longer recommends elective surgery after two or more uncomplicated episodes of diverticulitis.9 Thus, we excluded the cases of recurrent diverticulitis in analyzing the risk factors for operation. Eleven patients out of the seventeen included in the analysis were Hinchey class Ib or higher, and this was found to be a significant risk factor for operation (OR, 7.708; 95% CI, 2.209 to 26.894; p=0.001). Furthermore, nine patients had left-sided diverticulitis and the OR for operation was 5.14, which was significant (95% CI, 1.396 to 18.922; p=0.014). To the best of our knowledge, we do not know any Asian study that reported an association between the location of diverticulitis and colectomy. There were only several studies to suggest a favorable course of right-sided diverticulitis,34-36 implying that left-sided diverticulitis necessitates operation more frequently than right diverticulitis. Our study not only demonstrated that left-sided diverticulitis progressed virulently, but also frequently necessitated surgical management. This finding is in contrast to Western reports indicating that right-sided diverticulitis requires surgical intervention more frequently.37,38 Therefore, we can only assume that left-sided diverticulitis is strongly associated with operated diverticulitis as well as SD in Asia.
Our current study only enrolled patients whose CT result was confirmed positive for diverticulitis. Numerous researchers have attempted to identify the risk factors for complicated diverticulitis and poor clinical outcomes, but the data were not consistent and there were contradictory conclusions. The inconsistency may be due to the relatively small sample sizes or the heterogeneity of the categories that were investigated as opposed to an examination of single, well-defined conditions.4 In addition, various diagnostic methods were employed (including CT, abdominal sonography, barium studies, colonoscopy, or operations) and other studies used clinical indexes such as abscess, perforation, recurrence, or systemic inflammatory response syndrome as a determination of severity. For these reasons, it is very difficult to make comprehensive comparisons between studies. Therefore, the fact that we enrolled only patients with diverticulitis that was confirmed by CT likely made this study more homogeneous and allowed for a more objective grading of the severity of diverticulitis compared to previous studies.
Another attribute of our study is that we subdivided complicated diverticulitis into moderate and severe. Ambrosetti39 suggested that complicated diverticulitis be stratified into moderate and severe based on CT imaging because of the differing prognoses; MD was defined as a localized colonic wall thickening greater than 5 mm with signs of inflammation in the pericolic fat, and SD was defined as colonic wall thickening with the presence of an abscess and/or extraluminal air and/or contrast leakage. In addition, Kaiser et al.3 demonstrated that the morbidity and mortality of patients with either Hinchey stage 0 or Ia disease were 4.4% and 0%, respectively, whereas patients with stage Ib or higher had significantly more complications (32.3%) and fatal outcomes (2.3%). Therefore, we subdivided complicated diverticulitis into two categories: MD was defined as stage Ia, while SD was defined as stage Ib or higher.
The clinical implications of this study require further investigation because of several drawbacks. This single tertiary center study is not representative of the entire Korean population. Additionally, since not all patients with episodes of acute diverticulitis underwent an abdominal CT scan, selection bias could affect the results.
In summary, there are considerable literatures detailing the risk factors related to complicated diverticulitis and poor clinical outcomes, but the data are not consistent because of the diversity in clinical categories of disease and the methods used for diagnosis. This study was performed only using patients whose CT imaging confirmed acute diverticulitis in order to achieve objectivity and homogeneity.
Conclusively, old age, smoking, comorbidity, leukocytosis, recurrent episode of diverticulitis, and left-sided disease were all associated with SD. Left-sided diverticulitis was also found to be an important risk factor in undergoing surgical treatment for an acute episode of diverticulitis. These clinical parameters should be taken into consideration for the management of acute colonic diverticulitis, being aware that there are considerable differences between Asian and Western populations. Moreover, given that the morbidity and mortality are quite different between moderate and severe stages of diverticulitis, we suggest that it is necessary to subdivide complicated diverticulitis into MD and SD, based on CT findings.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Bogardus ST., Jr What do we know about diverticular disease? A brief overview. J Clin Gastroenterol. 2006;40(Suppl 3):S108–S111. doi: 10.1097/01.mcg.0000212603.28595.5c. [DOI] [PubMed] [Google Scholar]
- 2.Siewert JR, Huber FT, Brune IB. Early elective surgery of acute diverticulitis of the colon. Chirurg. 1995;66:1182–1189. [PubMed] [Google Scholar]
- 3.Kaiser AM, Jiang JK, Lake JP, et al. The management of complicated diverticulitis and the role of computed tomography. Am J Gastroenterol. 2005;100:910–917. doi: 10.1111/j.1572-0241.2005.41154.x. [DOI] [PubMed] [Google Scholar]
- 4.Morris CR, Harvey IM, Stebbings WS, Speakman CT, Kennedy HJ, Hart AR. Epidemiology of perforated colonic diverticular disease. Postgrad Med J. 2002;78:654–658. doi: 10.1136/pmj.78.925.654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cho KC, Morehouse HT, Alterman DD, Thornhill BA. Sigmoid diverticulitis: diagnostic role of CT: comparison with barium enema studies. Radiology. 1990;176:111–115. doi: 10.1148/radiology.176.1.2191360. [DOI] [PubMed] [Google Scholar]
- 6.Ambrosetti P, Grossholz M, Becker C, Terrier F, Morel P. Computed tomography in acute left colonic diverticulitis. Br J Surg. 1997;84:532–534. doi: 10.1046/j.1365-2168.1997.02576.x. [DOI] [PubMed] [Google Scholar]
- 7.Lohrmann C, Ghanem N, Pache G, Makowiec F, Kotter E, Langer M. CT in acute perforated sigmoid diverticulitis. Eur J Radiol. 2005;56:78–83. doi: 10.1016/j.ejrad.2005.03.003. [DOI] [PubMed] [Google Scholar]
- 8.Jacobs DO. Clinical practice. Diverticulitis. N Engl J Med. 2007;357:2057–2066. doi: 10.1056/NEJMcp073228. [DOI] [PubMed] [Google Scholar]
- 9.Rafferty J, Shellito P, Hyman NH, Buie WD Standards Committee of American Society of Colon and Rectal Surgeons. Practice parameters for sigmoid diverticulitis. Dis Colon Rectum. 2006;49:939–944. doi: 10.1007/s10350-006-0578-2. [DOI] [PubMed] [Google Scholar]
- 10.de Wit NJ, Berger MY, Vogelenzang R, et al. Summary of the Dutch College of General Practitioners (NHG) practice guideline on 'Diverticulitis'. Ned Tijdschr Geneeskd. 2012;156:A4140. [PubMed] [Google Scholar]
- 11.Ambrosetti P, Gervaz P, Fossung-Wiblishauser A. Sigmoid diverticulitis in 2011: many questions, few answers. Colorectal Dis. 2012;14:e439–e446. doi: 10.1111/j.1463-1318.2012.03026.x. [DOI] [PubMed] [Google Scholar]
- 12.Spivak H, Weinrauch S, Harvey JC, Surick B, Ferstenberg H, Friedman I. Acute colonic diverticulitis in the young. Dis Colon Rectum. 1997;40:570–574. doi: 10.1007/BF02055381. [DOI] [PubMed] [Google Scholar]
- 13.Reisman Y, Ziv Y, Kravrovitc D, Negri M, Wolloch Y, Halevy A. Diverticulitis: the effect of age and location on the course of disease. Int J Colorectal Dis. 1999;14:250–254. doi: 10.1007/s003840050219. [DOI] [PubMed] [Google Scholar]
- 14.Dobbins C, Defontgalland D, Duthie G, Wattchow DA. The relationship of obesity to the complications of diverticular disease. Colorectal Dis. 2006;8:37–40. doi: 10.1111/j.1463-1318.2005.00847.x. [DOI] [PubMed] [Google Scholar]
- 15.Turunen P, Wikström H, Carpelan-Holmström M, Kairaluoma P, Kruuna O, Scheinin T. Smoking increases the incidence of complicated diverticular disease of the sigmoid colon. Scand J Surg. 2010;99:14–17. doi: 10.1177/145749691009900104. [DOI] [PubMed] [Google Scholar]
- 16.Klarenbeek BR, Samuels M, van der Wal MA, van der Peet DL, Meijerink WJ, Cuesta MA. Indications for elective sigmoid resection in diverticular disease. Ann Surg. 2010;251:670–674. doi: 10.1097/SLA.0b013e3181d3447d. [DOI] [PubMed] [Google Scholar]
- 17.Schwartz HA. Lower gastrointestinal side effects of nonsteroidal antiinflammatory drugs. J Rheumatol. 1981;8:952–954. [PubMed] [Google Scholar]
- 18.Campbell K, Steele RJ. Non-steroidal anti-inflammatory drugs and complicated diverticular disease: a case-control study. Br J Surg. 1991;78:190–191. doi: 10.1002/bjs.1800780218. [DOI] [PubMed] [Google Scholar]
- 19.Canter JW, Shorb PE., Jr Acute perforation of colonic diverticula associated with prolonged adrenocorticosteroid therapy. Am J Surg. 1971;121:46–51. doi: 10.1016/0002-9610(71)90076-6. [DOI] [PubMed] [Google Scholar]
- 20.Yoo PS, Garg R, Salamone LF, Floch MH, Rosenthal R, Longo WE. Medical comorbidities predict the need for colectomy for complicated and recurrent diverticulitis. Am J Surg. 2008;196:710–714. doi: 10.1016/j.amjsurg.2008.07.017. [DOI] [PubMed] [Google Scholar]
- 21.Kim JH, Cheon JH, Park S, et al. Relationship between disease location and age, obesity, and complications in Korean patients with acute diverticulitis: a comparison of clinical patterns with those of Western populations. Hepatogastroenterology. 2008;55:983–986. [PubMed] [Google Scholar]
- 22.Law WL, Lo CY, Chu KW. Emergency surgery for colonic diverticulitis: differences between right-sided and left-sided lesions. Int J Colorectal Dis. 2001;16:280–284. doi: 10.1007/s003840100339. [DOI] [PubMed] [Google Scholar]
- 23.Kim SY, Oh TH, Seo JY, et al. The clinical factors for predicting severe diverticulitis in Korea: a comparison with Western countries. Gut Liver. 2012;6:78–85. doi: 10.5009/gnl.2012.6.1.78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Komuta K, Yamanaka S, Okada K, et al. Toward therapeutic guidelines for patients with acute right colonic diverticulitis. Am J Surg. 2004;187:233–237. doi: 10.1016/j.amjsurg.2003.11.009. [DOI] [PubMed] [Google Scholar]
- 25.Pautrat K, Bretagnol F, Huten N, de Calan L. Acute diverticulitis in very young patients: a frequent surgical management. Dis Colon Rectum. 2007;50:472–477. doi: 10.1007/s10350-006-0787-8. [DOI] [PubMed] [Google Scholar]
- 26.Hackford AW, Schoetz DJ, Jr, Coller JA, Veidenheimer MC. Surgical management of complicated diverticulitis. The Lahey Clinic experience, 1967 to 1982. Dis Colon Rectum. 1985;28:317–321. doi: 10.1007/BF02560431. [DOI] [PubMed] [Google Scholar]
- 27.Parks TG. Natural history of diverticular disease of the colon. A review of 521 cases. Br Med J. 1969;4:639–642. doi: 10.1136/bmj.4.5684.639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Colcock BP. Surgical management of complicated diverticulitis. N Engl J Med. 1958;259:570–573. doi: 10.1056/NEJM195809182591204. [DOI] [PubMed] [Google Scholar]
- 29.Chapman JR, Dozois EJ, Wolff BG, Gullerud RE, Larson DR. Diverticulitis: a progressive disease? Do multiple recurrences predict less favorable outcomes? Ann Surg. 2006;243:876–830. doi: 10.1097/01.sla.0000219682.98158.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Comparato G, Di Mario F NDSG. Recurrent diverticulitis. J Clin Gastroenterol. 2008;42:1130–1134. doi: 10.1097/MCG.0b013e3181886ee4. [DOI] [PubMed] [Google Scholar]
- 31.Chautems RC, Ambrosetti P, Ludwig A, Mermillod B, Morel P, Soravia C. Long-term follow-up after first acute episode of sigmoid diverticulitis: is surgery mandatory? A prospective study of 118 patients. Dis Colon Rectum. 2002;45:962–966. doi: 10.1007/s10350-004-6336-4. [DOI] [PubMed] [Google Scholar]
- 32.Salem L, Veenstra DL, Sullivan SD, Flum DR. The timing of elective colectomy in diverticulitis: a decision analysis. J Am Coll Surg. 2004;199:904–912. doi: 10.1016/j.jamcollsurg.2004.07.029. [DOI] [PubMed] [Google Scholar]
- 33.Janes S, Meagher A, Frizelle FA. Elective surgery after acute diverticulitis. Br J Surg. 2005;92:133–142. doi: 10.1002/bjs.4873. [DOI] [PubMed] [Google Scholar]
- 34.Kim MR, Kye BH, Kim HJ, Cho HM, Oh ST, Kim JG. Treatment of right colonic diverticulitis: the role of nonoperative treatment. J Korean Soc Coloproctol. 2010;26:402–406. doi: 10.3393/jksc.2010.26.6.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Park SJ, Choi SI, Lee SH, Lee KY. Image-guided conservative management of right colonic diverticulitis. World J Gastroenterol. 2009;15:5838–5842. doi: 10.3748/wjg.15.5838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Matsushima K. Management of right-sided diverticulitis: a retrospective review from a hospital in Japan. Surg Today. 2010;40:321–325. doi: 10.1007/s00595-008-4055-5. [DOI] [PubMed] [Google Scholar]
- 37.Lane JS, Sarkar R, Schmit PJ, Chandler CF, Thompson JE., Jr Surgical approach to cecal diverticulitis. J Am Coll Surg. 1999;188:629–634. doi: 10.1016/s1072-7515(99)00043-5. [DOI] [PubMed] [Google Scholar]
- 38.Fang JF, Chen RJ, Lin BC, Hsu YB, Kao JL, Chen MF. Aggressive resection is indicated for cecal diverticulitis. Am J Surg. 2003;185:135–140. doi: 10.1016/s0002-9610(02)01209-6. [DOI] [PubMed] [Google Scholar]
- 39.Ambrosetti P. Acute diverticulitis of the left colon: value of the initial CT and timing of elective colectomy. J Gastrointest Surg. 2008;12:1318–1320. doi: 10.1007/s11605-008-0489-8. [DOI] [PubMed] [Google Scholar]