

Abstract
This is a case report of suicidal ingestion of chlorfenapyr, presenting with neurological complications after a latent period of more than a week, and rapidly progressing to death within days of symptoms. Chlorfenapyr is a moderately hazardous pesticide according to World Health Organization toxicity classification, and kills target organism by depriving it of energy through interference with oxidative phosphorylation at mitochondrial level. A pro-pesticide, chlorfenapyr takes time to convert to its active form and either this active form or a toxic metabolite causes delayed neurological symptoms. It causes significant neurotoxicity in rat models. This case report provides for the first time from India (second worldwide), clinical and “radiological evidence” (magnetic resonance imaging showing demyelinating/oedematous changes) of “chlorfenapyr neurotoxicity in humans.” It also highlights the “latent period” between ingestion and onset of fatal manifestations. Earlier, similar case reports of human deaths with delayed onset neurological symptoms, due to chlorfenapyr poisoning have been reported, from Japan, Columbia, and Korea.
Keywords: Chlorfenapyr, pesticides, poisoning, suicides
Introduction
According to World Health Organization (WHO), suicide deaths globally are approximately 9,00,000 annually and deaths due to pesticide poisoning are alarmingly high at 3,00,000/year.[1] Chlorfenapyr, a novel insecticide, causes neurotoxicity in experimental animals. There are similar case reports of delayed onset neurological symptoms culminating in death due to chlorfenapyr poisoning from Japan, Columbia, and Korea.[2–4] Although, abstracts are unavailable, case reports by Choi et al. and Endo et al. have been mentioned in clinical toxicology and Chudoku Kenkyu respectively. This report provides for the first time from India (second worldwide), “radiological evidence” of chlorfenapyr neurotoxicity in humans, besides highlighting the “latent period” in clinical course.
Case Report
A 28-year-old female, housewife from Tenali in Guntur district of Andhra Pradesh, was brought to the hospital, Guntur, with chief complaints of low backache, weakness of lower limbs, and drowsiness for 2 days. Ten days prior to presentation, she consumed pesticide chlorfenapyr with suicidal intent and she was apparently normal prior to the incident. At her hometown, gastric lavage and supportive treatment were given before discharge, 2 days later. Three days post-discharge, she was treated symptomatically for headache and neck pain, which reportedly were relieved. For 7 days following discharge she was apparently normal and had no history of fever/vomiting/diarrhea/abdominal pain/cough/breathing difficulty/chest pain/palpitations/cranial nerve/motor/sensory/cerebellar dysfunction. However, she presented to the Guntur hospital, 7 days later, with rapidly progressing weakness and pain in lower limbs, low back pain, swaying, increasing drowsiness, since 2 days. On admission, she was treated with Inj. Neurobion one ampoule IM, Inj. Pantoprazole 40 mg IV, Inj. ceftriaxone 1 gm IV, Inj. Methylprednisolone 1 g IV stat and IV fluids - RL, DNS,5%D. Except for the poisoning history, initial clinical presentation looked similar to acute disseminated encephalomyelitis, requiring the steroid. Symptoms progressed rapidly over the next 24 h. Lower limbs weakness progressed to involve the upper limbs and complete paralysis ensued. Motor examination showed complete loss of power, hypotonia, bilateral plantar extensor, and lost superficial and deep tendon reflexes in all limbs. Sensory examination showed complete loss of all sensations. Her sensorium rapidly deteriorated to coma. She developed high grade fever on 2nd day and eventually died within 24 h of admission and 10 days after consuming chlorfenapyr.
Hemoglobin was 8.4 gm %, Total count was 8400 and ESR was 20 mm at 1 hour. Serun biochemistry was normal. S Cholinestrase was 10370u/ml. MRI showed white matter changes in the brainstem and white matter in the brain and spinal cord [Figures 1–3].
Figure 1.
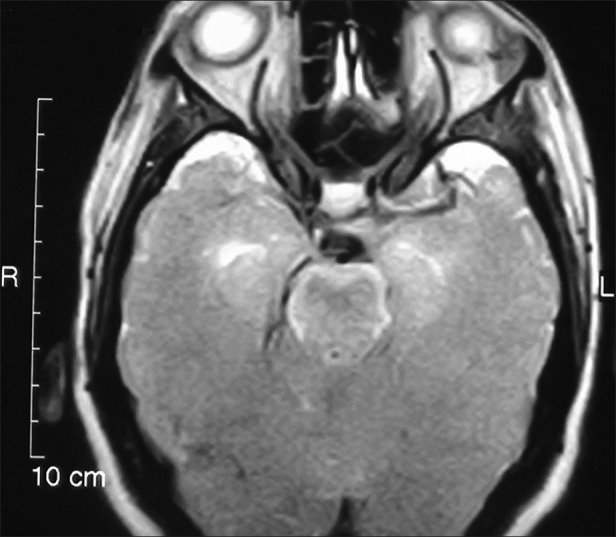
T2W axial image of brain showing demyelination of pons and predominantly medial temporal lobe
Figure 3.

T2W mid sagittal image of spinal cord showing diffuse edema and demyelination
Figure 2.
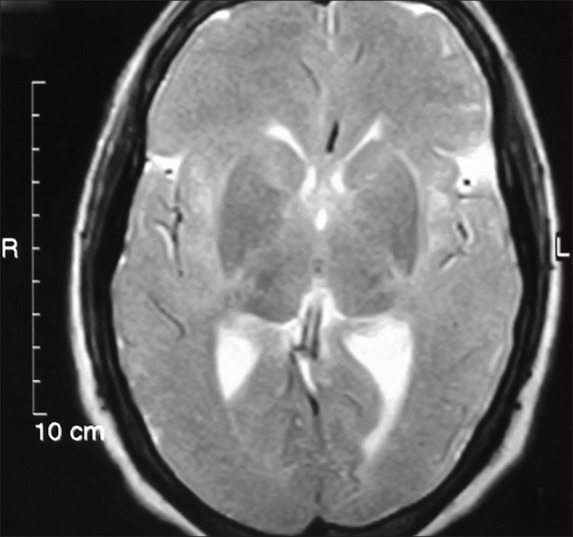
T2W axial image of brain showing demyelination of internal capsule, external capsule and insular cortex
Discussion
Chlorphenapyr, is a novel - insecticide, belonging to pyrrole group. WHO has accorded it CAS No. 122453-73-0 and classified it as class 2-moderately hazardous chemical.[5] Compounds with LD50(mean lethal dose) for rats with oral exposure of 50-2000 ng/kg or dermal exposure of 200-2,000 ng/kg are classified as moderately hazardous.[5] Chlorphenapyr is 4-Bromo-2-(4-chlorophenyl)-1-(ethoxymethyl)-5-(triflouromethyl) pyrrole-3-carboritrile. Its empirical formula is C15H11BrClF3N2O. It has no antidote.[6]
A non-repellant, Chlorphenapyr is used for protection of plants and vegetables[6] and it is a pro-insecticide and oxidative removal of the N-ethoxy methyl group of chlorphenapyr by mixed function oxidases leads to it’s active, toxic form identified as 303268 or a toxic metabolite, which uncouples oxidative phosphorylation in the mitochondria, resulting in disruption of adenosine tri-phosphate production and loss of energy leading to cell dysfunction and subsequent death of the organism.[6]
Interestingly, neurohistopathological examination of rats during the 1 year dietary neurotoxicity study (MRID 43492833) of chlorphenapyr revealed myelin sheath swelling in the spinal n roots compared to controls at 13 weeks.[7] Acute neurotoxicity studies in rats (MRID 43492829) showed gait disturbances, locomotion problems, arousal, and lethargy.[7] Findings in animal studies are similar to the radiological findings observed in this case. Thus, this case report confirms, “chlorfenapyr neurotoxicity in humans” and provides radiological evidence of the same. The first evidence from India of “Spinal cord changes” in addition to magnetic resonance imaging brain changes due to chlorfenapyr are presented here.
This case report also alerts physicians to “a latent period,” which gives a false sense of security to the doctor, between the initial period of ingestion when symptomatic management is given and appearance later of sudden, rapidly deteriorating fatal manifestations. The clinical course is biphasic-non-specific symptoms initially followed by fatal, neurotoxic symptoms by 7th day. In the previous case reports, as in this case, neurological complications occurred suddenly on or after 7th day and death within 24 h.
An estimated 187,000 suicides per year from India are due to deliberate pesticide poisoning, concentrated in four southern states, including Andhra Pradesh, from where this case report comes.[8] In view of the scale of human losses due to poisoning, this case report re-emphasizes, the need for intensifying the currently low-level of search for antidotes. Piperanoyl butoxinide, inhibitior of cyp450 enzymes in target organisms is a synergist to many pesticides but studies in insects, and effect on mosquitoes in treated malaria bed nets have demonstrated antagonism with chlorfenapyr.[9,10] It interferes with conversion of chlorfenapyr pro-insecticide to toxic form 303268 or a toxic metabolite and it offers a ray of hope as an antidote but it’s toxicity profile in humans needs more extensive study before recommending it.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Bertolote JM, Fleischmann A, Butchart A, Besbelli N. Suicide, suicide attempts and pesticides: A major hidden public health problem. [last accessed on 11/17/2012];Bull World Health Organ. 2006 84:260. doi: 10.2471/blt.06.030668. Available from: http://www.who.int./bulletin/volumes/84/4/editorial30406 html/en/index.html . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hoshiko M, Naito S, Koga M, Mori M, Hara K, Ishitake T. Case report of acute death on the 7 th day due to exposure to the vapor of the insecticide chlorfenapyr. Chudoku Kenkyu. 2007;20:131–6. [PubMed] [Google Scholar]
- 3.Maria S, Suarez J. Use of pesticides as a suicide method: A case report with chlorfenapyr. Rev Colomb Psiquiatr. 2008;37:272–9. [Google Scholar]
- 4.Kwon JS, Kim HY, Han HJ, Han JY, Kim JY, Park JH. A case of chlorfenapyr intoxication with central nervous system involvement. J Clin Toxicol. 2012;2:147. [Google Scholar]
- 5.The WHO Recommended classification of pesticides by hazard and guidelines to classification. IPCS. 2009. [Last accessed on 10/03/2012]. Available from: http://www.who.int/ipcs/publications/pesticides_hazard_rev_3.pdf .
- 6.Kegley SE, Hill BR, Orme S, Choi AH. Chlorfenapyr-toxicity, ecological toxicity and regulating interactions. PAN PesticideDatabase, Pesticide Action Network, North America. 2010. [Last accessed on 10/03/2012]. Available from: http://www.pesticideinfo.org/Detail_Chemical.jsp?Rec_id=PC35810 .
- 7.Chlorfenapyr 129093: Health Effect Division Risk Characterization. 1998. [Last accessed on 10/03/2012]. Available from: http://www.epa.gov/opprd001/chlorfenapyr/memohed2.pdf .
- 8.Patel V, Ramasundarahettige C, Vijayakumar L, Thakur JS, Gajalakshmi V, Gururaj G, et al. Suicide mortality in India: A nationally representative survey. Lancet. 2012;379:2343–51. doi: 10.1016/S0140-6736(12)60606-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Black BC, Hollingworth RM, Ahammadsahib KI, Kukel CD, Donovan S. Insecticidal action and mitochondrial uncoupling activity of ac-303,630 and related halogenated pyrroles. [Last accessed on 11/26/2012];Pestic Biochem Physiol. 1994 50:115–28. Available from: http://dx.doi.org/10.1006/pest. 1994.1064. [Google Scholar]
- 10.Raghavendra K, Barik TK, Sharma P, Bhatt RM, Srivastava HC, Sreehari U, et al. Chlorfenapyr: A new insecticide with novel mode of action can control pyrethroid resistant malaria vectors. Malar J. 2011;10:16. doi: 10.1186/1475-2875-10-16. [DOI] [PMC free article] [PubMed] [Google Scholar]