

Abstract
Primary sarcoma of breast are rare. Diagnosis by aspiration cytology is difficult due to nonspecific cytomorphologic features. An initial presentation with neurological symptoms due to metastasis of breast sarcoma to the brain has not been previously reported. Here, we describe a case of a 60-year-old female who presented with headache, dizziness and convulsion and was subsequently diagnosed with undifferentiated high grade pleomorphic sarcoma of breast with cerebellar metastasis.
Keywords: Aspiration cytology, breast sarcoma, cerebellar metastasis, pleomorphic malignant fibrous histiocytoma, undifferentiated high grade pleomorphic sarcoma
Introduction
Primary breast sarcoma are rare tumors accounting for less than 1% of breast malignancies.[1] Cytological diagnosis of primary breast sarcoma is extremely challenging as the differential diagnosis includes a variety of spindle cell lesions such as cystosarcoma phyllodes, sarcomatoid/metaplastic carcinomas and melanomas. The diagnosis of pleomorphic sarcoma is a diagnosis of exclusion. Brain metastasis as an initial presentation of breast sarcoma has not been reported. Here, we describe the case of a 60-year-old female patient who presented with the symptoms of headache and a single episode of seizure with a subsequent diagnosis of primary breast undifferentiated high grade pleomorphic sarcoma with cerebellar metastasis.
Case Report
A 60-year-old postmenopausal woman presented to the outpatient department with symptoms of headache and occasional dizziness for the last 2 months with one episode of generalized tonic clonic seizure 2 days back. The patient was of poor health status with mild pallor. The patient, on enquiry, also complained about a lump in her left breast for the last six months. There was no history of nipple discharge. On examination, a firm 6 × 4 cm swelling was palpated in the upper outer quadrant of the left breast. The swelling was non-tender and mobile with fixity to the overlying skin but not with the chest wall. There was no axillary lymphadenopathy; and the other breast was found normal on clinical examination. Clinical examination and history did not reveal any other abnormality. The patient underwent laboratory and imaging studies with fine needle aspiration of the breast lump. CT scan showed a heterogeneously enhancing hypodense infratentorial lesion measuring 6.3 × 5.7 cm in left cerebellar hemisphere and vermis compressing and displacing the fourth ventricle [Figure 1]. Laboratory tests showed hemoglobin of 9.8 gm/dl with microcytic, hypochromic anemia. The chest X-ray was normal. During FNAC, two passes were made. The smears were stained with Papanicolaou and May-Grunwald-Giemsa (MGG) stain and showed a dispersed population of malignant pleomorphic, sometimes bizarre, spindle cells and few multinucleated tumor giant cells. There was no epithelial component in the prepared smears. The background was hemorrhagic [Figure 2]. A cytologic diagnosis of malignant sarcomatoid spindle cell tumor was made. The differential diagnoses suggested were undifferentiated high grade pleomorphic sarcoma, malignant phyllodes tumor and metaplastic carcinoma (spindle/sarcomatoid variant). The patient underwent wide excision of the tumor. No axillary dissection was done. The histopathologic examination showed a high grade sarcoma composed of pleomorphic spindle cells arranged in fascicles and vague storiform pattern. There were bizarre and multinucleated tumor giant cells. The mitotic count was 15/10 HPF with atypical forms. There were foci of dystrophic calcification [Figure 3]. Immunohistochemistry for Cytokeratin (CK), Epithelial Membrane Antigen (EMA), Smooth Muscle Actin (SMA), desmin and S-100 protein were performed with adequate controls and showed no immunoreactivity indicating a lack of differentiation. A stereotactic biopsy from the cerebellar lesion showed similar histological and immunohistochemical pattern. A diagnosis of primary high grade undifferentiated pleomorphic sarcoma of breast with cerebellar metastasis was made. The patient in the post-operative period deteriorated quickly and developed progressive ataxia and headache. The patient died 3 weeks later.
Figure 1.
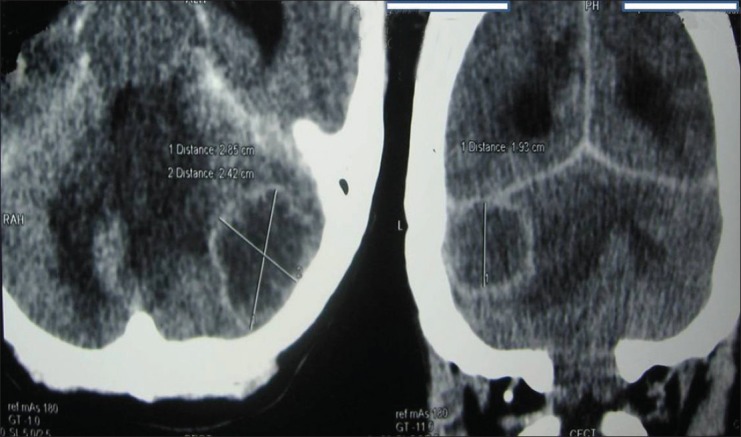
CT scan showing a heterogeneously enhancing hypodense infratentorial lesion in left cerebellar hemisphere and vermis compressing and displacing the fourth ventricle
Figure 2.
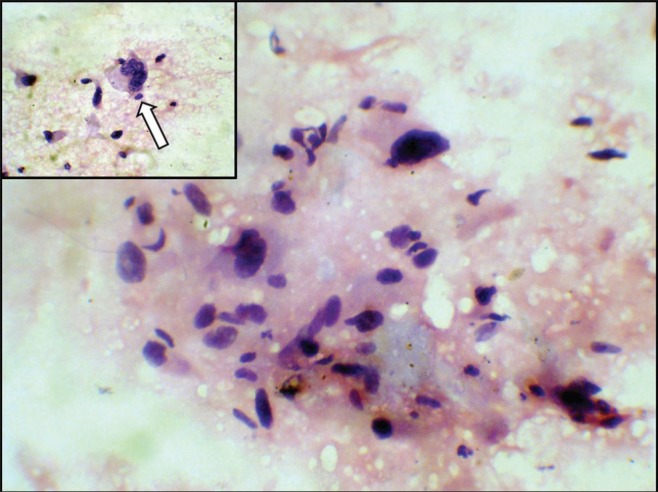
Microphotograph showing dispersed population and loose aggregates of pleomorphic spindle cells with bizarre cells. Inset shows a multinucleated giant cell (white arrow). (Papanicolaou stain; ×400 magnification)
Figure 3.
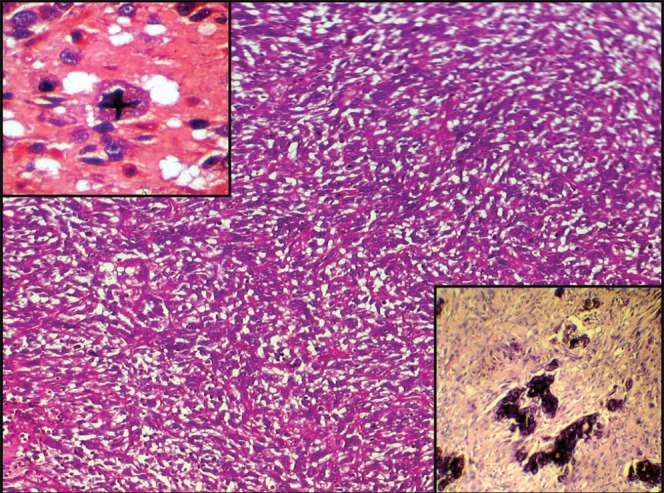
Microphotograph showing histopathology of undifferentiated pleomorphic sarcoma of breast with inset in lower right showing foci of dystrophic calcification (H and E, ×100 magnification) Inset in upper left shows atypical mitotic figure (H and E, ×400 magnification)
Discussion
Malignant fibrous histiocytoma (MFH) is now regarded as a morphological pattern rather than a distinct clinicopathological entity. The terms pleomorphic MFH and undifferentiated high grade pleomorphic sarcoma are used interchangeably to represent a group of pleomorphic, high-grade sarcomas showing no line of differentiation[1,2] although focal smooth muscle actin immunoreactivity can be seen.
Primary breast sarcomas are rare neoplasms with a reported incidence of less than 1% of breast malignancies[1] and they have rarely been reported by aspiration cytology. Chhieng et al.,[3] in a series of 5306 breast FNACs showed a specificity of 82.6% in diagnosing spindle cell lesions of breast. In a cytological study of 2064 breast FNA biopsies, Silverman et al., found that sarcoma accounted for 2.6% of all malignant breast tumors.[4] Stanley et al.,[5] described cytological diagnosis of two cases of stromal sarcoma and two cases of angiosarcomas of the breast.
Diagnosing primary sarcoma of breast in cytology aspirates is difficult not only because of its rarity but also since a variety of malignant neoplasms including malignant phyllodes tumor, metaplastic carcinoma, pleomorphic breast carcinoma and even melanomas can have overlapping cytomorphologic features. Malignant phyllodes tumor, for example, shows presence of malignant spindle cells with pleomorphism and increased mitoses but presence of benign epithelial cell clusters usually favors the diagnosis. Occasionally, undifferentiated high grade pleomorphic sarcoma can present with benign ductal epithelium, not to be misinterpreted as a biphasic tumor. Phyllodes can be similar to fibroadenoma on low power cytology but usually have increased stromal atypia. Also inadequate sampling causes diagnostic difficulties. Metaplastic carcinoma, chiefly spindle cell carcinoma and carcinosarcoma can be difficult to differentiate on cytology from primary sarcoma. Immunohistochemistry for epithelial markers on cell block material can be helpful. Still, few cases become very difficult to interpret. Sharma et al.,[6] reported a case of MFH of chest wall which on FNAC was reported as medullary carcinoma of breast in two separate institutions.
Malignant fibrous histiocytoma/undifferentiated high grade pleomorphic sarcoma are rare high grade sarcoma and constitute less than 5% of all sarcomain adults[7] and have been rarely seen in breast.[8] In the largest series till date, Hartel et al.[9] presented 19 cases of primary breast malignant fibrous histiocytoma (MFH) or myxofibrosarcoma/pleomorphic sarcoma not otherwise specified. They confirmed the presence of MFH in breast and discussed various histomorphological and immunohistochemical patterns.
Brain metastasis is an important cause of mortality and morbidity in cancer patients and outnumbers primary brain tumors in adults. The common primary sites include lung, breast, skin etc., but to our knowledge, cerebellar metastasis from breast sarcoma has not been previously reported. As sarcoma usually spread by hematogenous route, in our case we did not find any evidence of lymph node metastasis.
Hence, we present the first case of primary undifferentiated high grade pleomorphic sarcoma of breast with cerebellar metastasis which presented primarily with neurological symptoms.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Jeong YJ, Oh HK, Bong JG. Undifferentiated pleomorphic sarcoma of the male breast causing diagnostic challenges. J Breast Cancer. 2011;14:241–6. doi: 10.4048/jbc.2011.14.3.241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fletcher CD, Unni KK, Mertens F. World Health Organization Classification of Tumors: Pathology and Genetics of Tumors of Soft Tissue and Bone.Lyon: IARC Press; 2002. p. World Health Organization Classification of Tumors: Pathology and Genetics of Tumors of Soft Tissue and Bone Lyon: IARC Press; 2002 p 9-154. [Google Scholar]
- 3.Chhieng DC, Cangiarella JF, Waisman J, Fernandez G, Cohen JM. Fine-needle aspiration cytology of spindle cell lesions of the breast. Cancer. 1999;87:359–71. doi: 10.1002/(sici)1097-0142(19991225)87:6<359::aid-cncr7>3.0.co;2-7. [DOI] [PubMed] [Google Scholar]
- 4.Silverman JF, Geisinger KR, Frable WJ. Fine-needle aspiration cytology of mesenchymal tumors of the breast. Diagn Cytopathol. 1988;4:50–8. doi: 10.1002/dc.2840040113. [DOI] [PubMed] [Google Scholar]
- 5.Stanley MW, Tani EM, Horwitz CA, Tulman S, Skoog L. Primary spindle-cell sarcomas of the breast: Diagnosis by fine-needle aspiration. Diagn Cytopathol. 1988;4:244–9. doi: 10.1002/dc.2840040313. [DOI] [PubMed] [Google Scholar]
- 6.Sharma P, Jain S, Nigam S, Bahadur AK, Ouseph MM. Malignant fibrous histiocytoma of the chest wall masquerading as medullary Breast carcinoma- A case report. Acta Cytol. 2006;50:577–80. doi: 10.1159/000326020. [DOI] [PubMed] [Google Scholar]
- 7.Fletcher CD. The evolving classification of soft tissue tumours: An update based on the new WHO classification. Histopathology. 2006;48:3–12. doi: 10.1111/j.1365-2559.2005.02284.x. [DOI] [PubMed] [Google Scholar]
- 8.Adem C, Reynolds C, Ingle JN, Nascimento AG. Primary breast sarcoma: Clinicopathologic series from the Mayo clinic and review of the literature. Br J Cancer. 2004;91:237–41. doi: 10.1038/sj.bjc.6601920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hartel PH, Bratthauer G, Hartel JV, Fanburg-Smith JC. Primary malignant fibrous histiocytoma (myxofibrosarcoma/pleomorphic sarcoma not otherwise specified) of the breast: Clinicopathologic study of 19 cases. Ann Diagn Pathol. 2011;15:407–13. doi: 10.1016/j.anndiagpath.2011.05.007. [DOI] [PubMed] [Google Scholar]