

Abstract
Background:
Coronary artery bypass graft is one of common cardiac surgeries which unfortunately accompany with some adverse events such as delirium. Proinflammatory processes play an important role in pathogenesis of post-operative delirium. Therefore, the effect of dexamethasone (DEX) on post-operative delirium after cardiac surgery was evaluated.
Materials and Methods:
This randomized clinical trial study was conducted with objective of evaluation of DEX effects on post-operative deliriums and complications after cardiac surgery. Ninety three eligible patients who undergone coronary arteries bypass graft was divided into two groups of DEX with 43 patients and placebo (PCB) with 50 patients. DEX group taken 8 mg DEX intra-venous before induction of anesthesia followed by 8 mg every 8 h for 3 day and other group received PCB in same way.
Results:
All patients assessed by Mini-mental status questionnaire and psychiatric interviewing with aim of diagnosing delirium. Extubation time of DEX group was significantly reduced. The first post-operative day deliriums, extubation time, hospital, and intensive-care unit length of stay significantly reduced in DEX group without increasing serious complications such as infectious disease. After administration of DEX only hyperglycemia as an adverse event was increased in DEX group. Other complications of renal, cardiac, cerebrovascular and respiratory system did not show any significant differences between groups.
Conclusion:
Pre-operative administration of DEX might safely protect brain of the patients who undergone cardiac surgery against post-operative delirium.
Keywords: Cardiac surgery, clinical trial, delirium, dexamethasone
INTRODUCTION
Coronary artery bypass graft (CABG) is one of most common modality for treating damaged coronary arteries and performed in order to improve quality of life, especially, in its mental and physical aspects.[1,2] However, complications of CABG vary from minor symptoms to fatal brain injuries.[3] Impairment of memory, concentration, and language comprehension are related to post-operative cognitive disorders.[3] Cognitive impairment occurs in 15-80% of patients undergone CABG, and associated with increased mortality, hospital lengths of stay with long-term effects on individuals life.[4,5]
The main cause of this neuropsychological impairment is still unknown; nevertheless, despite of advances in CABG procedure and cardiopulmonary bypass (CPB), evidences suggest that CPB act as trigger for neuropsychological disorders.[6] CPB led to a systemic inflammatory response syndrome (SIRS), which understood to be associated with cognitive decline.[7,8] Enzymes and proinflammatory cytokines that released by monocytes and neutrophils, in collaboration with reactive oxygen species may result in cerebral damage and brain edema secondary to vasodilatation and fluid leak into brain-tissue.[9,10,11] Today, Corticosteroids considered as an anti-inflammatory strategy to interrupting inflammatory events after CPB.[12,13] Potential Inhibition of proinflammatory response by corticosteroids might improve outcomes such as improvement of myocardial function, reduction of extubation time, shortening of intensive-care unit (ICU), and hospital length of stay (LOS).[13,14]
Beneficial effect of dexamethasone (DEX) on neurological seqsuelae has been showed previously, but its value in context of cardiac surgery is still remained controversial.[12,15] Despite of high incidence of neurologic deficits and importance of immediate post-operative period, There are a few literatures have been found which evaluating this period.[16] According to our searches in available databases, there is a little knowledge about effects of DEX on post-cardiac surgery cognitive disorders. Therefore, this study was conducted with aim of evaluation of DEX effects on post-operative delirium and complications after cardiac surgery.
MATERIALS AND METHODS
Study design
This randomized clinical trial was performed from January of 2009 to February 2011. This study was carried out in Chamran heart center, which is one of teaching hospitals of Isfahan University of medical sciences. All male and female patients undergone elective CABG were included in our study. Exclusion criteria were longer duration of CPB (more than 3 h), age older than 80 years, Ejection Fraction (EF) lower than 20%, instability of hemodynamic, history of delirium, emergency operation, and inability of fulfillment of Mini-mental status examination (MMSE) questionnaire.
In the present study, the samples were selected using simple random sample method. Totally, 110 patients who had undergone CABG were eligible for this study. Informed consent was obtained from patients before their participation and they were randomly divided by means of Microsoft office excel 2007 software into two groups with same size (n = 55). During the study 17 patients were excluded because of death (n = 9), intubation more than 24 h (n = 5), and refusal to complete survey (n = 3). Hence, totally 93 patients were remained in the groups of DEX (n = 43), and placebo (PCB) (n = 50). Patients were received DEX or PCB as follows: 8 mg of intra-venous DEX was administrated to DEX group immediately before surgery and followed by 8 mg (2 ml) every 8 h for the first three post-operative days (POD). This method was repeated for PCB group using equal volume of normal saline 0.9% (as PCB) instead of DEX.
Anesthesia and surgical methods
After performing routine care and cardio-respiratory monitoring for all subjects, they were received a constant anesthesia. Surgery was performed under moderate hypothermia (28-30°C) approach. After institution of CPB at flow rate of 2.4 L/.min-1.M-2, aorta was cross-clamped and potassium cardioplagia administrated. During surgery, radial arterial pressure was preserved in range of 60-80 mmHg with low-dose norepinephrine. After anastomosing grafts and repairing valves (if it was indicated), cross clamp was removed and patient's body was rewarmed. Moreover, after transferring patients to ICU, all of them were profited from protocolled managements includes sitting of mechanical ventilation, fast-tracking, administrating low-dose nitrates and dobutamine, and antibiotic therapy. Blood glucose was routinely monitored in ICU at interval of every 6 h and hyperglycemia managed according to ICU protocol by continuous infusion of insulin. The target goal of blood glucose was 80-180 mg/dl in this protocol.
Psychological methods
The participants’ cognitive status was assessed by using MMSE as a screening method for diagnosing probable cognitive impairment. The MMSE questionnaire was completed in pre-operative day (PROD), first, second, and third (POD1, 2, 3) for each participant. Patients were not examined in operative day because of surgery, anesthesia, intubation, and psychological stresses. The MMSE screening questionnaire, which evaluating general mental status, includes 11 items with maximum score of 30 point.[17] Total score of less than 23 was considered as a possible indicator for cognitive impairment. Hence, the diagnostic criteria to confirmation of diagnosis in patients who has been obtained score of 23 or less were based on Diagnostic and Statistical Manual of Mental Disorders DSM-IV criteria. In other words, delirium disorder was diagnosed if DSM-IV criteria were met in a patient.
Data analysis
Continuous variables of study described by Mean and standard deviation (SD) values that in this study shown by mean ± SD. Additionally, Frequency and percent of categorical variables are indicating as frequency (percent) and determined by means of descriptive statistic. After verifying normality of continuous variables by using one-sample Kolmogorov-Smirnov test. Then, analysis of comparison between continuous data of Study's groups (DEX and PCB groups) performed by using independent-sample t-test. In order to find any noticeable difference between and within groups we analyzed categorical statistics by χ2 or Fisher's exact test (as appropriate). In all of the tests, P value < 0.05 was considered as significant level. All analysis was performed by using SPSS software (version 16, SPSS Inc.).
RESULTS
A total of 93 patients participated in the study groups (DEX and PCB). Table 1 consist summarization of comparisons of pre-, intra-, and post-operative characteristics for two groups. As shown in Table 1, there is no significant difference were noted in pre-operative baseline characteristics of the groups. Those variables includes age, left ventricular ejection fraction, gender, history of cerebrovascular attack, chronic renal failure, Debates Mellitus, hypertension, chronic obstructive pulmonary disease, carotid bruit, recent myocardial infarction, cigarettes smoking, and alcohol. In similarity, intra-operative variables had not statistically meaningful difference in using of intra-aortic balloon pump (IABP), CABG operation with or without valve repair, number of grafts, cross-clamp time, pump time, average intra-operative hemoglobin, and temperature between groups. Analysis of post-operative data revealed that the patients of DEX group were significantly intubated for a shorter time (P = 0.04). In other words, mean extubation time of DEX group was 9.18 ± 2.40 h, however, for PCB group it was 10.56 ± 3.86 h. Other significant difference was seen in mean of post-operative blood sugar between groups (P = 0.007), which DEX group had mean blood glucose 245 ± 68 mg/dl versus 212 ± 45 mg/dl in PCB group.
Table 1.
Comparison of medical characteristics between the groups
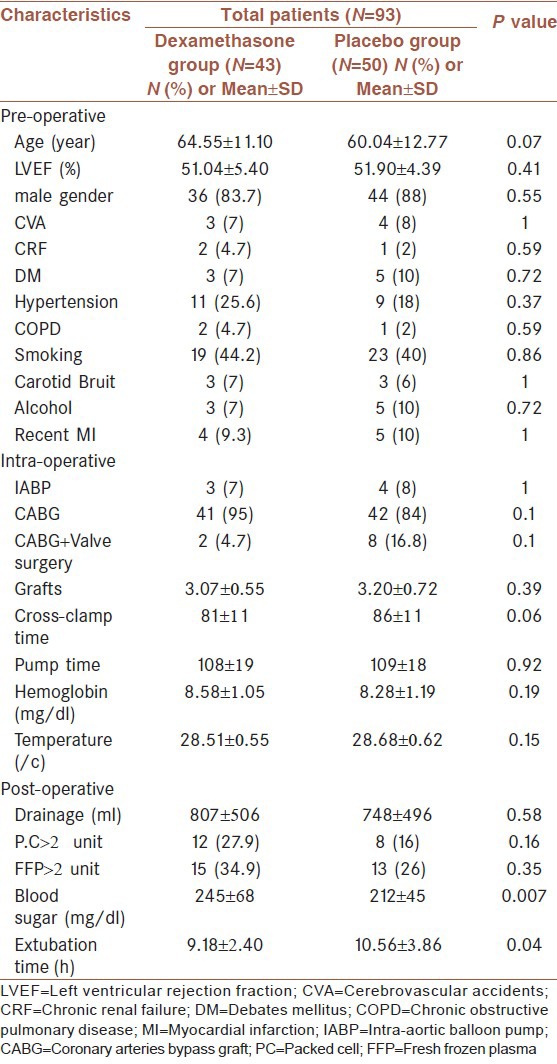
The other Intra-operative variables includes chest tube drainage volume, transfusion of packed cell and fresh frozen plasma more than 2 units, arterial partial pressure of carbon dioxide more than 50 mmHg, and arterial partial pressure of oxygen less than 60 mmHg. These variables statistics did not show any significant difference between the groups.
The psychometric results of MMSE questionnaire in PROD and POD presented in Table 2. According to these results, there is no significant difference between scores of DEX and PCB groups in PROD (28.63 ± 3.06 vs. 27.84 ± 3.15, respectively, P = 0.1). Although, the DEX group compared to the PCB group obtained higher scores in POD1 (27.53 ± 3.44 vs. 25.78 ± 4.70, respectively, P = 0.04). DEX group significantly had a higher scores than PCB group in POD2 (28.12 ± 2.66 vs. 26.26 ± 4.20, respectively, P = 0.04). The scores of POD3 did not show any meaningful difference between the DEX and PCB groups (28.00 ± 3.08 vs. 27.40 ± 3.20, respectively, P = 0.36).
Table 2.
Comparison of mini mental status examination scores between the groups
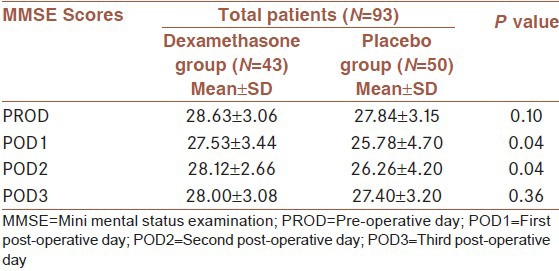
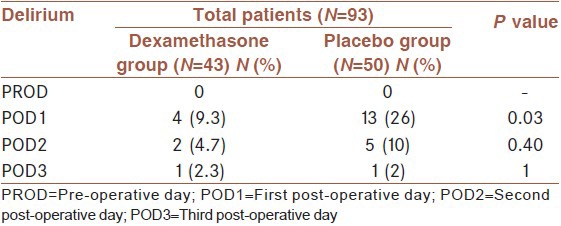
Table 3 demonstrates statistics of delirium incidences and shows that in this study basically none of subject was diagnosed as delirious in PROD. The results of POD1 were exhibited a significant reduction of delirium incidence in DEX in contrasted with PCB group (4 (9.3%) vs. 13 (26%), respectively, P = 0.03). The results of POD2 did not show any significant difference between DEX and PCB groups (2 (4.7%) vs. 5 (10%), respectively, P = 0.40). In the same way, there is no statistically difference in number of the patients who suffered from delirium in DEX versus PCB group in POD3 (1 (2.3%) vs. 1 (2%), respectively, P = 1).
Table 3.
Comparison of delirium incidences between the groups
As displayed in Table 4, the results showed that the patients of DEX group with 2.86 ± 1.3 days had a shorter ICU LOS than the patients of PCB group with 3.68 ± 1.33 days. In addition, the hospital LOS for DEX group was 12.93 ± 1.03 days versus 13.64 ± 1.75 days for the PCB group. Therefore, both parameters of ICU and hospital LOS was significantly shorter in the DEX group (P = 0.004, P = 0.02, respectively).
Table 4.
Comparison of hospital outcomes between the groups

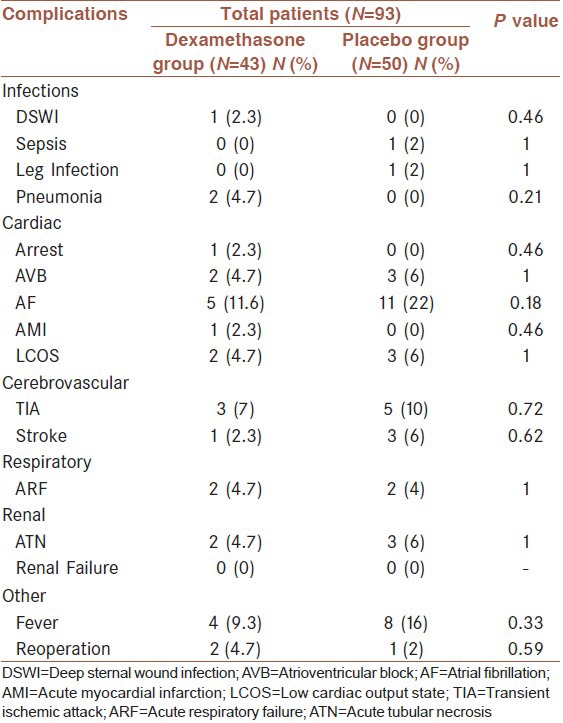
Table 5 depicted comparison of post-operative complications between the two groups. Analysis of this variables shows that there is no significant difference in post-operative complication rates. The results shows that occurrences of deep sternal wound infection, leg infection, sepsis, and pneumonia did not statistically differed between the groups. In addition, cardiac complications including acute myocardial infarction, cardiac arrest, atrioventricular block, atrial fibrillation (AF), and low cardiac output state were not statistically different. There is no significant difference in cerebrovascular (transient ischemic attack, stroke), respiratory (acute respiratory failure), and renal (acute tubular necrosis, renal failure) systems was seen.
Table 5.
Comparison of post-operative complications between the groups
DISCUSSION
Generally, post-cardiac surgery delirium may be due to complicated neurobiological factors, such as inflammatory responses, cytokines, and hypoxemia.[5] These factors predispose patients for delirium after establishment of CPB. Ischemia-reperfusion damage during CPB leads to activation of inflammatory cytokines, oxidative stress, and production of reactive oxygen species, which increasing blood brain barrier (BBB) permeability.[18,19] Breakdown of BBB integrity precipitate destruction of brain parenchyma.[20] Finally, infiltration of Inflammatory cells into the damaged cerebral tissue causes extension of water inflow into brain which leading to brain edema and cell dysfunction.[9,20,21] In summary, overload of proinflammatory cytokines inflowing into the brain can cause dysfunction of the autonomic nervous and neuroendocrine systems that may result in delirium.[22] Consequently, DEX with its modulatory effect on inflammatory mediators (tissue plasminogen activator, IL-6, IL8, and TNF-α) and disruption of above processes might have positive effects on reduction of delirium after utilization of CPB.[23] We believed that DEX played a brain protective role by interruption of this consequence.
According to our knowledge, there is no study that evaluated DEX effect on delirium incidence after cardiac surgery. In present study, we focus on effect of administration of DEX on post-operative incidence of delirium. Furthermore, this study compares the rates of complications and secondary outcomes between groups during hospitalization.
In our study, we used MMSE questionnaire as a primary screening tool. The results did not show any significant difference in PROD, which this means the global mental status of both of DEX and PCB groups, was same together. Unsurprisingly, the MMSE scores were decreased after cardiac surgery. Although, according to results of POD1 this significant decrease was more obvious in PCB group rather than DEX group. In the same way, MMSE scores of POD2 shows that the patients of DEX group had a better cognitive status in comparing to PCB group. Although, It is shown that delirium associated with lower MMSE scores in several studies however, there are some of other studies which does not prove the correlation of MMSE scores and delirium.[5,24,25] This discrepancy may be related to some issues of sensitivity/specificity of MMSE test and its limitations. In addition, previously was shown that highest sensitivity to cognitive impairments is in cut-off point 23/24 that can indicate possible cognitive impairment.[25,26] Therefore, recommended that diagnosis with MMSE must be based on clinical features of patients.[26]
As mentioned above, unfortunately MMSE scores is not very reliable diagnostic test. Thus, psychiatric interviewing is the choice approach for validation of diagnosis of delirium. Similar to MMSE scores, the incidence of delirium was lower in DEX group in POD1, 2 though only the result of POD1 was significant. The incidence of delirium in POD3 was too similar in the both groups. We believe that these results are not one of statistical errors and DEX really protects brains from damages. We hypothesizes that the maximum effect of DEX is in first POD because of maximum of inflammatory responses occurs in this period. As mentioned above, establishment of CPB by activation of proinflammatory cytokines express as SIRS, which can effect on cerebrum by several mechanisms including of hypoxia and increasing vascular permeability, and secondary brain tissue damage and edema. Previously, the studies found that DEX protect brain and its global function (e.g., learning, memory) by reduction of cerebral tissue death that due to cytokines and ischemia.[27] And results of our study are a new evidence for cerebral protection effect of DEX. In other way, there is a strong relationship between cortisol and cognitive impairment disorders. DEX with its negative feedback on Hypothalamic-pituitary-adrenal (HPA) axis initiates decreasing of cortisol and theoretically may be a useful strategy for decreasing of post-cardiac surgery deliriums.[28] Researchers, who studied this mechanism of DEX however, not after CPB, discovered a wide range of contradictory results.[28] With regard of these controversies should be mentioned that DEX effect on cognition is dose dependent. In detail, cortisol has an inverted U-shape dose response effect on cognition, that means presence of extreme low or high level of serum cortisol (which regulated by DEX level) impose brain to show cognitive symptoms. Seems DEX might worsen mental condition of some pathological disturbances (e.g., Cushing syndrome, Alzheimer's disease), which suffer from HPA axis dysregulation.[28,29] Any way in comparison with any other triggers, pathogenesis of post-cardiac surgery delirium rather linked with inflammatory phenomena.[30] Hence, we think DEX reduced delirium incidence with its anti-inflammatory properties because of greatest difference was seen in closest times to CPB. In other words, in comparison with the PCB group, the DEX group had a lower incidence in both of POD1, two but only in POD1 was significant which this day is nearer to CPB.
In one study, the advantageous effects of DEX in reduction of inflammatory responses after CPB manifested as decreased adverse effects and consequently better outcomes after cardiac surgery.[31] This prospect was experienced by Prasongsukarn et al.23 who used corticosteroids (1 g methylprednisolone before CPB and 4 mg DEX) in the first day post-cardiac surgery. They were reported that consequential unfavorable events of cardiac surgery, which assumed to be related to reduction of inflammatory cascade and cytokines significantly reduced. Results of their study were shown significant reduction of AF rhythm occurrence after cardiac surgery after steroid therapy. This report supports by our results, which shown AF occurred in DEX group with a lower incidence however this decline was not statistically significant. In contrast with our results, study of Prasongsukarn et al. showed that DEX correlate with longer hospital LOS. This is could be due to more complications that were seen in their steroid group. In any way, incidence of post-operative complications between our groups (DEX and PCB) was not shows any significant difference. A recent meta-analysis, which evaluated effects of steroids on post-cardiac surgery complications indicated that ICU and hospital LOS has been totally reduced after administration of steroids.[32]
One of major concerns related to prophylaxis of DEX is risk of increase of post-operative infections.[33] Previously known that DEX may be having an association with higher incidences of infectious disease due to immunosuppression and hyperglycemia. Our results show that blood glucose of DEX group was significantly higher than PCB group nevertheless post-operative rate of infections was not any significant difference between DEX and PCB groups. We suppose low dose of DEX cannot noticeably increase incidence of post-operative infections because of DEX effect is dose dependent. Other studies, which support our results stated that DEX was not absolutely associated with higher incidences of infections.[32,33]
In addition, we found that DEX group had better outcomes than PCB group. The result of study indicated that the patients of DEX group were extubated sooner and they had significantly shorter time of intubation. This finding relatively is important because of longer intubation time is relating with more complications (e.g., ventilator associated pneumonia, and so forth). This hypothesis was experienced in study of Yared et al.14 who confirm valuable effect of DEX in early extubation of patients after cardiac surgery. They stated that this effect might due to reduction of shivering and fever. Furthermore, we believe that other reason of early extubation was lower incidence of delirium in DEX group. Because of hypnotic-sedative agents which administrating for delirium management, lower incidences of delirium can result in earlier awakening and extubation of patients. The full consciousness and obedience of patients are necessary for extubation and administrations of hypnotic-sedative medications may delay this awakening of patients. Therefore, DEX could cause early extubation due to protection of brain against cognitive decline and delirium.
Literatures recommended that anti-inflammatory strategies such as administration of glucocorticoids, might improve cognitive dysfunction after cardiac surgery, despite of lack of information about effects of DEX on delirium after CPB.[34] Our results might be a proof for such recommendations. These results shown that DEX significantly keep more appropriate brain function after establishment of CPB without any serious complications. In other words, prophylaxis of DEX can place on pre-operative management of patients who underwent cardiac surgery.
Although, we take into account probability of several known and unknown factors that maybe influence on our results. In this regard, it is supposed that post-cardiac surgery delirium is relating to Intra-operative factors such as complexity of surgery, longer duration of CPB, cross-clamp time, and using of IABP. Therefore, our concern arisen in this atmosphere because of possibility of synergetic interference of these factors, which might contribute to causing higher incidence of delirium in PCB. With take into consideration the limitations of our study; we are declaring that approval of prophylaxis of DEX need to conduction of similar studies by same methodology but with larger subject population. According to our knowledge, many factors have influence on mental response to corticosteroids such as subjects’ mood, medications, and even their hormonal level status. In any way, our results strongly support that prophylaxis of DEX can effectively reducing post-cardiac surgery delirium.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Weisberg AD, Weisberg EL, Wilson JM, Collard CD. Preoperative evaluation and preparation of the patient for cardiac surgery. Med Clin North Am. 2009;93:979–94. doi: 10.1016/j.mcna.2009.05.001. [DOI] [PubMed] [Google Scholar]
- 2.Barry LC, Kasl SV, Lichtman J, Vaccarino V, Krumholz HM. Social support and change in health-related quality of life 6 months after coronary artery bypass grafting. J Psychosom Res. 2006;60:185–93. doi: 10.1016/j.jpsychores.2005.06.080. [DOI] [PubMed] [Google Scholar]
- 3.Ramlawi B, Rudolph JL, Mieno S, Feng J, Boodhwani M, Khabbaz K, et al. C-Reactive protein and inflammatory response associated to neurocognitive decline following cardiac surgery. Surgery. 2006;140:221–6. doi: 10.1016/j.surg.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 4.Rosengart TK, Sweet JJ, Finnin E, Wolfe P, Cashy J, Hahn E, et al. Stable cognition after coronary artery bypass grafting: Comparisons with percutaneous intervention and normal controls. Ann Thorac Surg. 2006;82:597–607. doi: 10.1016/j.athoracsur.2006.03.026. [DOI] [PubMed] [Google Scholar]
- 5.Hopkins RO, Jackson JC. Assessing neurocognitive outcomes after critical illness: Are delirium and long-term cognitive impairments related? Curr Opin Crit Care. 2006;12:388–94. doi: 10.1097/01.ccx.0000244115.24000.f5. [DOI] [PubMed] [Google Scholar]
- 6.Stroobant N, Van Nooten G, Belleghem Y, Vingerhoets G. Short-term and long-term neurocognitive outcome in on-pump versus off-pump CABG. Eur J Cardiothorac Surg. 2002;22:559–64. doi: 10.1016/s1010-7940(02)00409-8. [DOI] [PubMed] [Google Scholar]
- 7.Kozora E, Kongs S, Collins JF, Hattler B, Baltz J, Hampton M, et al. Cognitive outcomes after on- versus off-pump coronary artery bypass surgery. Ann Thorac Surg. 2010;90:1134–41. doi: 10.1016/j.athoracsur.2010.05.076. [DOI] [PubMed] [Google Scholar]
- 8.Reis Miranda D, Gommers D, Struijs A, Dekker R, Mekel J, Feelders R, et al. Ventilation according to the open lung concept attenuates pulmonary inflammatory response in cardiac surgery. Eur J Cardiothorac Surg. 2005;28:889–95. doi: 10.1016/j.ejcts.2005.10.007. [DOI] [PubMed] [Google Scholar]
- 9.Gazit AZ, Huddleston CB, Checchia PA, Fehr J, Pezzella AT. Care of the pediatric cardiac surgery patient–Part 1. Curr Probl Surg. 2010;47:185–250. doi: 10.1067/j.cpsurg.2009.11.006. [DOI] [PubMed] [Google Scholar]
- 10.Franke A, Lante W, Markewitz A, Weinhold C. In vitro restoration of post-operatively decreased IFN-gamma levels after cardiac surgery and its effect on pro- and anti-inflammatory mediators. J Surg Res. 2006;136:266–72. doi: 10.1016/j.jss.2006.06.036. [DOI] [PubMed] [Google Scholar]
- 11.Parnell AD, Massey NJ. Postoperative care of the adult cardiac surgical patient. Anaesth Intensive Care Med. 2009;10:430–6. [Google Scholar]
- 12.Larmann J, Theilmeier G. Inflammatory response to cardiac surgery: Cardiopulmonary bypass versus non-cardiopulmonary bypass surgery. Best Pract Res Clin Anaesthesiol. 2004;18:425–38. doi: 10.1016/j.bpa.2003.12.004. [DOI] [PubMed] [Google Scholar]
- 13.Marik PE, Fromm R. The efficacy and dosage effect of corticosteroids for the prevention of atrial fibrillation after cardiac surgery: A systematic review. J Crit Care. 2009;24:458–63. doi: 10.1016/j.jcrc.2008.10.016. [DOI] [PubMed] [Google Scholar]
- 14.Yared JP, Starr NJ, Torres FK, Bashour CA, Bourdakos G, Piedmonte M, et al. Effects of single dose, postinduction dexamethasone on recovery after cardiac surgery. Ann Thorac Surg. 2000;69:1420–4. doi: 10.1016/s0003-4975(00)01180-2. [DOI] [PubMed] [Google Scholar]
- 15.Irazuzta J, Pretzlaff RK, DeCourten-Myers G, Zemlan F, Zingarelli B. Dexamethasone decreases neurological sequelae and caspase activity. Intensive Care Med. 2005;31:146–50. doi: 10.1007/s00134-004-2462-7. [DOI] [PubMed] [Google Scholar]
- 16.Bickert AT, Gallagher C, Reiner A, Hager WJ, Stecker MM. Nursing neurologic assessments after cardiac operations. Ann Thorac Surg. 2008;85:554–60. doi: 10.1016/j.athoracsur.2007.09.050. [DOI] [PubMed] [Google Scholar]
- 17.Nelson A, Fogel BS, Faust D. Bedside cognitive screening instruments. A critical assessment. J Nerv Ment Dis. 1986;174:73–83. doi: 10.1097/00005053-198602000-00002. [DOI] [PubMed] [Google Scholar]
- 18.Hoffman WH, Stamatovic SM, Andjelkovic AV. Inflammatory mediators and blood brain barrier disruption in fatal brain edema of diabetic ketoacidosis. Brain Res. 2009;1254:138–48. doi: 10.1016/j.brainres.2008.11.100. [DOI] [PubMed] [Google Scholar]
- 19.Joashi U, Tibby SM, Turner C, Mayer A, Austin C, Anderson D, et al. Soluble Fas may be a proinflammatory marker after cardiopulmonary bypass in children. J Thorac Cardiovasc Surg. 2002;123:137–44. doi: 10.1067/mtc.2002.118685. [DOI] [PubMed] [Google Scholar]
- 20.Wasserman JK, Schlichter LC. Minocycline protects the blood-brain barrier and reduces edema following intracerebral hemorrhage in the rat. Exp Neurol. 2007;207:227–37. doi: 10.1016/j.expneurol.2007.06.025. [DOI] [PubMed] [Google Scholar]
- 21.Nakamura K, Ueno T, Yamamoto H, Iguro Y, Yamada K, Sakata R. Relationship between cerebral injury and inflammatory responses in patients undergoing cardiac surgery with cardiopulmonary bypass. Cytokine. 2005;29:95–104. doi: 10.1016/j.cyto.2004.10.002. [DOI] [PubMed] [Google Scholar]
- 22.Ebersoldt M, Sharshar T, Annane D. Sepsis-associated delirium. Intensive Care Med. 2007;33:941–50. doi: 10.1007/s00134-007-0622-2. [DOI] [PubMed] [Google Scholar]
- 23.Prasongsukarn K, Abel JG, Jamieson WR, Cheung A, Russell JA, Walley KR, et al. The effects of steroids on the occurrence of postoperative atrial fibrillation after coronary artery bypass grafting surgery: A prospective randomized trial. J Thorac Cardiovasc Surg. 2005;130:93–8. doi: 10.1016/j.jtcvs.2004.09.014. [DOI] [PubMed] [Google Scholar]
- 24.van der Mast RC, van den Broek WW, Fekkes D, Pepplinkhuizen L, Habbema JD. Incidence of and preoperative predictors for delirium after cardiac surgery. J Psychosom Res. 1999;46:479–83. doi: 10.1016/s0022-3999(99)00002-1. [DOI] [PubMed] [Google Scholar]
- 25.Jankowski CJ, Trenerry MR, Cook DJ, Buenvenida SL, Stevens SR, Schroeder DR, et al. Cognitive and functional predictors and sequelae of postoperative delirium in elderly patients undergoing elective joint arthroplasty. Anesth Analg. 2011;112:1186–93. doi: 10.1213/ANE.0b013e318211501b. [DOI] [PubMed] [Google Scholar]
- 26.Wind AW, Schellevis FG, Van Staveren G, Scholten RP, Jonker C, Van Eijk JT. Limitations of the Mini-Mental State Examination in diagnosing dementia in general practice. Int J Geriatr Psychiatry. 1997;12:101–8. doi: 10.1002/(sici)1099-1166(199701)12:1<101::aid-gps469>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 27.Feng Y, Rhodes PG, Liu H, Bhatt AJ. Dexamethasone induces neurodegeneration but also up-regulates vascular endothelial growth factor A in neonatal rat brains. Neuroscience. 2009;158:823–32. doi: 10.1016/j.neuroscience.2008.10.024. [DOI] [PubMed] [Google Scholar]
- 28.Belanoff JK, Gross K, Yager A, Schatzberg AF. Corticosteroids and cognition. J Psychiatr Res. 2001;35:127–45. doi: 10.1016/s0022-3956(01)00018-8. [DOI] [PubMed] [Google Scholar]
- 29.Gurevich D, Siegel B, Dumlao M, Perl E, Chaitin P, Bagne C, et al. HPA axis responsivity to dexamethasone and cognitive impairment in dementia. Prog Neuropsychopharmacol Biol Psychiatry. 1990;14:297–308. doi: 10.1016/0278-5846(90)90018-c. [DOI] [PubMed] [Google Scholar]
- 30.Gao L, Taha R, Gauvin D, Othmen LB, Wang Y, Blaise G. Postoperative cognitive dysfunction after cardiac surgery. Chest. 2005;128:3664–70. doi: 10.1378/chest.128.5.3664. [DOI] [PubMed] [Google Scholar]
- 31.El Azab SR, Rosseel PM, de Lange JJ, Groeneveld AB, van Strik R, van Wijk EM, et al. Dexamethasone decreases the pro- to anti-inflammatory cytokine ratio during cardiac surgery. Br J Anaesth. 2002;88:496–501. doi: 10.1093/bja/88.4.496. [DOI] [PubMed] [Google Scholar]
- 32.Cappabianca G, Rotunno C, de Luca Tupputi Schinosa L, Ranieri VM, Paparella D. Protective effects of steroids in cardiac surgery: A meta-analysis of randomized double-blind trials. J Cardiothorac Vasc Anesth. 2011;25:156–65. doi: 10.1053/j.jvca.2010.03.015. [DOI] [PubMed] [Google Scholar]
- 33.Price J, Tee R, Lam BK, Hendry P, Green MS, Rubens FD. Current use of prophylactic strategies for postoperative atrial fibrillation: A survey of Canadian cardiac surgeons. Ann Thorac Surg. 2009;88:106–10. doi: 10.1016/j.athoracsur.2009.03.059. [DOI] [PubMed] [Google Scholar]
- 34.Kadoi Y. Pharmacological neuroprotection during cardiac surgery. Asian Cardiovasc Thorac Ann. 2007;15:167–77. doi: 10.1177/021849230701500220. [DOI] [PubMed] [Google Scholar]