

Abstract
Purpose
Epidemiologists have long contributed to policy efforts to address health disparities. Three examples illustrate how epidemiologists have addressed health disparities in the U.S. and abroad through a “social determinants of health” lens.
Methods
To identify examples of how epidemiologic research has been applied to reduce health disparities, we queried epidemiologists engaged in disparities research in the U.S., Canada, and New Zealand, and drew upon the scientific literature.
Results
Resulting examples covered a wide range of topic areas. Three areas selected for their contributions to policy were: 1) epidemiology's role in definition and measurement, 2) the study of housing and asthma, and 3) the study of food policy strategies to reduce health disparities. While epidemiologic research has done much to define and quantify health inequalities, it has generally been less successful at producing evidence that would identify targets for health equity intervention. Epidemiologists have a role to play in measurement and basic surveillance, etiologic research, intervention research, and evaluation research. However, our training and funding sources generally place greatest emphasis on surveillance and etiologic research. Conclusions: The complexity of health disparities requires better training for epidemiologists to effectively work in multidisciplinary teams. Together we can evaluate contextual and multilevel contributions to disease and study intervention programs in order to gain better insights into evidenced-based health equity strategies.
Keywords: Health Status Disparities, Healthcare Disparities, Minority Health, Epidemiology, Policy, Socioeconomic Factors
“If all epidemiologists stop short of helping to affect policy, then the voice of science will be lost from making decisions that most affect the health of the public.” (1).
Introduction
Results of the 2010 U.S. Census suggest that as the growth of Black, Hispanic and Asian ethnic groups continues to accelerate, there will be a “minority majority” as early as 2042, when Hispanics (of any race) will comprise 24 percent of the population, Blacks 15 percent and Asians 8 percent (2). This majority of racial/ethnic minorities will occur even earlier (2023) among children and adolescents (2). Addressing their health needs, especially in the face of growing evidence of continued and severe health disparities for many racial/ethnic groups, is challenging for health care and public health.
Knowledge of the range and complexity of health disparities has evolved as a result of data collection on race and ethnicity in epidemiologic surveillance and research (3). In addition, epidemiologists have long been involved in policy efforts to address health disparities beyond the conduct, analysis, interpretation and dissemination of health data. These efforts have included preparation of governmental reports (4-6), managing policy offices (7), identifying priorities for initiatives (8-10), and providing policy guidance (11).
There are many routes from epidemiologic activity to policy formation: surveillance raises awareness of an issue, measurement research progressively refines exposures and outcomes, etiologic research identifies causal relations in natural settings, intervention research pilots potential actions, and evaluation research considers impacts of policies. The development and implementation of policies, including laws, regulations, and judicial decrees, includes advocacy in support of all these efforts. Albert Szent-Gyorgi described three “faces” of science as: 1) a way of thinking about things (evidence, objectivity, and a “cool head”), 2) the results and their applications, and 3) the scientist's moral code (12). The three “faces” are interrelated: from science come results and these may be applied through attendant public policies.
Epidemiologists wear all three of these “faces,” and have come to recognize not only the importance of values in many aspects of professional practice, but also the need for ethical guidance that regulates our public behavior. Representing the “science of public health,” epidemiologists are naturally the most qualified to interpret the epidemiologic studies used to set public health policy. As Weed has noted, the bioethical principle of beneficence provides moral justification for advocacy (12).
Epidemiologic research to address health disparities has also evolved, through the four phases of health disparities research (13). The first phase of health disparities research has been the identification of the nature and extent of disparities (4). The second phase identified underlying factors for racial, ethnic and socioeconomic disparities. The third phase, the development and implementation of interventions (14), increasingly includes transdisciplinary research, community engagement, and knowledge translation. The fourth phase encompasses a mixed methods approach to evaluation of comprehensive, multilevel interventions. Classical epidemiologic approaches and training provide a good basis for contributions to the first two phases, however, this review highlights a need to expand training for epidemiologists to encompass the complexity of health disparities and address contextual social determinants that contribute to disease, and the foundation of successful health equity strategies that can reduce and/or eliminate health disparities.
All health behaviors, policies and interventions can impact on disparities. For this reason, we focus our attention on social determinants of health: policies and interventions that are targeted at social conditions, rather than medical care or individual behavior change. There is a long history of interventions on social conditions intended to reduce disparities. For example, Sara Josephine Baker (1873–1945) implemented public health interventions among the poor in New York City, including licensing midwives, encouraging breastfeeding, providing safe pasteurized milk and school lunches, school-based screening and maternal education initiatives (15). Likewise, Joseph Goldberger (1874–1929) was an advocate for scientific and social recognition of the links between poverty and disease. He noted that alleviation of poverty improved nutrition, which reduced pellagra in the rural poor (16).
Social context interventions tend to be non-specific in their impacts, but are often promoted on the basis of multiple motivations. Because they are “upstream” they generally have diverse consequences (intended and unintended). Social context interventions are also necessarily contextual, and observed effects in one setting often don't generalize well to others. Finally, social conditions are frequently associated with health outcomes in observational data, making both causal inference and anticipation of the effects of policy modifications inherently difficult.
In this review, we provide three examples of how epidemiologists have addressed health disparities through a “social determinants of health” lens. To identify examples of how epidemiology approaches health disparities, we broadly queried epidemiologists engaged in health disparities research in the US, Canada and New Zealand through listservs, LinkedIn, and personal communication. Potential cases offered covered a wide range of topics areas, including asthma, cancer screening and management, cardiovascular disease, data development, nutrition, food pricing, sexually transmitted infections, HIV/AIDS, child and adult immunizations, health services, and other topics. We were interested in highlighting examples that had a “social determinants of health” focus, had not already been discussed in the American College of Epidemiology's epidemiology and policy series, and had multiple applications, either in the U.S. or abroad.
Theoretical Framework for Causal Effects of Policies
Health policy interventions are enacted among populations to influence outcomes through various mechanisms. The impacts of population-level policies lead to individual-level effects measured at the aggregate level (17). Consider the example of a policy designed to increase physical activity among children attending school-based physical education classes (18, 19). At the individual level, children may respond to the program by increasing their physical activity while attending classes. Suppose that each targeted school later reports that the overall prevalence of childhood obesity has decreased among children attending the school. It therefore appears that the physical activity policy has influenced childhood obesity rates. But is the observed change in obesity equal to the causal effect of the intervention? Could the measured effect be confounded by social or behavioral factors that affect obesity in the students at some of the schools?
If such factors were to exist, then it would be necessary to adjust for these confounding variables in a statistical model. Epidemiologists often use a causal diagram to illustrate relations among factors relevant to an exposure-outcome association, to facilitate identification of a sufficient set of adjustments to reduce confounding, and to illustrate inappropriate adjustment for variables that are not confounders of the exposure effect of interest. A key criterion that epidemiologists should consider is whether adjusted factors are affected by the policy as opposed to determinants of policy implementation.
The following example provides an illustration of a graphical model to conceptualize the influence of a policy intervention on poor living conditions and its subsequent effect on childhood asthma exacerbations. Because causal diagrams require qualitative determinations of which factors to include, a critical review of existing evidence is required. Furthermore, causal diagrams present structural relations using available evidence at a given snapshot in time. Fortunately, these diagrams can be modified as new evidence becomes available. We encourage epidemiologists to develop and share their proposed graphical models with other researchers to promote transparency and to aid in the progressive accumulation of knowledge. Connecting the graphical model with the statistical modeling approach can promote a greater understanding of the analytic assumptions, and this can be helpful to the evaluation process needed to translate scientific findings into policy innovations (20).
Recent research suggests that poor living conditions (e.g., indoor allergens, environmental tobacco smoke, etc.) exacerbate asthma in children (21). Policies have been enacted to remediate these environmental factors from households (22). We are interested in quantifying the magnitude of the effect of the policy intervention on childhood asthma exacerbations. We recognize that the social environment and its effects on individual and population health occur at multiple levels and involve dynamic social interactions (23); therefore we use a simplified graphical model as a tool to illustrate some conditional dependencies among the interrelated variables in our small universe of measured factors that influence the outcome (24, 25).
Figure 1 is a graphical representation of the relations among some of the factors that influence childhood asthma exacerbations. This graph depicts one of many plausible mechanisms for the sequencing and inter-relations between the policy, the outcome and some important covariates. This illustrates the dependencies among the many levels in the data and provides transparency regarding assumptions so that they can be discussed and critiqued. These factors can be described as social (e.g., socioeconomic status), environmental (e.g., outdoor air pollution), and genetic variations, and can be defined concurrently at the individual and population levels. For example, outdoor air pollution occurs at a population level affecting individual level exposures to pollutants that can lead to asthma exacerbations (26). Circulating respiratory infections in the community, which occur throughout the year, increase the occurrence of asthmatic exacerbations in individual children infected with rhinoviruses, influenza, or other respiratory viruses (27).
Figure 1.
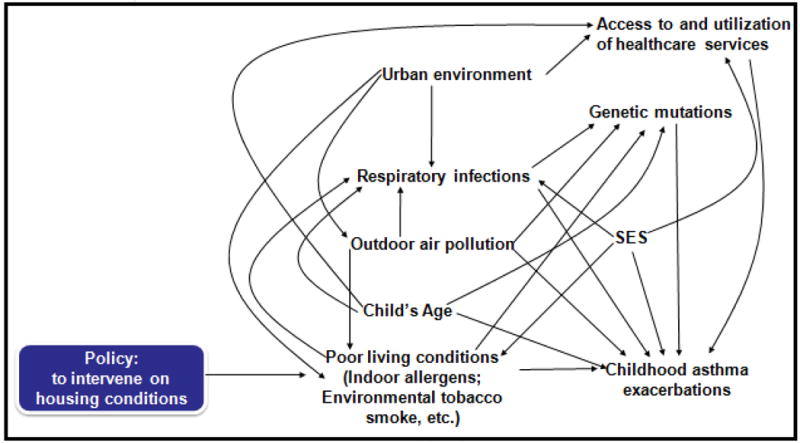
Proposed graphical representation illustrating the dependency assumptions for the influence of policy and caregiver decision-making to improve poor living conditions (i.e., reduce indoor allergens) on the occurrence of childhood asthma exacerbations
To estimate the causal effect on childhood asthma exacerbations of a potential policy of intervening on poor housing conditions, it is necessary to identify a sufficient set of covariates for which to adjust in an analytic model. Based on our assumptions, no adjustment is indicated because the policy is exogenous (i.e., there are no arrows leading into the policy node (25)). Adjustment for other variables, such as socioeconomic status (SES), which is not a cause of the policy intervention, would therefore result in a biased estimate of the total effect of the policy. While the policy is unconfounded in this network of factors, another exposure of potential interest may be. For example, we may be interested in determining whether installation of allergen reducing air filters in homes (as a subcomponent of a multi-faceted, in-home tailored intervention (28)) reduces childhood asthma compared to children living in homes without air filters (29). In this exposure-outcome relation, a sufficient set of covariates to adjust may include social factors such as SES. In more realistically elaborate graphs, it will often be the case that no set of observed variables would be sufficient for complete confounding control (30).
The Role of Epidemiology in Definition and Measurement
A primary goal of epidemiologic research is to provide an evidentiary basis for informed policy decisions, and this is no less true for policies that impact health through broad social determinants such as food, housing, schooling and employment. These “upstream” factors are all subject to important policy decisions on a routine basis, from tax and subsidy policies to targeted interventions, and clearly have the potential to affect health disparities positively or negatively. While health disparities are not the only consideration in setting such policies, they are an important one that can impact both cost-benefit calculations as well as the perceived social desirability of one policy over another in terms of overall equity, justice and social desirability.
Epidemiologic study of social determinants in relation to health disparities entails many significant challenges. The subject matter relevant to these exposures and the policies that regulate their distributions is often outside of typical training in epidemiology. Much of the available funding is tied to specific disease categories, but social determinants often have broad impacts across many diseases. Causal inference is difficult because the exposures are usually far from exogenous, leading many scientists to seek out natural experiments or other sources of random variation with which to make stronger conclusions (31). Finally, generalizability is often questionable because the exposures are experienced within social contexts that differ greatly across societies or race, gender, and class subgroups within societies.
Much descriptive epidemiology regarding health disparities is published each year. This work is constantly evolving and being refined by attention to novel axes of disparity (e.g., sexual orientation, wealth, and place) and by increasingly diverse methods of defining composite outcomes, such as disability adjusted life-years (DALYs), quality adjusted life-years (QALYs) and other composite measures (32). The definition of “health disparity” (and related terms such as “inequality” and “inequity”) has itself endured continual epidemiologic critique on conceptual grounds. Increasingly an emerging literature has challenged routine approaches of simple health comparisons across divergent social groups (33-37).
One major role for epidemiology on health disparities policy is through definition, classification and measurement, fundamental issues that are necessary for all evidenced-based decisions, and for which epidemiology has a long standing tradition of methodologic development. This work includes exposure assessment, outcome classification, and analysis of measurement error. On the exposure side, there have been dramatic developments in recent decades in the assessment of social determinants of health, in both conceptual and operational terms. Epidemiologists have been at the forefront in public health of refining conceptually valid and practically implementable measures of constructs such as racism, segregation, inequality, educational attainment and various forms of wealth and poverty in health studies (23). Likewise, on the outcomes side, assessment of disparities has evolved to encompass a wide variety of measures, each with unique advantages with respect to absolute or relative comparisons and the scaling of the dimension over which the outcomes are contrasted (38,39). These developments are crucial because the use of different exposure and outcome measures can generate dramatically different understandings of the relationships (40). Moreover, common descriptive techniques, such as routine standardization, can have artifactual influences on the disparity patterns that could sway policy-makers into an inaccurate perception of changes over time (41). One example that continues to motivate further work in the area of standardization is the collection of data on race and ethnicity. Current efforts are underway by HHS as directed by the Affordable Care Act to improve the monitoring of inequities not only by race but also by ethnicity, primary language, sex, and disability status. (42-45).
A concrete example in which the development of exposure indices has influenced policy for reduction of disparities is the advent of neighborhood quality indices, which summarize a wide variety of social indicators. For example, the Connecticut Association of Directors of Health's Health Equity Index assesses numerous domains including economic security, educational resources, transportation, civic involvement, housing quality, and environmental quality (46). It is used in policy evaluations to assess community change in relation to various interventions and policies.
Another example of neighborhood quality indices comes from New Zealand's “Social Reports (Te Pūrongo Oranga Tangata), which are used by government agencies to monitor social progress in health disparities (47). These reports have now gained a level of prominence in central and local government as a tool for surveillance within that country. In qualitative assessments of the value of this tool for policy makers, senior health officials from the Ministry of Health asserted that the institution of routine assessment and reporting, and the availability of content from these reports have assisted in both raising awareness and stimulating action to address the social determinants of health and improve health equity, both within and outside the health sector. Amongst civil society actors, too, these reports have gained currency with health advocacy agencies, health service providers, indigenous organizations, academic audiences and the media.
The Example of Housing and Asthma
Housing interventions to reduce asthma exacerbations among racial and ethnic minorities and the poor such as those conducted in Seattle-King County, Washington; Chicago, Illinois; and New Zealand are another example of a social contextual intervention to reduce health disparities. Asthma disproportionately affects minority and disadvantaged children, including residents of federally assisted housing (48-50). Racial and ethnic minority and low-income children are more likely to live in substandard housing with greater exposure to allergens and higher asthma sensitization rates due to crowding, pest infestations, poor ventilation, deteriorated carpeting, excessive moisture and dampness, poor ventilation, and structural deficits (51).
Since environmental conditions in the home can exacerbate asthma symptoms, housing interventions have included home assessment for asthma triggers (e.g., environmental tobacco smoke, dust mites, outdoor air pollution, cockroach allergen, pets, mold, wood smoke), provision of products and services to reduce exposure to asthma triggers (e.g., mattress cases, chemical methods to reduce dust mites), and asthma education on identification of asthma triggers and how to reduce exposure. Home-based multi-trigger, multi-component interventions with an environmental focus are recommended by the Task Force on Community Preventive Services for children and adolescents, but, not for adults due to insufficient evidence (52).
Several of the housing intervention programs have clear ties to community needs assessments. For example, Seattle's King County Department of Public Health conducts a health survey every three years and analyzes data by region and health planning area. Stemming from disparities identified in this survey, the Healthy Homes Project aimed to reduce exposure to indoor asthma triggers among low-income urban children with asthma (53-55). This project has been translated by Sinai Health Systems in Chicago (56), and included home visits by community health workers (57, 58).
The eight phases of the Sinai Model for Reducing Health Disparities and Improving Health included: a community survey (2002-2003), analysis and comparison of results with national and state data to locate community-level differences, wide dissemination of findings (2004-2007), partnership with community organizations to prioritize health concerns, location/development of potentially effective interventions, work with community based organizations (CBOs) to locate funding for interventions, implementation of interventions (e.g., The Westside Children's Asthma Partnership), and evaluation of interventions (59). Many challenges have been identified. For example, some medical center projects have been criticized, leading to shifts in the handling of factors such as community interaction and indirect costs. Some communities have not mounted interventions related to survey findings. In some cases budget crises and loss of funding have affected sustainability. In all cases, broad generalizability remains a concern. Oftentimes, limited funding for evaluation and dissemination has hindered the ability to assess program impact on participants and the larger community. Indeed, many housing intervention studies fail to examine the effectiveness of interventions over time (60, 61). Few housing interventions have moved from efficacy to effectiveness studies.
Multilevel interventions pose challenges for evaluation, making it hard to tease out the impact of specific components. As an example, community partners of Seattle-King County's Healthy Homes Project argued against having a “usual care” comparison group and therefore both intervention arms incorporated multiple components. Their low-intensity comparison group received a combination of home assessment of triggers, home action plans, limited education during the assessment visit and bedding encasements (62).
Evidence is lacking or mixed for key components of multilevel housing interventions in addressing asthma. Trials of chemical and/or physical methods to reduce dust mite exposure to date have sometimes been of poor quality, as noted by a Cochrane review which found that control measures to reduce exposure to dust mites or their products had no effect on lung function, asthma symptoms or medication scores (63). Moderate-quality evidence exists that repairing houses or remediation decreased asthma-related symptoms among adults, and acute care visits among children (64). Published reviews indicate evidence to support three of 11 interventions for asthma: multi-faceted, in-home, tailored asthma interventions; integrated pest management (cockroach allergen reduction); and moisture intrusion elimination (61, 65, 66). Recently, the Breathe Easy home project found that children and adolescents with asthma who moved into an asthma-friendly home (moisture-reduction features, enhanced ventilation systems, and materials that minimized dust and off-gassing) experienced large decreases in asthma morbidity and trigger exposure (67).
For epidemiologists to more fully contribute to development and evaluation of interventions such as these, education and training are needed that integrate contextual social and political aspects of community involvement, process and outcome evaluation of community level interventions, qualitative and mixed methods, and analytic techniques such as multilevel modeling (68). Epidemiologists also need to be prepared to address generalizability and sustainability concerns. Because of differences in populations, climate, predominant type of housing, housing codes and policies (e.g., enforcement, new construction guidelines), and exposure to other indoor and outdoor pollutants, modifications may be needed to match interventions to individual community needs and context. Contextualizability may be a better to concept to consider, since different places have different profiles. Detailed information on the content of interventions and context, and the processes that led to the interventions, are therefore needed to address generalizability concerns (60).
Food Policy Strategies to Reduce Health Disparities
Unequal distribution of healthy foods -- a significant factor in health disparities is an example of a contextual issue identified through epidemiologic data. Policies that increase access to healthy foods include healthy food financing initiatives or zoning ordinances to support farmers markets and corner store initiatives; zoning and other city ordinances that decrease access to unhealthy foods (e.g., limit fast-food restaurants); and pricing strategies that make healthy foods less expensive and unhealthy foods more expensive. For each of these policies, evaluation is key to documentation of the baseline disparity, and ensuring that short term and long term outcomes lead to a reduction in health disparities.
Over the last 10 years, a growing number of communities have implemented policies to increase access to healthy foods with a particular focus on areas of food deserts and food swamps. Promising polices include providing incentives that allow the installation of refrigeration units for the sale of fresh fruits and vegetables in convenience or corner stores; loans and zoning ordinances that promote large grocery stores, farmers markets and corner stores particularly within food deserts or food swamps; decreasing access to unhealthy foods through zoning ordinances such as those restricting fast food establishments; and implementing price strategies that reduce the costs for health foods through consolidated bids and Electronic Benefit Transfer (EBT)/Supplemental Nutrition Assistance Program (SNAP), (69, 70).
A number of communities, such as Louisville, Seattle and Philadelphia are working with local store owners to convert their retail establishments for the sale of fresh fruits and vegetables and healthy foods. In Charlotte, North Carolina, a farmers market was established on the grounds of the county health department through a change in the zoning ordinance. Between 2001 and 2005, the daily consumption of five or more fruits and vegetables among African Americans in North Carolina increased from 23.1% to 25.3%, while overall state-wide consumption of fruits and vegetable decreased from 21.7% to 17.5% (71). The documented increase in fruits and vegetable consumption among African Americans in North Carolina at a time when the general trend was in the opposite direction represents important changes in health behavior, however, additional evaluation is needed to determine the long term impact of these policies.
In addition to increasing access to healthy foods, another important strategy is decreasing access to unhealthy food. As an initial step, the community of South Los Angeles (LA) documented the paucity of large, regional and national chain supermarkets and overabundance of small local markets and convenience stores in South LA when compared with West LA (72). The community used this information to advocate for a two year moratorium of new fast food restaurants opening in the community; the rationale being that during this moratorium a plan would be developed and implemented to bring grocery stores and more healthy eating options into South LA (70). During the moratorium, several small stores started selling fruits and vegetables, the first farmers market in the region started accepting Women, Infants and Children (WIC) checks, and new supermarkets moved into South LA in 2010 (70, 73, 74). Subsequently the Los Angeles municipal code was amended to limit new fast food establishments from opening within ½ mile of an existing fast food establishment (73). While the impact of this moratorium on the health of the community still needs to be evaluated, West-Adam Baldwin Hills LA has passed a similar ordinance, and the city of Detroit is considering a similar ordinance. Menu calorie labeling has previously been suggested to have a bigger impact on overweight and obesity than banning new fast-food establishments (75) given continued access to unhealthy foods at gas stations and convenience stores. A recent analysis of 15 years of longitudinal data from the Coronary Artery Risk Development in Young Adults (CARDIA) study found evidence that zoning restrictions on fast food restaurants within three kilometers of low-income residents reduced consumption of fast food, while better access to supermarkets did not improve people's diets (76). The strongest factors in food choice were income and proximity to fast-food restaurants.
Pricing strategies include enhanced usability of the SNAP, WIC, and EBT at healthier food vendors, working with grocers in placement and pricing of healthier foods, and consolidated bid purchase by large organizations such as school districts, large worksites, and local governments. Consolidated bids allow large purchasers to buy healthier foods at a reduced price passing the savings onto the consumer. A number of communities are working to enhance the use of SNAP/EBT cards at healthier vendors including farmers markets and convenience stores. There are various models for this intervention, for example the policy in which consumers who purchase $3 of fruits and vegetables receive two additional dollars in “bonus bucks” for the purchase of additional fruits and vegetables. While such strategies seem quite promising, their impact (particularly long term) in relation to health disparities has not been fully evaluated. Despite the common perception that farmers markets are not viable for low income populations due to their costs, little research has been conducted comparing costs between supermarkets and farmers markets (77).
The implementation of food policies, particularly those that are jurisdiction-wide, should be an effective strategy to reducing disparities in health. These policy approaches should align with health equity since the entire population is covered by the intervention. Unfortunately, a jurisdiction-wide approach could inadvertently exacerbate health disparities if differential barriers exist in the adoption, implementation, and enforcement of the policy by the community or a sub-population. For example, in 1988 the US Food and Drug Administration required the fortification of enriched cereal grain products with folic acid and manufacturers voluntarily added folate to many ready-to-eat cereals. This strategy was extremely effective in increasing folate levels for women of childbearing age, greatly reducing the rate of neural tube defects in the US (78). Unfortunately, because of differential access to folate-rich foods, racial and ethnic disparities in folate remain (78, 79). Integrating a health disparities assessment into policy planning and implementation can help to ensure that the implementation of policies lessen, and not widen, health disparities. This includes the development of milestones that are specifically aimed at advancing health equity, targeting efforts to sub-populations experiencing greater burden, working with organizations and in settings to reach underserved populations, and by addressing barriers to and potential unintended consequences of policy strategies. While some policy approaches may seem promising for addressing health inequities, they may be insufficient in practice without strategic actions to alleviate barriers that sub-populations face in terms of the implementation, enforcement, and sustainability as well as any unintended consequences of the policy.
Conclusions
These three examples illustrate that epidemiologists working in the area of health disparities are faced with a number of dilemmas. First, the complexity of the topic often demands innovation in methodological and statistical approaches, including the collection or identification of data not typically encountered in the academic formation of epidemiologists. Qualitative data may often be necessary to help understand the culture and context in which the disease or risk factor occurs in order to determine who and what to include in surveillance activities. As an example, in the early history of the HIV/AIDS epidemic it was thought that categories of people, rather than their behaviors, were the sources of risk. In this way, gay men and Haitians were identified as targets of surveillance, but only later were the risk behaviors described (e.g., men having sex with men, injection drug use), as well as their social patterning. Nuanced approaches of interviewing and studying cultural group norms and behaviors helped epidemiologists to eventually ask better questions in order to determine and provide guidance on how to reduce risk of infection. It was also in those qualitative approaches that quantitative questions were included in surveillance, leading to further insights about the socially patterned differences in HIV incidence by race/ethnicity, gender and sexual orientation (37, 80).
Health disparities researchers face unique challenges in the translation of their findings into policy, since interventions often involve changes outside the health care enterprise, including redistribution of resources, affirmative action programs or opposition to actions that foster social inequality. Epidemiologists, like other health professionals, have traditionally avoided explicit connections between their scientific findings and social justice motivations of that work (35, 37). This determination to engage in value free science and let others determine how best to apply the findings of epidemiologic research to policy is a long-standing value within the discipline, and the source of much tension in the application of epidemiology to the study of disparities.
Health inequalities of interest from a policy perspective are those differences in health that are judged unnecessary, preventable, and unjust (33, 35). Yet the obvious consequence of such a definition is that these classifications cannot be based on “scientific” evidence alone. Ideology, values, and political perspectives are all necessarily part of the process of determining these classifications. It is therefore naive to imagine that epidemiologists can avoid subjectivity in the conduct and interpretation of their work, even while as scientists they strive to provide the best evidence-based knowledge for effective policy development.
Spasoff (1999) suggested that policy development has five key steps and that epidemiologic data are central as a guide in each of those steps (81). The first step is the assessment of population health, in which the role of epidemiology is to define the population and to use surveillance to identify trends and patterns and to assess risks and health needs. While the field has demonstrated important contributions to this first step, it has done less to follow up with the remaining steps which involve producing evidence for successful health equity interventions. To some extent, this may result from a greater emphasis on individual level risk factor identification versus evaluation of intervention programs (35, 81). Research on risk factors may lead more naturally to intervention opportunities if studied from the perspective of population level factors, particularly as they occur within specific environments or socially patterned risk clusters and vulnerable sub-populations (82-85).
Epidemiologists bring a set of methodological and analytic skills to the last three cycles in policy development: policy choices, policy implementation and policy evaluation (81). Assessing potential interventions often requires synthesizing and evaluating evidence across diverse applications and study designs. Though epidemiologists are often trained in conducting systematic reviews, they are sometimes less prepared for the type of evaluation necessary to identify cost effective and efficacious policy interventions. They must embrace evaluation and dissemination at the beginning of the planning process, and seek funding to support these tasks. Funders also should consider the need to support all phases of health disparities research.
Box 1. Five key steps of the policy cycle.
Assessment of population health
Assessment of potential interventions
Policy choices
Policy implementation
Policy evaluation
Acknowledgments
We gratefully acknowledge comments from participants of the April 2011 American College of Epidemiology policy committee meeting in St. Louis, Missouri, as well as suggestions of topics for potential cases from health disparities researchers in response to our queries. We also acknowledge funding support from the American College of Epidemiology and Washington University in St. Louis (Division of Public Health Sciences) for the April 2011 meeting, and from NIH DA 20826 (Mays) and CDC cooperative agreement 1 U48 DP001929 (Carter-Pokras) for participation in preparation of this manuscript. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
List of Abbreviations and Acronyms
- AIDS
Acquired Immune Deficiency Syndrome
- CARDIA
Coronary Artery Risk Development in Young Adults Study
- CBOs
Community Based Organizations
- CDC
Centers for Disease Control and Prevention
- DALYs
Disability Adjusted Life-Years
- EBT
Electronic Benefit Transfer
- HIV
Human Immunodeficiency Virus
- HHS
United States Department of Health and Human Services
- LA
Los Angeles
- ng/mL
Nanograms per milliter
- RBC
Red Blood Cells
- REACH
Racial and Ethnic Approaches to Community Health program
- QALYs
Quality Adjusted Life-Years
- SES
Socioeconomic status
- SNAP
Supplemental Nutrition Assistance Program
- US
United States
- WIC
Women, Infants and Children
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Brownson RC, Hartge P, Samet JM, Ness RB. From epidemiology to policy: toward more effective practice. Ann Epidemiol. 2010 Jun;20(6):409–411. doi: 10.1016/j.annepidem.2010.03.003. [DOI] [PubMed] [Google Scholar]
- 2.United States Census Bureau Population Division. Population Projections. U.S. Interim Projections by Age, Sex, Race, and Hispanic Origin:2000-2050 [Google Scholar]
- 3.Ruffin J. The science of eliminating health disparities: Embracing a new paradigm. Am J Public Health. 2010 Apr 1;100(1):S8–9. doi: 10.2105/AJPH.2010.191957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Malone TE, Task Force Members Report of the Secretary's Task Force on Black & Minority Health. [Accessed on April 5, 2012];1985 Available at http://minorityhealth.hhs.gov/assets/pdf/checked/1/ANDERSON.pdf.
- 5.Centers for Disease Control and Prevention. Publications and Information Products Health, United States, annual report on trends in health statistics. [Accessed on April 5, 2012]; Available at http://www.cdc.gov/nchs/hus.htm.
- 6.U.S. Department of Health & Human Services. Agency for Healthcare Research and Quality 2010 National Healthcare Quality & Disparities Reports. [Accessed on April 5, 2012]; Available at http://www.ahrq.gov/qual/qrdr10.htm.
- 7.U.S. Department of Health & Human Services. The Office of Minority Health. [Accessed on April 5, 2012]; Available at http://minorityhealth.hhs.gov/
- 8.Clinton B. One America in the 21st Century: The President's Initiative on Race. [Accessed on April 5, 2012];1998 Mar; Available at https://www.ncjrs.gov/pdffiles/173431.pdf.
- 9.U.S. Department of Health & Human Services. Healthy People 2020. [Accessed on April 5, 2012]; Available at http://healthypeople.gov/2020/default.aspx.
- 10.U.S. Department of Health & Human Services. National Partnership for Action to End Health Disparities. HHS Action Plan to Reduce Racial and Ethnic Health Disparities. [Accessed on April 5, 2012]; Available at http://www.minorityhealth.hhs.gov/npa/files/Plans/HHS/HHS_Plan_complete.pdf.
- 11.Office of Management and Budget. Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. 1997;62:58781–58790. Federal Register. [Google Scholar]
- 12.Weed DL. Science, ethics guidelines, and advocacy in epidemiology. Ann Epidemiol. 1994 Mar;4(2):166–71. doi: 10.1016/1047-2797(94)90064-7. [DOI] [PubMed] [Google Scholar]
- 13.Thomas SB, Quinn SC, Butler J, Fryer CS, Garza MA. Toward a fourth generation of disparities research to achieve health equity. Annu Rev Public Health. 2011 Apr 21;32:399–416. doi: 10.1146/annurev-publhealth-031210-101136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Airhihenbuwa CO, Laveist TA. Racial and ethnic approaches to community health (REACH) 2010. Health Promot Pract. 2006;7(3 Suppl):174S–5S. doi: 10.1177/1524839906288671. [DOI] [PubMed] [Google Scholar]
- 15.Matyas ML, Haley-Oliphant AE, editors. Women Life Scientists: Past, Present, and Future-Connecting Role Models to the Classroom Curriculum. The American Physiological Society; 1997. [Google Scholar]
- 16.Bollet A. Politics and pellagra: the epidemic of pellagra in the U.S. in the early twentieth century. Yale J Biol Med. 1992;65(3):211–21. [PMC free article] [PubMed] [Google Scholar]
- 17.Cohen DA, Scribner RA, Farley TA. A structural model of health behavior: a pragmatic approach to explain and influence health behaviors at the population level. Prev Med. 2000 Feb;30(2):146–54. doi: 10.1006/pmed.1999.0609. [DOI] [PubMed] [Google Scholar]
- 18.Slater SJ, Nicholson L, Chriqui J, Turner L, Chaloupka F. The Impact of State Laws and District Policies on Physical Education and Recess Practices in a Nationally Representative Sample of US Public Elementary Schools. Archives of Pediatrics & Adolescent Medicine. 2011 doi: 10.1001/archpediatrics.2011.1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Story M, Nanney MS, Schwartz MB. Schools and obesity prevention: creating school environments and policies to promote healthy eating and physical activity. Milbank Q. 2009 Mar;87(1):71–100. doi: 10.1111/j.1468-0009.2009.00548.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Joffe M, Mindell J. Complex Causal Process Diagrams for Analyzing the Health Impacts of Policy Interventions. Am J Public Health. 2006;96(3):473–9. doi: 10.2105/AJPH.2005.063693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Task Force on Community Preventive Services. Recommendations from the Task Force on Community Preventive Services to decrease asthma morbidity through home-based, multi-trigger, multicomponent interventions. Am J Prev Med. 2011;41(2S1):S1–4. doi: 10.1016/j.amepre.2011.04.011. [DOI] [PubMed] [Google Scholar]
- 22.Jacobs DE, Brown MJ, Baeder A, Sucosky MS, Margolis S, Hershovitz J, Kolb L, Morley RL. A Systematic Review of Housing Interventions and Health: Introduction, Methods, and Summary Findings. J Public Health Management Practice. 2010;16(5) E-Supp:S5–S10. doi: 10.1097/PHH.0b013e3181e31d09. [DOI] [PubMed] [Google Scholar]
- 23.Oakes JM, Kaufman JS. Methods in Social Epidemiology. San Francisco, CA: Jossey-Bass; 2006. [Google Scholar]
- 24.Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. 1999 Jan;10(1):37–48. [PubMed] [Google Scholar]
- 25.Glymour MM, Greenland S. Causal diagrams. In: Rothman KJ, Greenland S, Lash TL, editors. Modern Epidemiology. 3rd. Philadelphia PA: Lippincott Williams & Wilkins; pp. 2008pp. 183–209. [Google Scholar]
- 26.Tzivian L. Outdoor air pollution and asthma in children. J Asthma. 2011 Jun;48(5):470–81. doi: 10.3109/02770903.2011.570407. [DOI] [PubMed] [Google Scholar]
- 27.Johnston SL, Pattemore PK, Sanderson G, Smith S, Lampe F, Josephs L, et al. Community study of role of viral infections in exacerbations of asthma in 9–11 year old children. BMJ. 1995;310(6989):1225–9. doi: 10.1136/bmj.310.6989.1225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Krieger J, Jacobs DE, Ashley PJ, Baeder A, Chew GL, Dearborn D, Hynes HP, et al. Housing interventions and control of asthma-related indoor biologic agents: a review of the evidence. J Public Health Manag Pract. 2010 Sep-Oct;16(5 Suppl):S11–20. doi: 10.1097/PHH.0b013e3181ddcbd9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Reisman RE, Mauriello PM, Davis GB, Georgitis JW, Demasi JM. A double-blind-study of the effectiveness of a highefficiency particulate air (HEPA) filter in the treatment of patients with perennial allergic rhinitis and asthma. J Allergy Clin Immunol. 1990;85(6):1050–1057. doi: 10.1016/0091-6749(90)90050-e. [DOI] [PubMed] [Google Scholar]
- 30.Greenland S. Ch. 22: Overthrowing the Tyranny of Null Hypotheses Hidden in Causal Diagrams. In: Dechter R, Geffner H, Halpern JY, editors. Heuristics, Probabilities, and Causality: A Tribute to Judea Pearl. College Publications; pp. 2010pp. 365–382. [Google Scholar]
- 31.Meyer BD. Natural and Quasi-Experiments in Economics. Journal of Business & Economic Statistics. 1995;13(2):151–161. [Google Scholar]
- 32.Prieto L, Sacristán JA. Problems and solutions in calculating quality-adjusted life years (QALYs) [Accessed on April 5, 2012];Health Qual Life Outcomes. 2003 Dec 19;1(80) doi: 10.1186/1477-7525-1-80. Available from: http://www.hqlo.com/content/pdf/1477-7525-1-80.pdf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Carter-Pokras O, Baquet C. What is a health disparity? Public Health Reports. 2002;117:426–432. doi: 10.1093/phr/117.5.426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Keppel K, Pamuk E, Lynch J, Carter-Pokras O, Kim I, Mays V, Pearcy J, Schoenbach V, Weissman JS. Methodological Issues in Measuring Health Disparities. National Center for Health Statistics. Vital Health Stat. 2005;2(141) [PMC free article] [PubMed] [Google Scholar]
- 35.Braveman P. Health disparities and health equity: Concepts and measurement. Annu Rev Public Health. 2006;27:167–94. doi: 10.1146/annurev.publhealth.27.021405.102103. [DOI] [PubMed] [Google Scholar]
- 36.Harper S, King NB, Meersman SC, Reichman ME, Breen N, Lynch J. Implicit value judgments in the measurement of health inequalities. Milbank Q. 2010;88(1):4–29. doi: 10.1111/j.1468-0009.2010.00587.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.James SA. Epidemiologic research on health disparities: Some thoughts on history and current developments. Epidemiol Rev. 2009;31(1):1–6. doi: 10.1093/epirev/mxp010. [DOI] [PubMed] [Google Scholar]
- 38.Harper S, Lynch J, Meersman SC, Breen N, Davis WW, Reichman ME. An overview of methods for monitoring social disparities in cancer with an example using trends in lung cancer incidence by area-socioeconomic position and race-ethnicity, 1992-2004. Am J Epidemiol. 2008;167(8):889–99. doi: 10.1093/aje/kwn016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Messer LC. Measuring social disparities in health--what was the question again? Am J Epidemiol. 2008;167(8):900–4. doi: 10.1093/aje/kwn019. [DOI] [PubMed] [Google Scholar]
- 40.Scanlan JP. Can we actually measure health disparities? Chance. 2006;19(2):47–51. [Google Scholar]
- 41.Krieger N, Williams DR. Changing to the 2000 standard million: are declining racial/ethnic and socioeconomic inequalities in health real progress or statistical illusion? Am J Public Health. 2001 Aug;91(8):1209–13. doi: 10.2105/ajph.91.8.1209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Sebelius K. Washington DC: Department of Health and Human Services; 2011. Sept. [Accessed on April 5, 2012]. Report to Congress. Approaches for Identifying, Collecting, and Evaluating Data on Health Care Disparities in Medicaid and CHIP. Available from: http://www.healthcare.gov/law/resources/reports/index.html. [Google Scholar]
- 43.HHS Office of Minority Health; Final Data Collection Standards for Race, Ethnicity, Primary Language, Sex, and Disability Status Required by Section 4302 of the Affordable Care Act. US Department of Health and Human Services. [Accessed on April 5, 2012];2011 Available: http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlid=208.
- 44.HHS Office of Minority Health; Plan for Health Data Collection on Lesbian, Gay, Bisexual and Transgender (LGBT) Populations. US Department of Health and Human Services. [Accessed on April 5, 2012];2011 Available: http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlid=208.
- 45.Committee on Leading Health Indicators For Healthy People 2020. Leading Health Indicators For Healthy People 2020: Letter Report. National Academics Press: Washington, DC; 2010. [Google Scholar]
- 46.Salsbury B, O'Keefe E, Kertanis J. Chapter 23. Measuring Social Determinants of Health Inequities: The CADH Health Equity Index. In: Hofrichter R, Bhatia R, editors. Tackling Health Inequities through Public Health Practice: Theory to Action. New York, NY: Oxford University Press; 2010. [Google Scholar]
- 47.Whakapuakanga: Ministry of Social Development. Ministry of Social Development; New Zealand: 2010. [Accessed on April 5, 2012]. 2010 The Social Report–Te Purongo Oranga Tangata. Available at: http://www.communityresearch.org.nz/wp-content/uploads/tdomf/4097/the-social-report-2010.pdf. [Google Scholar]
- 48.Bloom B, Cohen RA, Freeman G. Summary health statistics for U.S. children: National Health Interview Survey, 2009. Vital Health Stat. 2010 Dec;10(247):1–82. [PubMed] [Google Scholar]
- 49.Digenis-Bury EC, Brooks DR, Chen L, Ostrem M, Horsburgh CR. Use of a population-based survey to describe the health of Boston public housing residents. Am J Public Health. 2008 Jan;98(1):85–91. doi: 10.2105/AJPH.2006.094912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Northridge J, Ramirez OF, Stingone JA, Claudio L. The role of housing type and housing quality in urban children with asthma. J Urban Health. 2010 Mar;87(2):211–24. doi: 10.1007/s11524-009-9404-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Krieger JW, Takaro TK, Rabkin JC. Chapter 19. Breathing easier in Seattle: addressing asthma disparities through healthier housing. In: Williams RA, editor. Healthcare Disparities at the Crossroads with Healthcare Reform. Springer: 2011. pp. 359–385. [Google Scholar]
- 52.Guide to Community Preventive Services. Asthma control: home-based multi-trigger, multicomponent interventions. www.thecommunityguide.org/asthma/multicomponent.html. Last updated: 11/17/2011.
- 53.Krieger JW, Song L, Takaro TK, Stout J. Asthma and the home environment of low-income urban children: preliminary findings from the Seattle-King County healthy homes project. Urban Health. 2000 Mar;77(1):50–67. doi: 10.1007/BF02350962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Krieger JW, Takaro TK, Song L, Weaver M. The Seattle-King County Healthy Homes Project: a randomized, controlled trial of a community health worker intervention to decrease exposure to indoor asthma triggers. Am J Public Health. 2005 Apr;95(4):652–9. doi: 10.2105/AJPH.2004.042994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Krieger JW, Takaro TK, Rabkin JC. Chapter 15. Breathe easy in Seattle: addressing asthma disparities through healthier housing. In: Williams RA, editor. Eliminating healthcare disparities in America. Totowa, NJ: Humana Press; 2007. pp. 313–339. [Google Scholar]
- 56.Margellos-Anast H, Gutierrez MA. Chapter 11. Pediatric asthma in black and Latino Chicago communities: local level data drives response. In: Whitman S, Shah AM, Benjamins MR, editors. Urban Health: combating disparities with local data. New York, NY: Oxford University Press; 2011. [Google Scholar]
- 57.Parker EA, Israel BA, Robins TG, Mentz G, Lin X, Brakefield-Caldwell W, et al. Evaluation of community action against asthma: a community health worker intervention to improve children's asthma-related health by reducing household environmental triggers of asthma. Health Education and Behavior. 2008;35(3):376–395. doi: 10.1177/1090198106290622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Spielman SE, Golembeski CA, Northridge ME, Vaughan RD, Swaner R, Jean-Louis B, et al. Interdisciplinary planning for healthier communities: findings from the Harlen Children's Zone Asthma Initiative. Journal of the American Planning Association. 2006;73:100–108. [Google Scholar]
- 59.Whitman S, Shah AM, Benjamins MR. Chapter 1. Introducing the Sinai model for reducing health disparities and improving health. In: Whitman S, Shah AM, Benjamins MR, editors. Urban Health: combating disparities with local data. New York, NY: Oxford University Press; 2011. [Google Scholar]
- 60.Saegert SC, Klitzman S, Freudenberg N, Cooperman-Mroczek J, Nassar S. Healthy Housing: A Structured Review of Published Evaluations of US Interventions to Improve Health by Modifying Housing in the United States, 1990–2001. Am J Public Health. 2003;93(9):1471–1477. doi: 10.2105/ajph.93.9.1471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.National Center for Healthy Housing. Housing Interventions and Health: A Review of the Evidence. 2009 [Google Scholar]
- 62.Krieger JK, Takaro TK, Allen C, Song L, Weaver M, Chai S, Dickey P. The Seattle-King County healthy homes project: implementation of a comprehensive approach to improving indoor environmental quality for low-income children with asthma. Environ Health Perspect. 2001 Apr;110(2):311–22. doi: 10.1289/ehp.02110s2311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Gøtzsche PC, Johansen HK. House dust mite control measures for asthma. Cochrane Database Syst Rev. 2008;(2) doi: 10.1002/14651858.cd001187.pub3. Art. No.: cd001187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Sauni R, Uitti J, Jauhiainen M, Kreiss K, Sigsgaard T, Verbeek JH. Remediating buildings damaged by dampness and mould for preventing or reducing respiratory tract symptoms, infections and asthma. Cochrane Database Syst Rev. 2011 Sep 7;9:CD007897. doi: 10.1002/14651858.CD007897.pub2. [DOI] [PubMed] [Google Scholar]
- 65.Jacobs DE, Brown MJ, Baeder A, et al. A systematic review of housing interventions and health: introduction, methods, and summary findings. J Public Health Management Practice. 2010;16(5) E-Supp:S5, S10. doi: 10.1097/PHH.0b013e3181e31d09. [DOI] [PubMed] [Google Scholar]
- 66.Krieger J, Jacobs DE, Ashley P, Peter J, et al. Housing Interventions and Control of Asthma-Related Indoor Biologic Agents: A Review of the Evidence. Journal of Public Health Management & Practice. 2010;16(5):S11–S20. doi: 10.1097/PHH.0b013e3181ddcbd9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Takaro TK, Krieger J, Song L, Sharify D, Beaudet N. The Breathe-Easy Home: the impact of asthma-friendly home construction on clinical outcomes and trigger exposure. Am J Public Health. 2011 Jan;101(1):55–62. doi: 10.2105/AJPH.2010.300008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Carter-Pokras OD, Spirtas R, Bethune L, Mays V, Freeman VL, Cozier YC. The training of epidemiologists and diversity in epidemiology: findings from the 2006 Congress of Epidemiology survey. Annals of epidemiology. 2009;19(4):268–75. doi: 10.1016/j.annepidem.2009.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Giang T, Karpyn A, Laurison HB, Hillier A, Perry RD. Closing the grocery gap in underserved communities: the creation of the Pennsylvania Fresh Food Financing Initiative. J Public Health Manag Pract. 2008 May-Jun;14(3):272–9. doi: 10.1097/01.PHH.0000316486.57512.bf. [DOI] [PubMed] [Google Scholar]
- 70.Bassford N, Galloway-Gilliam L, Flynn G CHC Food Resource Development Workgroup. Food Desert to Food Oasis: Promoting Grocery Store Development in South Los Angeles. Community Health Councils, Inc.; Los Angeles, CA: 2010. [Accessed on April 16, 2012]. Available at: http://www.chc-inc.org/downloads/Food%20Desert%20to%20Food%20Oasis%20July%202010.pdf. [Google Scholar]
- 71.Plescia M, Herrick H, Chavis L. Improving health behaviors in an African American Community: The Charlotte Racial and Ethnic Approaches to Community Health Project. Am J Public Health. 2008;98(9):1678–1684. doi: 10.2105/AJPH.2007.125062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Community Health Councils. Los Angeles, CA: Community Health Councils; 2008. Apr 8, [Accessed on April 5, 2012]. Does race define what's in the shopping cart. Available from: http://www.chc-inc.org/section.php?id=22. [Google Scholar]
- 73.Helmer J. South L.A. Fights Food Deserts: South Los Angeles has begun to say bye-bye to burgers and fries through its ordinance to limit fast-food restaurants. [Accessed on April 5, 2012];Urban Farm Online.Com. 2011 Mar 1; Available: http://www.urbanfarmonline.com/urban-farm-news/2011/03/01/south-la-fights-food-deserts.aspx.
- 74.MacVean M, South LA. South L.A. gets a new supermarket. [Accessed on April 5, 2012];Los Angeles Times. 2010 Feb 24; Available: http://latimesblogs.latimes.com/dailydish/2010/02/south-la-gets-a-new-supermarket.html.
- 75.Strum R, Cohen D. Zoning for Health? The Year-Old Ban on New Fast-Food Restaurants in South LA: The Ordinance Isn't a Promising Approach to Attacking Obesity. Health Affairs. 2009;28(6):1088–1097. doi: 10.1377/hlthaff.28.6.w1088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Boone-Heinonen J, Gordon-Larsen P, Kiefe CI, Shikany JM, Lewis CE, Popkin BM. Fast food restaurants and food stores: longitudinal associations with diet in young to middle-aged adults: the CARDIA study. Arch Intern Med. 2011 Jul 11;171(13):1162–70. doi: 10.1001/archinternmed.2011.283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Briggs S, Fisher A, Lott M, Miller S, Tessman N. Real Food, Real Choice: Connecting Snap Recipients with Farmers Markets. Community Food Security Coalition | Farmers Market Coalition. 2010 Jun; [Google Scholar]
- 78.Erickson JD, Mulinare J, Yang Q, et al. Folate status in women of childbearing age, by race/ethnicity—United States, 1999-2000. MMWR. 2002;51(36):808–810. [PubMed] [Google Scholar]
- 79.Cordero A, Mulinare J, Boyle C, Dietz W, Johnston R, Jr, Leighton J, Popovic T. CDC Grand Rounds: Additional Opportunities to Prevent Neural Tube Defects with Folic Acid Fortification. MMWR. 2010 Aug 13;59(31):980–984. [PubMed] [Google Scholar]
- 80.Mays VM, Maas R, Ricks J, Cochran SD. HIV and African American Women in the South: Employing A Population-Level HIV Prevention and Intervention Efforts. In: Baum A, Revenson R, Singer J, editors. Handbook of Health Psychology. New York: Oxford Press; 2011. pp. 771–801. [Google Scholar]
- 81.Spasoff RA. Epidemiologic Methods for Health Policy. New York, NY: Oxford University Press; 1999. [Google Scholar]
- 82.Farley TA. Sexually transmitted diseases in the Southeastern United States: location, race, and social context. Sex Transm Dis. 2006 Jul;33(7 Suppl):S58–64. doi: 10.1097/01.olq.0000175378.20009.5a. [DOI] [PubMed] [Google Scholar]
- 83.Mays V, Maas R, Ricks J, Cochran SD. HIV in African American Women: A Social Determinants Approach in Population-Level HIV Prevention Intervention. In: Baum A, Revenson TA, Singer J, editors. A Handbook of Health Psychology. 2nd. Florence, KY: Psychology Press; 2011. [Google Scholar]
- 84.Rhodes T. Risk environments and drug harms: a social science for harm reduction approach. Int J Drug Policy. 2009 May;20(3):193–201. doi: 10.1016/j.drugpo.2008.10.003. Epub 2009 Jan 14. [DOI] [PubMed] [Google Scholar]
- 85.Rhodes T, Stimson GV, Crofts N, Ball A, Dehne K, Khodakevich L. Drug injecting, rapid HIV spread, and the ‘risk environment’: implications for assessment and response. AIDS. 1999;13(A):S259–69. [PubMed] [Google Scholar]