

Abstract
Objective
To evaluate the relationship between anthropometric measurements and renal length and volume measured with ultrasound in Korean children who have morphologically normal kidneys, and to create simple equations to estimate the renal sizes using the anthropometric measurements.
Materials and Methods
We examined 794 Korean children under 18 years of age including a total of 394 boys and 400 girls without renal problems. The maximum renal length (L) (cm), orthogonal anterior-posterior diameter (D) (cm) and width (W) (cm) of each kidney were measured on ultrasound. Kidney volume was calculated as 0.523 × L × D × W (cm3). Anthropometric indices including height (cm), weight (kg) and body mass index (m2/kg) were collected through a medical record review. We used linear regression analysis to create simple equations to estimate the renal length and the volume with those anthropometric indices that were mostly correlated with the US-measured renal sizes.
Results
Renal length showed the strongest significant correlation with patient height (R2, 0.874 and 0.875 for the right and left kidneys, respectively, p < 0.001). Renal volume showed the strongest significant correlation with patient weight (R2, 0.842 and 0.854 for the right and left kidneys, respectively, p < 0.001). The following equations were developed to describe these relationships with an estimated 95% range of renal length and volume (R2, 0.826-0.884, p < 0.001): renal length = 2.383 + 0.045 × Height (± 1.135) and = 2.374 + 0.047 × Height (± 1.173) for the right and left kidneys, respectively; and renal volume = 7.941 + 1.246 × Weight (± 15.920) and = 7.303 + 1.532 × Weight (± 18.704) for the right and left kidneys, respectively.
Conclusion
Scatter plots between height and renal length and between weight and renal volume have been established from Korean children and simple equations between them have been developed for use in clinical practice.
Keywords: Kidney, Organ size, Body size, Ultrasonography, Child
INTRODUCTION
Childhood is an important period of growth for many organ systems. Among various growth parameters, kidney size is an important parameter used for the clinical evaluation of renal growth and renal abnormalities, including atrophy, hypoplasia, and hypertrophy in children. Therefore, having a reliable reference for kidney size in children is valuable.
Several studies suggest that kidney length and volume are strongly correlated with a patient's height, weight and body mass index (BMI) (1, 2). The prevalence of obesity has increased within children globally over the past decade, and this issue has raised concerns for health of the pediatric population. Recent studies in Korea have also reported that the prevalence of obesity among children increased from 5.8% in 1997 to 9.7% in 2005 according to the definition of obesity as being at or above the 95th percentile of the gender-specific BMI for age in the 2007 Korean National Growth Charts or a BMI of 25 or higher (3, 4). Therefore, it is important to establish an up-to-date reference for kidney size in the pediatric population with consideration of the recent increase in average height, weight, and BMI.
There are several methods for measuring renal sizes, including abdominal CT and MRI. However, these approaches have disadvantages such as radiation exposures and high costs. In comparison, ultrasonography (US) is a safe and simple method for evaluating renal length and volume. However, previous studies have only shown the normal range of renal size through a graph, which is somewhat difficult to apply clinically (5, 6). The purpose of this study was to evaluate the relationship of height, weight and BMI with renal length and volume measured with US in Korean children who have morphologically normal kidneys. In addition, we attempted to develop simple equations to estimate the renal sizes using the anthropometric measurements.
MATERIALS AND METHODS
The institutional review board of our hospital approved this retrospective study and informed consent was waived. We reviewed US images of pediatric patients under 18 years of age who were referred to our health system from November 2009 to August 2010 for routine care or follow-up examinations. Patients underwent neither preparations nor sedations for the US examinations.
Ultrasonography was performed using an iU22 ultrasound unit (Philips Ultrasound, Bothell, WA, USA) with a 5-8 or 1-5 MHz convex transducer by two pediatric radiologists with 27 and 9 years of experience for pediatric US, respectively. Renal length (L) (cm) and width (W) (cm) were routinely measured during abdominal US in our institution. The orthogonal anterior-posterior diameter (cm) of each kidney was measured retrospectively by one pediatric radiologist with 9 years of experience for pediatric US. These data were obtained in the sagittal and axial planes passing through the renal hilum with patients in the supine or slightly left or right lateral decubitus positions. Kidney volume was calculated in cubic centimeters using the equation for an ellipsoid: volume (cm3) = mean length (L) × mean width (W) × mean depth (D) × 0.523.
Exclusion criteria included any congenital renal anomaly or renal disease that affects US renal size measurement, such as renal agenesis or the horseshoe kidney. Patients with abnormal ultrasound imaging of the kidney, such as cortical scarring, increased echogenicity, pelvic dilatation, renal cysts and other abnormal findings in the urinary bladder or urinary tract, were also excluded. Patients with hematuria or proteinuria within 6 months after US examination or pyuria within 1 month before and after US study in urinalysis were also excluded. If the patient had a systemic disease such as a hematologic, oncologic or endocrine disease that could affect height, weight, BMI and abdominal organ growth, they were also excluded. The most common indication of the US examinations in the enrolled group was the evaluation of fever except from the urinary tract infection. Routine health screening was the second largest cause. Abdominal pain unrelated to renal problems and evaluation of benign mass such as hepatic cyst or hemangioma were followed as reasons for US examinations.
Age, gender, height and weight were collected by reviewing the medical records for each patient. Height (cm) and weight (kg) were measured on the day of US study. BMI was calculated as weight (kg)/height (m2). Obesity was defined as BMI with age which was more than 95 percentiles or 25 kg/m2 according to a previous study (7). Statistical analyses were performed using the Statistical Analysis System version 9.2 (SAS Institute Inc., Cary, NC, USA). Paired t test was used to compare the length and volume of bilateral kidneys. Simple and multiple linear regression analyses were applied to evaluate the relationship between the anthropometric parameters and the renal length or volume. We also used the linear regression analysis to create simple equations to estimate the renal length and volume with anthropometric indices that were correlated to the US-measured renal sizes. Results were considered statistically significant if the p-value was < 0.05 for all data analyses.
RESULTS
A total of 794 Korean children, 394 boys and 400 girls, were included in this study. Ages ranged from 0 to 18 years with a mean of 4.6 ± 4.6 years. The average height of the enrolled group was 100.5 ± 33.8 cm (range: 43-182) and the average weight was 19.4 ± 15.0 kg (range: 2.4-89). The average BMI was calculated as 16.7 ± 2.5 kg/m2 (range: 6.1-27.3). The overall percentage of obesity in the study population was 3.7% (29/794), and in school-age children aged 8-18 years, it increased to 7.5% (14/186). The left kidney was significantly larger than the right kidney in terms of both renal length (mean 7.06 vs. 6.89 cm; p < 0.001) and volume (mean 37.07 vs. 32.15 cm3, p < 0.001).
Tables 1-4 shows the relationship between each parameter and renal size on univariate and multivariate analyses. The lengths of both the right (R2 = 0.874) and the left (R2 = 0.875) kidneys showed the strongest correlation with patient height in the univariate analysis (Table 1). On the multivariate analysis, only height indicated significantly strong correlations of the univariate analysis with renal length, whereas weight and BMI showed inconsistent and/or weaker correlations (Table 2). The volume of both the left (R2 = 0.854) and the right (R2 = 0.842) kidneys showed the strongest correlation with patient's weight in the univariate analysis (Table 3). Both height and weight showed significant correlations with renal volume in the multivariate analysis, whereas BMI did not (Table 4).
Table 1.
Univariate Analysis of Relation between Renal Length and Age, Weight, Height or Body Mass Index (BMI) in Boys and Girls

Note.- All betas were significant as p-value < 0.001.
Table 4.
Multivariate Analysis of Relation between Renal Volume and Age, Weight, Height, Body Mass Index (BMI) or Gender
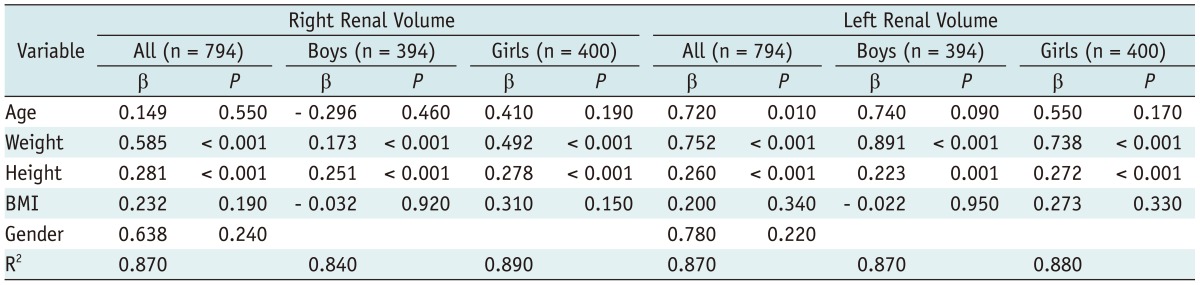
Table 2.
Multivariate Analysis of Relation between Renal Length and Age, Weight, Height, Body Mass Index (BMI) or Gender
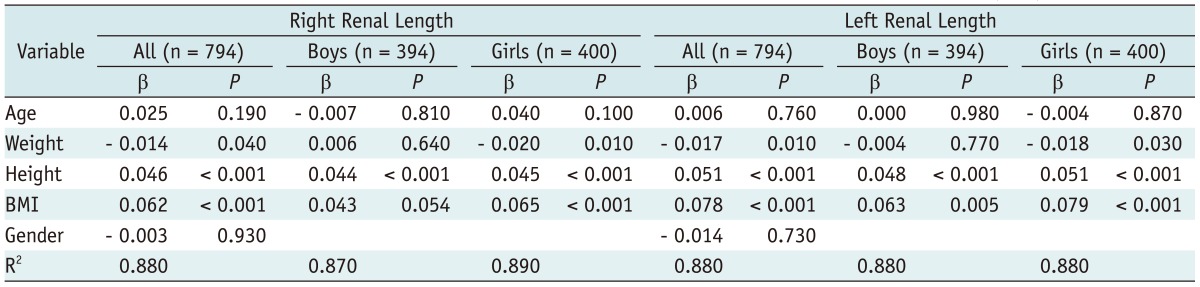
Table 3.
Univariate Analysis of Relation between Renal Volume and Age, Weight, Height or Body Mass Index (BMI) in Boys and girls

Note.- All betas were significant as p-value < 0.001.
Given the small, if any, effect of BMI on the renal sizes and robustness of height and weight as standalone independent variables, we developed simple univariate equations to estimate kidney length and volume using height and weight, respectively, as shown below including the estimated 95% confidence limit (R2 0.826-0.884, p < 0.001) (Figs. 1, 2).
Fig. 1.

Scatterplots and linear regression lines of height and renal length.
Graphs with simple equations for relationship between patient height and length of (A) right and (B) left kidneys including range for estimated 95% confidence limit.
Fig. 2.

Scatterplots and linear regression lines of weight and renal volume.
Graphs with simple equations for relationship between patient weight and volume of (A) right and (B) left kidneys including range for estimated 95% confidence limit.
Renal length (cm):
Boys: right = 2.270 + 0.046 × Height (± 1.200), left = 2.203 + 0.048 × Height (± 1.192)
Girls: right = 2.485 + 0.044 × Height (± 1.072), left = 2.528 + 0.045 × Height (± 1.152)
All groups: right = 2.383 + 0.045 × Height (± 1.135), left = 2.374 + 0.047 × Height (± 1.173)
Renal volume (cm3):
Boys: right = 6.408 + 1.324 × Weight (± 16.649), left = 5.349 + 1.632 × Weight (± 18.555)
Girls: right = 9.037 + 1.189 × Weight (± 15.047), left = 8.692 + 1.458 × Weight (± 18.657)
All groups: right = 7.941 + 1.246 × Weight (± 15.920), left = 7.303 + 1.532 × Weight (± 18.704)
DISCUSSION
There are many reports about US renal sizes and volumes and their relationships with body size (1, 2, 8, 9). To our knowledge, this study is one of the largest studies performed which evaluates the relationship between renal size and anthropometric indices. There were discrepancies in sizes between the left and the right kidney. In our study, the left kidney was significantly larger than the right kidney. This has also been shown in prior studies (5, 10). However, there are some studies that have demonstrated no significant differences between the left and right kidney size in children (11, 12).
It is well-known that renal size is related to age, height and weight. Many studies have shown that height correlates best with renal length (13, 14). Our study supports these prior results in that the bilateral kidney lengths show the strongest correlation with height. There is also a previous article which concludes that renal volume is closely related with body weight (13), and our results were consistent with this observation as well. In the univariate analysis, renal length shows the highest correlation with patient height and weight. Univariate equations were formulated by using simple linear regressions to estimate renal length and volume through respective body indices. The results of the univariate and multivariate analyses were also considered with the ease of use in clinical practices. Scatterplots were created, and they showed a close linear relationship between height and renal length and also between weight and renal volume.
There are also controversies regarding the correlation between gender and kidney size in children. Some studies suggest that girls have smaller kidneys (15, 16) and other studies indicate no differences in renal size between genders (17, 18). These differences may be due to the low statistical power of a small number of study groups. In our study, we made separate equations for renal size measurements for boys and girls. However, we suggest that the constants used in each equation are not remarkably different. Multivariate analysis also demonstrated that gender was not a significant independent factor on renal length and volume.
Body mass index is one of the widely-used parameters for measuring obesity. There have been several studies that evaluated body surface area and lean body mass as a predictor of renal size in children (14, 16). However, there are far fewer studies about the relationships between BMI and renal length and volume. Pantoja Zuzuárregui et al. (1) suggested that BMI is well-correlated with renal length. Interestingly, we found much weaker correlations between BMI and renal length or volume compared with that of height and weight. This suggests that BMI might not be a significant confounder in estimating the renal sizes. However, considering that the overall percentage of obese children in our study group was low, the effect of BMI might have diluted our study. Therefore, our study results may not be applicable to a population where obesity rate is higher and the effects of BMI may need to be further investigated.
Several prior articles have suggested nomograms for predicting renal size according to body height and weight (9, 13). Herein, we have proposed a simple equation with an estimated 95% normal range that demonstrates a linear relationship between the renal size and the body parameters for easy practice. We believe that this equation can be easily applied in clinical practices and can enable a quick assessment of normal kidney size in sonographic studies.
There are limitations to our study. First, it was a retrospective study of renal size even though renal length and width measurements were routinely performed by two pediatric radiologists. The second limitation is that we examined renal size only by US, which has indicated a relatively high intra- and inter-observer error with previous studies (19, 20). The difference in US techniques, patient positioning, and cursor placement can affect the reproducibility of measurements on renal length. Therefore, future prospective studies evaluating intra- and interobserver agreements are necessary. Moreover, Bakker et al. (21) proposed that renal volume acquired by US calculated with ellipsoid formula is not accurate, compared with renal volume acquired by MRI. Although only a small amount of patients were being compared. We think that the US assessment of renal volume is sufficient enough to obtain the normal range and to reveal relationships with body height and weight. Also, due to the need for sedation in CT or MRI, and the radiation exposure associated with CT, we prefer US evaluation in pediatric patients. However, this conclusion needs to be supported with future studies performed on a large number of patients especially in the comparison of renal volume acquired by US and MRI. The third limitation is that there were no evaluations of renal function measurements such as the serum creatinine level or glomerular filtration rate. We only evaluated sonographically normal kidneys and urinalysis for renal length and volume. However, renal function may be impaired in these morphologically normal kidneys. There have been several studies showing that renal function influences renal size (22, 23). Therefore, further study is also needed to analyze this relationship.
In conclusion, scatter plots between height and renal lengths and also between weight and renal volume were established among Korean children and simple equations between them were developed for use in clinical practice.
References
- 1.Pantoja Zuzuárregui JR, Mallios R, Murphy J. The effect of obesity on kidney length in a healthy pediatric population. Pediatr Nephrol. 2009;24:2023–2027. doi: 10.1007/s00467-009-1202-1. [DOI] [PubMed] [Google Scholar]
- 2.Glodny B, Unterholzner V, Taferner B, Hofmann KJ, Rehder P, Strasak A, et al. Normal kidney size and its influencing factors - a 64-slice MDCT study of 1.040 asymptomatic patients. BMC Urol. 2009;9:19. doi: 10.1186/1471-2490-9-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Oh K, Jang MJ, Lee NY, Moon JS, Lee CG, Yoo MH, et al. Prevalence and trends in obesity among Korean children and adolescents in 1997 and 2005. Korean J Pediatr. 2008;51:950–955. [Google Scholar]
- 4.Kim YS, Park MJ. Time trend in height, weight, BMI and waist circumference of Korean adolescents; from the Korean National Health and Nutrition Examination Survey (KNHNES), 1998, 2001 and 2005. J Korean Soc Pediatr Endocrinol. 2007;12:142–149. [Google Scholar]
- 5.Blane CE, Bookstein FL, DiPietro MA, Kelsch RC. Sonographic standards for normal infant kidney length. AJR Am J Roentgenol. 1985;145:1289–1291. doi: 10.2214/ajr.145.6.1289. [DOI] [PubMed] [Google Scholar]
- 6.Kadioglu A. Renal measurements, including length, parenchymal thickness, and medullary pyramid thickness, in healthy children: what are the normative ultrasound values? AJR Am J Roentgenol. 2010;194:509–515. doi: 10.2214/AJR.09.2986. [DOI] [PubMed] [Google Scholar]
- 7.Moon JS, Lee SY, Nam CM, Choi JM, Choe BK, Seo JW, et al. 2007 Korean National Growth Charts: review of developmental process and an outlook. Korean J Pediatr. 2008;51:1–25. [Google Scholar]
- 8.Luk WH, Lo AX, Au-Yeung AW, Liu KK, Woo YH, Chiang CC, et al. Renal length nomogram in Hong Kong Asian children: sonographic measurement and multivariable approach. J Paediatr Child Health. 2010;46:310–315. doi: 10.1111/j.1440-1754.2010.01714.x. [DOI] [PubMed] [Google Scholar]
- 9.Klare B, Geiselhardt B, Wesch H, Schärer K, Immich H, Willich E. Radiological kidney size in childhood. Pediatr Radiol. 1980;9:153–160. doi: 10.1007/BF01464310. [DOI] [PubMed] [Google Scholar]
- 10.Hederström E, Forsberg L. Kidney size in children assessed by ultrasonography and urography. Acta Radiol Diagn (Stockh) 1985;26:85–91. doi: 10.1177/028418518502600113. [DOI] [PubMed] [Google Scholar]
- 11.Han BK, Babcock DS. Sonographic measurements and appearance of normal kidneys in children. AJR Am J Roentgenol. 1985;145:611–616. doi: 10.2214/ajr.145.3.611. [DOI] [PubMed] [Google Scholar]
- 12.Holloway H, Jones TB, Robinson AE, Harpen MD, Wiseman HJ. Sonographic determination of renal volumes in normal neonates. Pediatr Radiol. 1983;13:212–214. doi: 10.1007/BF00973158. [DOI] [PubMed] [Google Scholar]
- 13.Dinkel E, Ertel M, Dittrich M, Peters H, Berres M, Schulte-Wissermann H. Kidney size in childhood. Sonographical growth charts for kidney length and volume. Pediatr Radiol. 1985;15:38–43. doi: 10.1007/BF02387851. [DOI] [PubMed] [Google Scholar]
- 14.Zerin JM, Blane CE. Sonographic assessment of renal length in children: a reappraisal. Pediatr Radiol. 1994;24:101–106. doi: 10.1007/BF02020164. [DOI] [PubMed] [Google Scholar]
- 15.Scott JE, Hunter EW, Lee RE, Matthews JN. Ultrasound measurement of renal size in newborn infants. Arch Dis Child. 1990;65(4 Spec No):361–364. doi: 10.1136/adc.65.4_spec_no.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Schmidt IM, Mølgaard C, Main KM, Michaelsen KF. Effect of gender and lean body mass on kidney size in healthy 10-year-old children. Pediatr Nephrol. 2001;16:366–370. doi: 10.1007/s004670100568. [DOI] [PubMed] [Google Scholar]
- 17.Chiara A, Chirico G, Barbarini M, De Vecchi E, Rondini G. Ultrasonic evaluation of kidney length in term and preterm infants. Eur J Pediatr. 1989;149:94–95. doi: 10.1007/BF01995855. [DOI] [PubMed] [Google Scholar]
- 18.Christophe C, Cantraine F, Bogaert C, Coussement C, Hanquinet S, Spehl M, et al. Ultrasound: a method for kidney size monitoring in children. Eur J Pediatr. 1986;145:532–538. doi: 10.1007/BF02429058. [DOI] [PubMed] [Google Scholar]
- 19.Sargent MA, Long G, Karmali M, Cheng SM. Interobserver variation in the sonographic estimation of renal volume in children. Pediatr Radiol. 1997;27:663–666. doi: 10.1007/s002470050207. [DOI] [PubMed] [Google Scholar]
- 20.Larson DB, Meyers ML, O'Hara SM. Reliability of renal length measurements made with ultrasound compared with measurements from helical CT multiplanar reformat images. AJR Am J Roentgenol. 2011;196:W592–W597. doi: 10.2214/AJR.10.5486. [DOI] [PubMed] [Google Scholar]
- 21.Bakker J, Olree M, Kaatee R, de Lange EE, Moons KG, Beutler JJ, et al. Renal volume measurements: accuracy and repeatability of US compared with that of MR imaging. Radiology. 1999;211:623–628. doi: 10.1148/radiology.211.3.r99jn19623. [DOI] [PubMed] [Google Scholar]
- 22.Sargent MA, Gupta SC. Sonographic measurement of relative renal volume in children: comparison with scintigraphic determination of relative renal function. AJR Am J Roentgenol. 1993;161:157–160. doi: 10.2214/ajr.161.1.8390789. [DOI] [PubMed] [Google Scholar]
- 23.Di Zazzo G, Stringini G, Matteucci MC, Muraca M, Malena S, Emma F. Serum creatinine levels are significantly influenced by renal size in the normal pediatric population. Clin J Am Soc Nephrol. 2011;6:107–113. doi: 10.2215/CJN.00580110. [DOI] [PMC free article] [PubMed] [Google Scholar]