

Abstract
Objective
Several prior investigations demonstrate an improvement in bone mineral density associated with use of TNF inhibitors (TNFi). We compared the risk of osteoporotic fractures among patients with rheumatoid arthritis (RA) initiating a disease-modifying antirheumatic drug (DMARD).
Methods
A population-based cohort study was conducted using health care utilization data (1996–2008) from a Canadian province and a US commercial insurance plan. Patients with at least two RA diagnoses were identified and follow-up began with the first prescription for a DMARD. Drug regimens were categorized into three mutually exclusive hierarchical groups: 1) TNFi with or without non-biologic DMARDs (nbDMARD), 2) methotrexate (MTX) without a TNFi, or 3) other nbDMARD without a TNFi or MTX. Main outcomes were hospitalizations for fractures of the hip, wrist, humerus, or pelvis based on diagnoses and procedure codes.
Results
The study cohort consisted of 16,412 RA patients with 25,988 new treatment episodes: 5,856 TNFi, 12,554 MTX, and 7,578 other nbDMARD. The incidence rate per 1,000 person-years for osteoporotic fracture were 5.11 (95% CI 3.50 – 7.45) for TNFi, 5.35 (95% CI 4.08–7.02) for MTX, and 6.38 (95% CI 3.78–10.77) for other nbDMARD. After multivariable adjustment for osteoporosis and fracture-related risk factors, the risk of non-vertebral osteoporotic fracture was not different in either TNFi (hazard ratio (HR) 1.07, 95% CI 0.57–1.98) or MTX (HR 1.18, 95% CI 0.60– 2.34) compared with nbDMARD.
Conclusion
Among subjects diagnosed with RA, the adjusted risk of non-vertebral fracture was similar across persons starting a TNFi, MTX, or other nbDMARD.
Keywords: rheumatoid arthritis, fracture, disease modifying antirheumatic drugs
INTRODUCTION
Rheumatoid arthritis (RA) is associated with an increased risk of osteoporosis and fractures.(1–3) A recent population-based cohort study reported that patients with RA had a 25% higher risk of osteoporotic fracture compared with non-RA subjects.(1) A number of factors such as older age, female sex, menopause, lower body mass index (BMI), glucocorticoids use, high RA disease activity, long RA disease duration, and decreased physical activity are associated with an increased risk of osteoporosis.(2, 4–7) Several studies demonstrated a link between proinflammatory cytokines such as tumor necrosis factor (TNF)-α, interleukin-1 and 6, and osteoporosis.(6, 8–10) These cytokines play an important role in bone resorption by stimulating osteoclast differentiation and increasing osteoclast activation. They also potentially lead to bone loss by inhibiting bone formation.(11–13) Some epidemiologic studies, but not all, also note a positive correlation between osteoporosis and C-reactive protein (CRP) which is a marker of active inflammation.(9, 14–16)
The relationship between RA, inflammation and osteoporosis suggests that systemic immunosuppression with disease-modifying antirheumatic drugs (DMARDs) may reduce the risk for osteoporosis and osteoporotic fracture in patients with RA. There is limited data regarding the effect of different DMARD agents, either biologic or non-biologic, and bone metabolism in patients with RA. Furthermore, results from several small studies that examined a potential effect of methotrexate (MTX) or tumor necrosis actor-α inhibitors (TNFi) on the hip, spine, or hand bone mineral density (BMD) were not consistent.(15, 17–28) Little is known about whether use of DMARDs has any impact on the risk of non-vertebral osteoporotic fracture in patients with RA.
We examined the relationship between different DMARD medications and the risk of non-vertebral osteoporotic fracture among RA patients using administrative data from two large health care insurance programs - one Canadian and one US. Based on prior studies suggesting improved BMD with TNFi, we hypothesized that TNFi would decrease the risk of non-vertebral osteoporotic fracture in RA patients compared to non-biologic DMARD (nbDMARD).
MATERIALS & METHODS
Study Design
We conducted a cohort analysis of the risk of osteoporotic fracture among subjects with RA initiating a DMARD. Subjects were enrolled in a Canadian Provincial health care system or a commercial US health plan. The Canadian Provincial health care system includes all persons living in the Province and is considered population-based. The US commercial plan insures mainly working adults and a small Medicare managed care population. The study protocol was approved by the Partners Healthcare Institutional Review Board.
Study Cohort
Potentially eligible subjects were over 18 years of age and diagnosed with RA, based on at least two inpatient or outpatient visits coded with the ICD-9-CM 714.XX. Continuous enrollment in the health plan for 12 months prior to the second diagnosis of RA was required. All persons in the study cohort were required to have had two diagnoses and at least one filled prescription for a DMARD at the start of follow-up Subjects entered the study cohort at the first change in DMARD regimen. Algorithms to define RA in a large health care utilization database that requires both two diagnoses and one or more dispensing of DMARDs have been found to have a positive predictive value of 86% for RA.(29) Our study spanned the period January 1996 through June 2008. Subjects were followed until they experienced an outcome, died, disenrolled from the health plan, or follow-up ended.
Exposure Definitions
We defined three mutually exclusive groups of DMARDs: TNFi, MTX, and other nbDMARD (i.e., hydroxychloroquine, sulfasalazine, leflunomide, cyclosporine, azathioprine, cylclophosphamide, mycophenolate mofetil, 6-thioguanine, d-penicillamine, gold, auranofin, myochrysine, and solganol). The TNFi group included adalimumab, etanercept, or infliximab. The MTX group included oral or injectable MTX. Subjects in the TNFi group were on a TNFi with and without non-biologic DMARDs including MTX. Subjects in the MTX group could not simultaneously use a TNFi; however, they could use other nbDMARDs. The other nbDMARD group, chosen as a reference, could not simultaneously use a TNFi or MTX or any other biologic systemic immunosuppressive drug. Study follow-up began with entry into one of these three exposure groups. Because the timing of the potential effect of DMARDs on fracture is not clear, our primary analysis permitted persons to enter the study cohort more than once and considered them in a given exposure group during the period of an active prescription. These assumptions were tested in a sensitivity analysis, in which we only allowed subjects to enter the cohort once.
Outcome Definitions
The primary outcome was defined as a fracture of the hip, wrist, humerus or pelvis, because these are considered to be typical sites of non-vertebral osteoporotic fracture and can be accurately defined in administrative claims databases.(30) The definitions of fracture were based on a combination of inpatient or outpatient diagnoses and procedure codes contained within the study database (see Appendix 1). Patients were censored at their first fracture in the ‘any osteoporotic fracture’ analysis for a given exposure group.
Covariates
Variables potentially related to a future fracture were assessed using data from the 12 months before the index date. These variables included demographic factors (age and sex), osteoporosis-related factors (osteoporosis diagnosis, osteoporosis medications, prior fractures, presence of BMD tests, Parkinson’s disease, Alzheimer’s disease, prior falls, and other comorbidities), use of other medications likely associated with bone metabolism or fall risk (oral glucocorticoids, anticonvulsants, benzodiazepines, selective serotonin reuptake inhibitors (SSRIs), proton pump inhibitors (PPIs), beta blockers, and opioids), and health care utilization factors (number of physician visits, acute care hospitalizations, and number of different medications). To quantify patients’ comorbidities, we calculated the Deyo-adapted Charlson Comorbidity Index based on ICD-9-CM.(31–32) The Comorbidity Index is a summary score, based on the presence of 19 major medical conditions including myocardial infarction, pulmonary, renal, hepatic disease, diabetes, cancer, human immunodeficiency virus infection, etc. A score of 0 represents absence of these comorbidities and a higher score indicates a greater number of comorbid conditions.
Statistical Analyses
We compared the baseline characteristics across the three exposure groups. Fracture of the hip, wrist, humerus or pelvis (‘osteoporotic fracture’) was identified during follow-up and person-years calculated from the start of follow-up until occurrence of fracture or other censoring events. The incidence rate (IR) and hazard ratio (HR) and 95% confidence interval (CI) for fracture was estimated for each exposure group.
The HR of composite osteoporotic fracture was estimated in a series of Cox proportional hazard models with increasing adjustment: Model 1 was adjusted for age and sex; Model 2 was adjusted for age, sex and prior use of steroid; and Model 3 was additionally adjusted for osteoporosis-related risk factors, cumulative steroid dose, use of other drugs such as oral glucocorticoids, anticonvulsants, benzodiazepines, SSRIs, PPIs, beta blockers, and opioids, Charlson Comorbidity Index, and health care utilization characteristics. These covariates were defined using data from the 12 months before the start of study follow-up. No information was available on BMI, BMD, or frailty. We performed the Kolmogorov supremum test to check the proportional hazards assumption for each of the Cox regression models.(33)
Sensitivity analyses included the variations on exposure definition as noted above. Other sensitivity analyses were performed by including only 1) subjects with a follow up period of 90 days or longer as a lag time period; 2) female subjects only; 3) persons with prior glucocorticoid use; 4) persons without prior glucocorticoid use; and 5) focusing only on those without a prior fracture.
RESULTS
We found 116,321 potentially eligible subjects with at least two visits for RA (see Figure 1). From this group, we excluded persons without a 365-day eligibility period prior to cohort entry (n=34,614) or evidence in the database of use of a systemic immunosuppressive drug (n = 65,295). Our final study cohort consisted of 16,412 subjects with 25,988 new treatment episodes.
Figure 1. Study cohort selection.
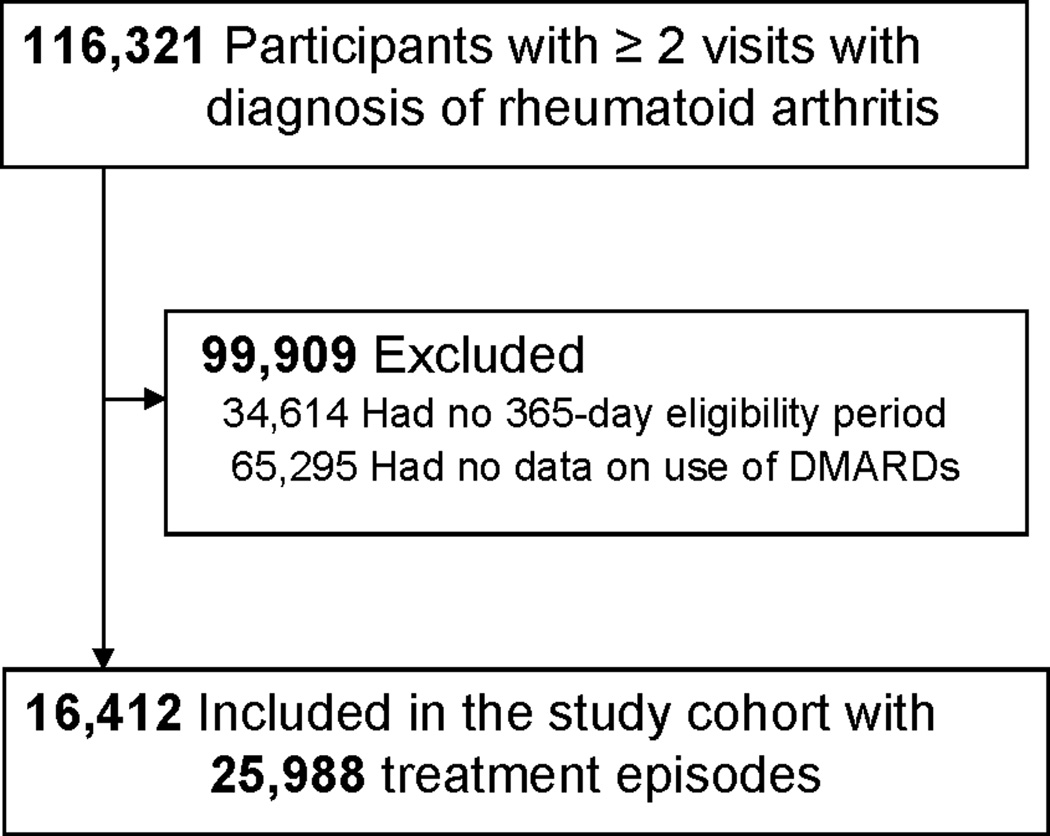
DMARD: disease-modifying antirheumatic drug
Baseline characteristics of the three exposure groups are shown in Table 1. The groups were similar with respect to age, gender, prior fracture and falls, use of osteoporosis medication, number of different medications used, comorbidities, and number of physician visits. Use of oral glucocorticoid in 30 days before the index date as well as the mean cumulative dose of oral glucocorticoids in 12 months before the index date was greater in the TNFi group compared to the MTX or other nbDMARD group Use of other medications such as benzodiazepines, opioids and PPIs was also higher in the TNFi group compared to the MTX or other nbDMARD group.
Table 1.
Baseline characteristics of the study cohort in 12 months before the index date
| TNF inhibitor | Methotrexate | Other non- biologic DMARD |
|
|---|---|---|---|
| No. of treatment episodes | 5,856 | 12,554 | 7,578 |
| Demographic | |||
| Age, mean (SD), years | 52.5 (13.4) | 55.6 (13.3) | 55.2 (13.0) |
| Female | 4,274 (73.0) | 9,464 (75.4) | 5,838 (77.0) |
| Osteoporosis-related | |||
| Osteoporosis diagnosis | 840 (14.3) | 1,429 (11.4) | 1,133 (15.0) |
| Osteoporosis medication | 1,129 (19.3) | 2,372 (18.9) | 1,535 (20.3) |
| Prior fracture | 58 (1.0) | 95 (0.8) | 83 (1.1) |
| Bone mineral density test | 860 (14.7) | 1,655 (13.2) | 1,056 (14.0) |
| Parkinson’s disease | 10 (0.2) | 23 (0.2) | 8(0.1) |
| Alzheimer’s disease | 2 (0.03) | 4 (0.03) | 7 (0.09) |
| Prior fall | 71 (1.2) | 143 (1.1) | 115 (1.5) |
| Comorbidity Index, mean (SD) a | 1.63 (1.4) | 1.68 (1.6) | 1.74 (1.5) |
| Medication use | |||
| Recent use of oral glucocorticoids b | 2,149 (36.7) | 3,499 (27.9) | 2,183 (28.8) |
| Cumulative dose of oral glucocorticoids, mean (SD) c | 659.7 (1605.4) | 415.6 (1077.7) | 526.59 (1465.3) |
| Anticonvulsants | 381(6.5) | 673 (5.4) | 575 (7.6) |
| Benzodiazepines | 945 (16.1) | 1663 (13.3) | 1,184 (15.6) |
| SSRIs | 968 (16.5) | 1746 (13.9) | 1,184(15.6) |
| Proton pump inhibitors | 1,440 (24.6) | 2,455(19.6) | 1,702 (22.5) |
| Beta blockers | 686 (11.7) | 1,483 (11.8) | 968 (12.8) |
| Opioids | 2,515 (43.0) | 3,688 (29.4) | 2,725 (36.0) |
| Health care utilization | |||
| Number of physician visits, mean (SD) | 17.4 (13.3) | 17.3 (13.1) | 17.7 (13.6) |
| Hospitalizations | 939 (16.0) | 1,778 (14.2) | 1,302 (17.2) |
| Number of all prescription drugs, mean (SD) | 11.9 (6.4) | 10.8 (6.2) | 11.9 (6.7) |
TNF: tumor necrosis factor, DMARD: disease-modifying antirheumatic drug Data are expressed as number (%).
SSRI, selective serotonin re-uptake inhibitor
Charlson-Deyo Comorbidity Index (31); a score of 0 represents absence of comorbidity and higher scores indicate a greater burden of comorbidity
Use of any oral glucocorticoids in 30 days prior to the index date
cumulative dose of oral glucocorticoids in 12 months prior to the index date in milligrams
The IR for osteoporotic fracture at any of four sites, hip, humerus, pelvis, and wrist, was 6.38 (95% CI, 3.78–10.77) per 1,000 person-years for persons who started other nbDMARD, 5.38 (95% CI, 4.08–7.02) per 1,000 person-years for MTX and 5.11 (3.50–7.45) per 1,000 person-years for a TNFi (see Table 2).
Table 2.
Incidence rates (IR) of osteoporotic fracture by fracture site and DMARD use
| TNF inhibitor | Methotrexate | Other non-biologic DMARD | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Fractures, N |
Person- years |
IR (95% CI) |
Fractures, N |
Person- years |
IR (95% CI) |
Fractures, N |
Person- years |
IR (95% CI) |
|
| Fracture site | |||||||||
| Any site | 27 | 5285.2 | 5.11 (3.50–7.45) | 52 | 9712.6 | 5.35 (4.08–7.02) | 14 | 2194.4 | 6.38 (3.78–10.77) |
| Hip | 7 | 5302.9 | 1.32 (0.63–2.77) | 7 | 9739.1 | 0.72 (0.34–1.51) | 5 | 2199.2 | 2.27 (0.94–5.45) |
| Humerus | 7 | 5299.5 | 1.32 (0.63–2.77) | 7 | 9739.0 | 0.72 (0.34–1.51) | 2 | 2202.6 | 0.91 (0.23–3.64) |
| Pelvis | 7 | 5301.3 | 1.32 (0.63–2.77) | 23 | 9730.7 | 2.36 (1.57–3.55) | 5 | 2201.5 | 2.27 (0.94–5.45) |
| Wrist | 9 | 5299.8 | 1.70 (0.88–3.27) | 16 | 9733.2 | 1.64 (1.00–2.68) | 4 | 2201.9 | 1.82 (0.68–4.85) |
TNF: tumor necrosis factor, DMARD: disease-modifying antirheumatic drug, CI: confidence interval; IRs are presented per 1,000 person-years.
Table 3 contains the HRs for fracture at each anatomical location in multivariate models. After full multivariable adjustment controlling for osteoporosis and fracture-related factors, the risk of osteoporotic fracture was not different in either TNFi (1.07, 95% CI 0.57–1.98) or MTX (1.18, 95% CI 0.60– 2.34) initiators, compared with nbDMARD. No significantly elevated risks were noted across four different anatomical sites.
Table 3.
Adjusted Cox proportional hazard ratios (95% confidence interval) of osteoporotic fracture in rheumatoid arthritis by fracture site and DMARD use a
| TNF inhibitor | Methotrexate | Other non-biologic DMARD |
|
|---|---|---|---|
| Fracture site | |||
| Any site | 1.18 (0.60–2.34) | 1.07 (0.57–1.98) | 1.00 |
| Hip | 0.65 (0.18–2.32) | 0.44 (0.13–1.54) | 1.00 |
| Humerus | 2.87 (0.56–14.62) | 1.18 (0.23–5.90) | 1.00 |
| Pelvis | 1.11 (0.32–3.82) | 1.25 (0.44–3.57) | 1.00 |
| Wrist | 1.22 (0.35–4.19) | 1.24 (0.39–3.92) | 1.00 |
TNF: tumor necrosis factor, DMARD: disease-modifying antirheumatic drug
Adjusted for age, sex, baseline steroid use, diagnosis of osteoporosis, Alzheimer’s dementia, Parkinson disease, prior fall, prior fracture, use of osteoporosis drugs, anticonvulsants, benzodiazepines, opioids, selective serotonin reuptake inhibitors, and proton pump inhibitors, and Charlson Score.
For the composite outcome, osteoporosis fracture at any of four sites, neither the partially (Models 1 and 2) nor the fully adjusted (Model 3) models suggest a reduced relative risk in patients initiating a TNFi and MTX compared with other nbDMARD (see Appendix 2).
None of the sensitivity analyses (see Figure 2) showed a decreased relative risk of non-vertebral osteoporotic fracture for RA patients initiating a TNFi compared to nbDMARD. We also performed a sensitivity analysis that allowed a subject to enter the cohort only once. 3,438 subjects started a TNFi, 9,461 MTX, and 3,513 other nbDMARD. The HR of osteoporotic fracture was 1.28 (95% CI, 0.56–2.95) for TNFi initiators and 0.85 (95% CI, 0.40–1.83) for MTX compared to other nbDMARD. For every model, the result of the Kolmogorov-type supremum test was not significant (all p-values > 0.80). Therefore, the "proportional hazards assumption" was not violated in our models.
Figure 2. Sensitivity Analyses.
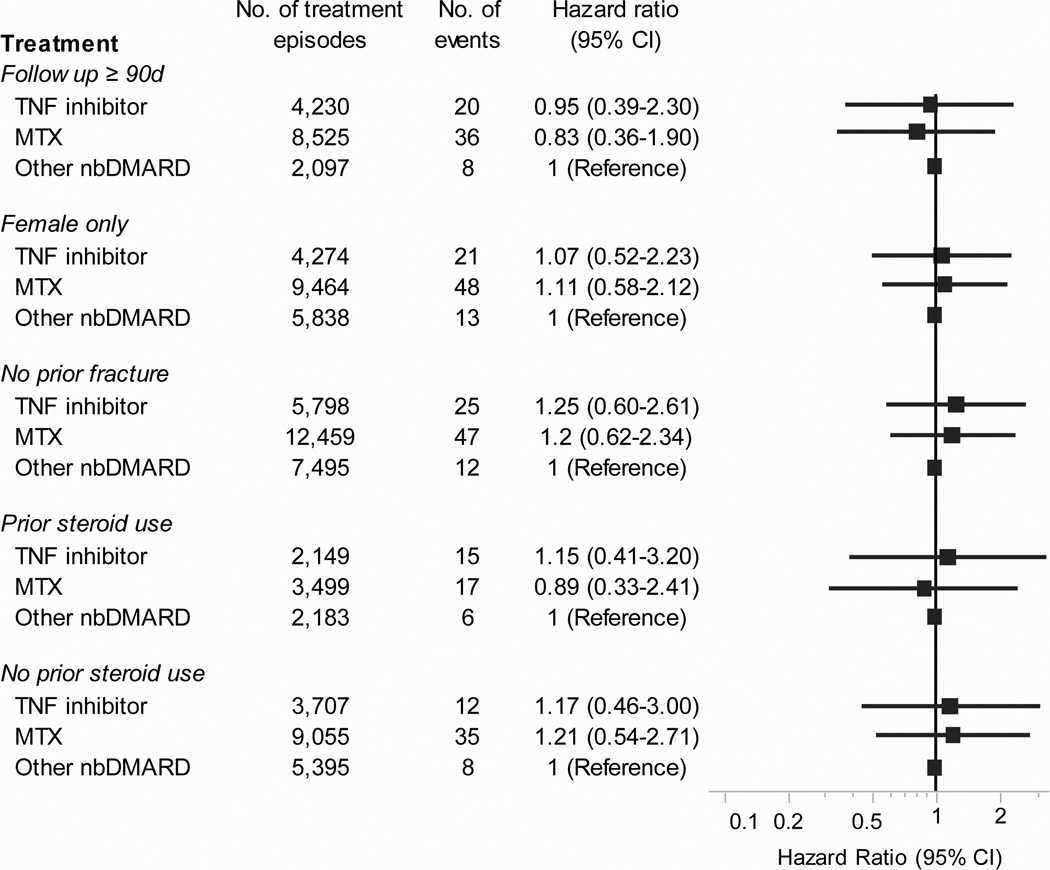
TNF: tumor necrosis factor, MTX: methotrexate, nbDMARD: non-biologic disease-modifying antirheumatic drug, CI: confidence interval
DISCUSSION
RA is associated with focal bone erosions at the joint and systemic bone loss, osteoporosis. Although the bone resorption process in RA is not fully understood, it has been shown that TNF α as well as the ligand for receptor activator of NF-κB (RANKL) have regulatory effects on osteoclastogenesis in RA, leading to development of bone erosion.(34) Chronic inflammation, mediated by these proinflammatory cytokines, is thought to increase the risk of osteoporosis and fracture in RA.(10) We examined the risk of osteoporotic fracture associated with a variety of DMARDs used for RA, because there is a possibility that use of systemic immunosuppressants such as DMARDs may reduce the risk of osteoporosis and there is limited data available for the risk of osteoporotic fracture in patients with RA relative to their treatment. The main finding of this study is, however, that osteoporotic fracture risk was not reduced in RA patients initiating a TNFi or MTX, compared to those starting other nbDMARD. Results from a variety of sensitivity analyses were also similar.
In our study, a fully adjusted HR was 1.07 (95% CI 0.57–1.98) in patients starting MTX compared to other nbDMARD. MTX was previously thought to have detrimental effects on bone, described by the term ‘MTX osteopathy’, mostly reported in children who had had a long-term maintenance therapy of MTX for acute leukemia.(35–36) Conflicting data, however, exists on the effect of low dose MTX in patients with rheumatic disease. Several case series reported stress fracture in tibia or fibula in patients with rheumatic disease on MTX,(37–38) while some found no association between low dose MTX use and change in femoral neck or lumbar spine BMD in RA patients.(17, 39–40) Low dose MTX use was not associated with change in femoral neck or lumbar spine BMD in patients who were not treated with corticosteroids, whereas combined treatment with MTX and 5mg or more prednisone per day was associated with greater bone loss in the lumbar spine than treatment with prednisone without MTX.(17)
Some data exists on a potential beneficial role of TNFi in bone loss,(41) and several published studies have examined BMD changes among patients with RA initiating a TNFi. (see Table 4) Most of the studies were observational and included only a small number of patients on a TNFi, mostly infliximab, and did not have a comparison group. The duration of follow up was generally short, varying from 6 months to 3.5 years. A number of studies reported improvement in the spine or hip BMD among TNFi users,(21, 23, 25) while others reported either stable BMD or less bone loss in TNFi users.(18–19, 22, 24, 26–28, 42–44) Although the exact role of TNFi on BMD remains unknown, one might still believe that BMD improved or did not decrease with use of TNFi.
Table 4.
Summary of published studies for the effect of tumor necrosis factor-α inhibitors on bone mineral density in RA patients
| Study, Yr | Subjects on TNFi | Mean age (yr) |
Subjects on Comparator DMARD |
Follow up period | Findings |
|---|---|---|---|---|---|
| Lange, 2005(23) | 26 IFX | 54 | - | 1 year | BMD increased by 12% at the femoral neck and 3% at the lumbar spine |
| Vis, 2005(27) | 36 IFX | 53 | - | 1 year | BMD remained stable at the spine and hip |
| Vis, 2006(26) | 102 IFX | 53 | - | 1 year | BMD remained stable at the spine and hip |
| Seriolo, 2006(25) | 11 ETA and 10 IFX | 51 | 10 MTX | 6 months | BMD increased by 0.1–0.2% at the spine and hip among TNFi users and decreased by 0.6–0.8% at the spine and hip among MTX users |
| Marotte, 2007(44) | 90 IFX | 51 | 99 MTX | 1 year | BMD decreased by 2.5–3.9% at the spine and femoral neck in the control group, but remained stable in the IFX group |
| Serelis, 2008(24) | 7 ADA and 12 IFX | 54 | - | 1 year | BMD remained stable at the spine |
| Chopin, 2008(18) | 48 IFX | 54 | - | 54 weeks | BMD remained stable at the spine |
| Haugeberg, 2009(20) | 10 IFX | 52 | 10 MTX | 1 year | BMD loss was significantly less in the infliximab group compared with the placebo group at the femoral neck (−0.4% vs. −3.4%) and total hip (−0.2% vs. −2.6%) but not at the hand and spine |
| Wijbrandts, 2009(28) | 52 ADA | 51 | - | 1 year | BMD remained stable at the spine and femur neck |
| Hoff, 2009(22) | 522 ADA | 52 | 246 MTX | 104 weeks | Hand BMD loss was lowest in the ADA plus MTX group and greatest in the MTX group (−3.0% vs. −4.6%) |
| Güler-Yüksel, 2009(19) | 52 IFX | 54 | 166 on other treatment | 2 years | Hand BMD loss was less in the IFX group compared with other treatment only |
| Eekman, 2011(21) | 52 IFX | 60 | - | 3.5 years | BMD was stable at the hip, increased by 2.6% at the spine, and decreased by 3.1% in the hand |
| Hoff, 2011(43) | 214 ADA | 52 | 188 MTX | 2 years | Hand bone loss was less in the ADA plus MTX group, independently of clinically assessed disease activity |
TNFi: tumor necrosis factor-α inhibitor, BMD: bone mineral density, IFX: infliximab, ADA, adalimumab, ETA: etanercept, MTX: methotrexate, DMARD: disease-modifying antirheumatic drug
Why did this current study then not observe similar effects on the risk of fracture? Even if a TNFi increases BMD in RA patients to some degree, it is possible that such improvement in BMD does not fully lead to lowering fracture risk in this patient population at high risk of osteoporosis and fracture. Several limitations in our study might also provide potential explanations. First, this cohort study is likely subject to residual confounding by race, family history of osteoporosis, BMD, BMI, calcium and vitamin D intake, frailty, physical activity, and other unmeasured risk factors. Although we assessed variables potentially related to a future fracture using the data from the 12 months prior to the index date, this time period might not be long enough to capture all the information on potential confounders.
Use of corticosteroids was adjusted as both the cumulative dose of oral corticosteroids in 12 months before the index date and any use of oral corticosteroids in 30 days before the index date. Steroid use during the follow-up period was not adjusted in our analysis. A recent study, however, showed that the use of medications (i.e., steroids or non-steroidal anti-inflammatory drugs) to control symptoms increased in the 6 months immediately before a new DMARD regimen was initiated compared to the previous 6–12-month period and that there was only modest change in the use of corticosteroids in 6–12 months after initiation of DMARDs.(45)
Second, as true in most epidemiologic studies, patients were not randomly exposed to drugs in our study. Therefore, the possibility of confounding by indication cannot be excluded with regard to the effect of different DMARDs on fracture risk in patients with RA. Large longitudinal RA registries either in Europe or the US might be an alternative choice for data source to study comparative safety or effectiveness although it is still subject to unmeasured confounding or confounding by indication.(46) One could completely avoid the issue of confounding bias by conducting a randomized clinical trial (RCT) (47). However, there are a number of important limitations in RCTs, including insufficient sample sizes, inadequate follow-up time, generalizability, ethical issues, and substantial cost, to study a relatively uncommon, long-term safety outcome of drugs such as fracture. It is highly unlikely that there will be a head-to-head randomized clinical trial of DMARDs that can address such safety outcome.
Third, there could be misclassification with the diagnoses of RA and osteoporotic fractures as we mainly relied on diagnosis and procedure codes to identify them although both the ICD codes for RA and fracture and procedure codes for fractures have been used a number of studies.(1, 30, 48)
Lastly, it is possible that our study had inadequate power to detect an increased the risk of osteoporotic fracture related to use of TNFi or MTX compared to other nbDMARD. Even with the use of a large cohort of RA patients from the combined data set (N= 16,412), it is challenging to investigate the risk of a relatively uncommon outcomes (fractures). Our results show that we can exclude an increase in the rate of osteoporotic fracture by more than 100% in TNFi and 135% in MTX initiators compared to nbDMARD initiators, with a confidence level of 95%.(49)
Several strengths of the current study are also worth noting. Our study provides novel information on treatment-specific fracture risk in RA patients using data from a population that is representative of the U.S. commercially-insured population and a Canadian Province. The study databases comprise many thousand patients from various settings, allowing us to better generalize from the findings of a specific study. Despite the aforementioned limitations such as unmeasured confounding or misclassification, our results were simultaneously adjusted for more than 20 risk factors of osteoporotic fracture in the multivariable Cox models and remained consistent across different patient subgroups in various sensitivity analyses. We used pharmacy claims information to identify initiators of different DMARD agents, which is thought to be more accurate than the use of medical records or patient-report.(50) Furthermore, the new user design employed in the present study, in which exposure time begins with the start of a new systemic immunosuppressive, allows for a more valid comparison of treatments than mixing ongoing users with new users in the same analysis.(51)
In conclusion, our study showed that the adjusted risk of fracture was similar across patients with RA starting a TNFi, MTX, or other nbDMARD. Various sensitivity analyses also yielded consistent results. Future studies using a detailed clinical dataset from large prospective RA cohorts or randomized clinical trials of DMARDs with long-term follow up periods could provide further information in fracture risk in RA patients relative to different DMARDs.
Acknowledgements
Kim is supported by the NIH grant K23 AR059677.
Schneeweiss is principal investigator of the Brigham and Women’s Hospital DEcIDE Center on Comparative Effectiveness Research, funded by the Agency for Healthcare Research and Quality, and of the Harvard-Brigham Drug Safety and Risk Management Research Contract, funded by the US Food and Drug Administration.
Solomon is supported by the NIH grants K24 AR055989, P60 AR047782, R21 DE018750, and R01 AR056215.
Appendix 1
Definition of fracture outcomes
| Fracture | Definition |
|---|---|
| Humerus | Humerus fracture diagnosis (ICD-9: 812.xx, 733.11) AND procedure within 30 days of fracture date (ICD-9: 78.52, 79.01, 79.11, 79.21, 79.31, 79.61; CPT-4: 23600, 23605, 23610, 23615, 23620, 23625, 23630, 23665, 23670, 23680, 24500, 24505, 24506, 24510, 24515, 24530, 24531, 24535, 24536, 24538, 24540, 24542, 24545, 24560, 24565, 24570, 24575, 24581, 24583, 24585-8, 24516) |
| Wrist | Radius/ulna fracture diagnosis (ICD-9: 813.xx, 733.12) AND procedure within 30 days of fracture date (ICD-9: 78.53, 79.02, 79.12, 79.22, 79.32, 79.62; CPT-4: 24620, 24625, 24635, 24650, 24655, 24660, 24665-6, 24670, 24680, 24685, 25500, 25505, 25510, 25515, 25530, 25535, 25540, 25545, 25560, 25565, 25570, 25575, 25600, 25605, 25610-1, 25615, 25620, 25650) |
| Hip | Hip fracture diagnosis (ICD-9 code: 820.xx,733.14) during hospitalization AND procedure code during hospitalization (ICD-9: 78.55, 79.05, 79.15, 79.25, 79.35, 79.65; CPT-4: 27230–27248) |
| Pelvis | Pelvis fracture diagnosis (ICD-9: 808.xx) |
ICD-9: International Classification of Diseases −9; CPT-4: Current Procedural Terminology −4
Appendix 2
Adjusted Cox proportional hazard ratios (95% confidence interval) for risk of osteoporotic fracture in rheumatoid arthritis
| TNF inhibitor | Methotrexate | Other non-biologic DMARD |
|
|---|---|---|---|
| Model 1 | 1.27 (0.80–2.00) | 0.77 (0.51–1.17) | 1.00 |
| Model 2 | 1.20 (0.76–1.91) | 0.80 (0.53–1.21) | 1.00 |
| Model 3 | 1.18 (0.60–2.34) | 1.07 (0.57–1.98) | 1.00 |
TNF: tumor necrosis factor, DMARD: disease-modifying antirheumatic drug
Model 1: Adjusted for age and sex. Model 2: Adjusted as Model 1 + baseline steroid use. Model 3: Adjusted as Model 2 + diagnosis of osteoporosis, Alzheimer’s dementia, Parkinson disease, prior fall, prior fracture, use of osteoporosis drugs, anticonvulsants, benzodiazepines, opioids, selective serotonin reuptake inhibitors, and proton pump inhibitors, and Charlson Score.
Footnotes
Competing interests
Kim has received research support from Takeda Pharmaceuticals North America and Pfizer. Schneeweiss is a paid member of scientific advisory boards for HealthCore and has received consulting fees from WHISCON. Schneeweiss received research grants from Pfizer and Novartis.
Solomon has received research support from Abbott Immunology, Amgen and Lilly and an educational grant from Bristol-Myers Squibb. He serves an unpaid member of an Executive Committee and a Data Safety Monitoring Board for two analgesic trials sponsored by Pfizer.
REFERENCES
- 1.Kim S, Schneeweiss S, Liu J, et al. Risk of osteoporotic fracture in a large population-based cohort of patients with rheumatoid arthritis. Arthritis Res Ther. 2010;12(4):R154. doi: 10.1186/ar3107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lane N, Pressman A, Star V, et al. Rheumatoid arthritis and bone mineral density in elderly women. The Study of Osteoporotic Fractures Research Group. J Bone Miner Res. 1995;10(2):257–263. doi: 10.1002/jbmr.5650100212. [DOI] [PubMed] [Google Scholar]
- 3.van Staa T, Geusens P, Bijlsma J, et al. Clinical assessment of the long-term risk of fracture in patients with rheumatoid arthritis. Arthritis Rheum. 2006;54:3104–3112. doi: 10.1002/art.22117. [DOI] [PubMed] [Google Scholar]
- 4.Coulson K, Reed G, Gilliam B, et al. Factors influencing fracture risk, T score, and management of osteoporosis in patients with rheumatoid arthritis in the Consortium of Rheumatology Researchers of North America (CORRONA) registry. J Clin Rheumatol. 2009;15(4):155–160. doi: 10.1097/RHU.0b013e3181a5679d. [DOI] [PubMed] [Google Scholar]
- 5.de Jong Z, Munneke M, Lems W, et al. Slowing of bone loss in patients with rheumatoid arthritis by long-term high-intensity exercise: results of a randomized, controlled trial. Arthritis Rheum. 2004;50(4):1066–1076. doi: 10.1002/art.20117. [DOI] [PubMed] [Google Scholar]
- 6.Oelzner P, Schwabe A, Lehmann G, et al. Significance of risk factors for osteoporosis is dependent on gender and menopause in rheumatoid arthritis. Rheumatol Int. 2008;28(11):1143–1150. doi: 10.1007/s00296-008-0576-x. [DOI] [PubMed] [Google Scholar]
- 7.Sinigaglia L, Nervetti A, Mela Q, et al. A multicenter cross sectional study on bone mineral density in rheumatoid arthritis. Italian Study Group on Bone Mass in Rheumatoid Arthritis. J Rheumatol. 2000;27(11):2582–2589. [PubMed] [Google Scholar]
- 8.Barnabe C, Hanley D. Effect of tumor necrosis factor alpha inhibition on bone density and turnover markers in patients with rheumatoid arthritis and spondyloarthropathy. Semin Arthritis Rheum. 2009;39(2):116–122. doi: 10.1016/j.semarthrit.2008.04.004. [DOI] [PubMed] [Google Scholar]
- 9.Ding C, Parameswaran V, Udayan R, et al. Circulating levels of inflammatory markers predict change in bone mineral density and resorption in older adults: a longitudinal study. J Clin Endocrinol Metab. 2008;93(5):1952–1958. doi: 10.1210/jc.2007-2325. [DOI] [PubMed] [Google Scholar]
- 10.McLean R. Proinflammatory cytokines and osteoporosis. Curr Osteoporos Rep. 2009;7(4):134–139. doi: 10.1007/s11914-009-0023-2. [DOI] [PubMed] [Google Scholar]
- 11.Gilbert L, He X, Farmer P, et al. Inhibition of osteoblast differentiation by tumor necrosis factor-alpha. Endocrinology. 2000;141(11):3956–3964. doi: 10.1210/endo.141.11.7739. [DOI] [PubMed] [Google Scholar]
- 12.Taichman R, Hauschka P. Effects of interleukin-1 beta and tumor necrosis factor-alpha on osteoblastic expression of osteocalcin and mineralized extracellular matrix in vitro. Inflammation. 1992;16(6):587–601. doi: 10.1007/BF00919342. [DOI] [PubMed] [Google Scholar]
- 13.Hock J, Krishnan V, Onyia J, et al. Osteoblast apoptosis and bone turnover. J Bone Miner Res. 2001;16(6):975–984. doi: 10.1359/jbmr.2001.16.6.975. [DOI] [PubMed] [Google Scholar]
- 14.Koh J, Khang Y, Jung C, et al. Higher circulating hsCRP levels are associated with lower bone mineral density in healthy pre- and postmenopausal women: evidence for a link between systemic inflammation and osteoporosis. Osteoporos Int. 2005;16(10):1263–1271. doi: 10.1007/s00198-005-1840-5. [DOI] [PubMed] [Google Scholar]
- 15.Maugeri D, Russo M, Franzé C, et al. Correlations between C-reactive protein, interleukin-6, tumor necrosis factor-alpha and body mass index during senile osteoporosis. Arch Gerontol Geriatr. 1998;27(2):159–163. doi: 10.1016/s0167-4943(98)00110-1. [DOI] [PubMed] [Google Scholar]
- 16.Nabipour I, Larijani B, Vahdat K, et al. Relationships among serum receptor of nuclear factor-kappaB ligand, osteoprotegerin, high-sensitivity C-reactive protein, and bone mineral density in postmenopausal women: osteoimmunity versus osteoinflammatory. Menopause. 2009;16(5):950–955. doi: 10.1097/gme.0b013e3181a181b8. [DOI] [PubMed] [Google Scholar]
- 17.Buckley L, Leib E, Cartularo K, et al. Effects of low dose methotrexate on the bone mineral density of patients with rheumatoid arthritis. J Rheumatol. 1997;24(8):1489–1494. [PubMed] [Google Scholar]
- 18.Chopin F, Garnero P, le Henanff A, et al. Long-term effects of infliximab on bone and cartilage turnover markers in patients with rheumatoid arthritis. Ann Rheum Dis. 2008;67(3):353–357. doi: 10.1136/ard.2007.076604. [DOI] [PubMed] [Google Scholar]
- 19.Güler-Yüksel M, Allaart C, Goekoop-Ruiterman Y, et al. Changes in hand and generalised bone mineral density in patients with recent-onset rheumatoid arthritis. Ann Rheum Dis. 2009;68(3):330–336. doi: 10.1136/ard.2007.086348. [DOI] [PubMed] [Google Scholar]
- 20.Haugeberg G, Conaghan P, Quinn M, et al. Bone loss in patients with active early rheumatoid arthritis: infliximab and methotrexate compared with methotrexate treatment alone. Explorative analysis from a 12-month randomised, double-blind, placebo-controlled study. Ann Rheum Dis. 2009;68(12):1898–1901. doi: 10.1136/ard.2008.106484. [DOI] [PubMed] [Google Scholar]
- 21.Eekman D, Vis M, Bultink I, et al. Stable bone mineral density in lumbar spine and hip in contrast to bone loss in the hands during long-term treatment with infliximab in patients with rheumatoid arthritis. Ann Rheum Dis. 2011;70(2):389–390. doi: 10.1136/ard.2009.127787. [DOI] [PubMed] [Google Scholar]
- 22.Hoff M, Kvien T, Kälvesten J, et al. Adalimumab therapy reduces hand bone loss in early rheumatoid arthritis: explorative analyses from the PREMIER study. Ann Rheum Dis. 2009;68(7):1171–1176. doi: 10.1136/ard.2008.091264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lange U, Teichmann J, Müller-Ladner U, et al. Increase in bone mineral density of patients with rheumatoid arthritis treated with anti-TNF-alpha antibody: a prospective open-label pilot study. Rheumatology (Oxford) 2005;44(12):1546–1548. doi: 10.1093/rheumatology/kei082. [DOI] [PubMed] [Google Scholar]
- 24.Serelis J, Kontogianni M, Katsiougiannis S, et al. Effect of anti-TNF treatment on body composition and serum adiponectin levels of women with rheumatoid arthritis. Clin Rheumatol. 2008;27(6):795–797. doi: 10.1007/s10067-008-0855-7. [DOI] [PubMed] [Google Scholar]
- 25.Seriolo B, Paolino S, Sulli A, et al. Bone metabolism changes during anti-TNF-alpha therapy in patients with active rheumatoid arthritis. Ann N Y Acad Sci. 2006;1069:420–427. doi: 10.1196/annals.1351.040. [DOI] [PubMed] [Google Scholar]
- 26.Vis M, Havaardsholm E, Haugeberg G, et al. Evaluation of bone mineral density, bone metabolism, osteoprotegerin and receptor activator of the NFkappaB ligand serum levels during treatment with infliximab in patients with rheumatoid arthritis. Ann Rheum Dis. 2006;65:1495–1499. doi: 10.1136/ard.2005.044198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Vis M, Voskuyl A, Wolbink G, et al. Bone mineral density in patients with rheumatoid arthritis treated with infliximab. Ann Rheum Dis. 2005;64:336–337. doi: 10.1136/ard.2003.017780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wijbrandts C, Klaasen R, Dijkgraaf M, et al. Bone mineral density in rheumatoid arthritis patients 1 year after adalimumab therapy: arrest of bone loss. Ann Rheum Dis. 2009;68:373–376. doi: 10.1136/ard.2008.091611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kim S, Servi A, Polinski J, et al. Validation of rheumatoid arthritis diagnoses in health care utilization data. Arthritis Res Ther. 2011;13(1):R32. doi: 10.1186/ar3260. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ray W, Griffin M, Fought R, et al. Identification of fractures from computerized Medicare files. J Clin Epidemiol. 1992;45(7):703–714. doi: 10.1016/0895-4356(92)90047-q. [DOI] [PubMed] [Google Scholar]
- 31.Deyo R, Cherkin D, Ciol M. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619. doi: 10.1016/0895-4356(92)90133-8. [DOI] [PubMed] [Google Scholar]
- 32.Schneeweiss S, Seeger J, Maclure M, et al. Performance of comorbidity scores to control for confounding in epidemiologic studies using claims data. Am J Epidemiol. 2001;154(9):854–64. doi: 10.1093/aje/154.9.854. [DOI] [PubMed] [Google Scholar]
- 33.Lin D, Wei L, Ying Z. Checking the Cox model with cumulative sums of martingale-based residuals. Biometrika. 1993;80(3):557–572. [Google Scholar]
- 34.Gravallese E, Manning C, Tsay A, et al. Synovial tissue in rheumatoid arthritis is a source of osteoclast differentiation factor. Arthritis Rheum. 2000;43(2):250–258. doi: 10.1002/1529-0131(200002)43:2<250::AID-ANR3>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- 35.O'Regan S, Melhorn D, Newman A. Methotrexate-induced bone pain in childhood leukemia. Am J Dis Child. 1973;126(4):489–490. doi: 10.1001/archpedi.1973.02110190403008. [DOI] [PubMed] [Google Scholar]
- 36.Ragab A, Frech R, Vietti T. Osteoporotic fractures secondary to methotrexate therapy of acute leukemia in remission. Cancer. 1970;25(3):580–585. doi: 10.1002/1097-0142(197003)25:3<580::aid-cncr2820250313>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 37.Mäenpää H, Soini I, Lehto M, et al. Insufficiency fractures in patients with chronic inflammatory joint diseases. Clin Exp Rheumatol. 2002;20(1):77–79. [PubMed] [Google Scholar]
- 38.Alonso-Bartolomé P, Martínez-Taboada V, Blanco R, et al. Insufficiency fractures of the tibia and fibula Semin Arthritis Rheum. 1999;28(6):413–420. doi: 10.1016/s0049-0172(99)80007-9. [DOI] [PubMed] [Google Scholar]
- 39.di Munno O, Mazzantini M, Sinigaglia L, et al. Effect of low dose methotrexate on bone density in women with rheumatoid arthritis: results from a multicenter cross-sectional study. J Rheumatol. 2004;31(7):1305–1309. [PubMed] [Google Scholar]
- 40.Cranney A, McKendry R, Wells G, et al. The effect of low dose methotrexate on bone density. J Rheumatol. 2001;28(11):2395–2399. [PubMed] [Google Scholar]
- 41.Saidenberg-Kermanac'h N, Corrado A, Lemeiter D, et al. TNF-alpha antibodies and osteoprotegerin decrease systemic bone loss associated with inflammation through distinct mechanisms in collagen-induced arthritis. Bone. 2004;35(5):1200–1207. doi: 10.1016/j.bone.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 42.Hippisley-Cox J, Coupland C. Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ. 2009;339:b4229. doi: 10.1136/bmj.b4229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hoff M, Kvien T, Kälvesten J, et al. Adalimumab reduces hand bone loss in rheumatoid arthritis independent of clinical response: subanalysis of the PREMIER study. BMC Musculoskelet Disord. 2011;12(54) doi: 10.1186/1471-2474-12-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Marotte H, Pallot-Prades B, Grange L, et al. A 1-year case-control study in patients with rheumatoid arthritis indicates prevention of loss of bone mineral density in both responders and nonresponders to infliximab. Arthritis Res Ther. 2007;9(3):R61. doi: 10.1186/ar2219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kawai V, Grijalva C, Arbogast P, et al. Changes in cotherapies after initiation of disease-modifying antirheumatic drug therapy in patients with rheumatoid arthritis. Arthritis Care Res. 2011;63:1415–1424. doi: 10.1002/acr.20550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Curtis J, Jain A, Askling J, et al. A comparison of patient characteristics and outcomes in selected European and U.S. rheumatoid arthritis registries. Semin Arthritis Rheum. 2010;40(1):2–14. doi: 10.1016/j.semarthrit.2010.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Csizmadi I, Collet J-P. In: Bias and confounding in pharmacoepidemiology. Strom B, Kimmel S, editors. Textbook of Pharmacoepidemiology: John Wiley & Sons, Ltd; 2006. pp. 167–171. [Google Scholar]
- 48.Ziadé N, Jougla E, Coste J. Using vital statistics to estimate the population-level impact of osteoporotic fractures on mortality based on death certificates, with an application to France (2000–2004) BMC Public Health. 2009;9:344. doi: 10.1186/1471-2458-9-344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Goodman S, Berlin J. The use of predicted confidence intervals when planning experiments and the misuse of power when interpreting results. Ann Intern Med. 1994;121(3):200–206. doi: 10.7326/0003-4819-121-3-199408010-00008. [DOI] [PubMed] [Google Scholar]
- 50.Schneeweiss S, Avorn J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. J Clin Epidemiol. 2005;58(4):323–337. doi: 10.1016/j.jclinepi.2004.10.012. [DOI] [PubMed] [Google Scholar]
- 51.Ray WA. Evaluating medication effects outside of clinical trials: new-user designs. American Journal of Epidemiology. 2003;158(9):915–920. doi: 10.1093/aje/kwg231. [DOI] [PubMed] [Google Scholar]