

Abstract
Background and Purpose: Cerebral fat embolism (CFE) has been diagnosed previously by both brain magnetic resonance imaging (MRI) and dedicated head computed tomography (HCT) studies. The most commonly reported feature on CT is the presence of the “hypodense artery sign,” although the number of reported cases has been minimal to date. Methods: Report of a single case involving a 88-year-old patient who underwent cardiac surgery. Postoperatively, the patient developed right hemiparesis. Contraindications existed for performing brain MRI and dedicated head CT. Portable head CT (pHCT) was obtained. Hounsfield unit measurement was used. Results: A hypodense artery sign was visualized, and Hounsfield unit measurement indicated fat density. Diagnosis was determined to be CFE. Conclusion: This case report emphasizes that pHCT quality may be sufficient to diagnose CFE and offers a viable alternative when MRI or HCT is contraindicated.
Keywords: cerebral fat embolism, imaging, stroke and cerebrovascular disease
A 88-year-old female underwent cardiac surgery involving a mitral valve replacement. Postoperatively, she was noted to have right-sided hemiparesis. She was ineligible for brain magnetic resonance imaging (MRI) due to temporary pacer wires in place and ineligible for dedicated noncontrast head computed tomography (HCT) due to concern over hemodynamic instability. A noncontrast portable HCT (pHCT) was obtained, which showed a large left middle cerebral artery (MCA) infarct. A hypodense filling defect was noted in the distal left MCA on brain and bone windows (Figure 1). Region of interest measurement of CT density of the hypodense lesion was −50 Hounsfield units, consistent with fat density rather than air density.
Figure 1.
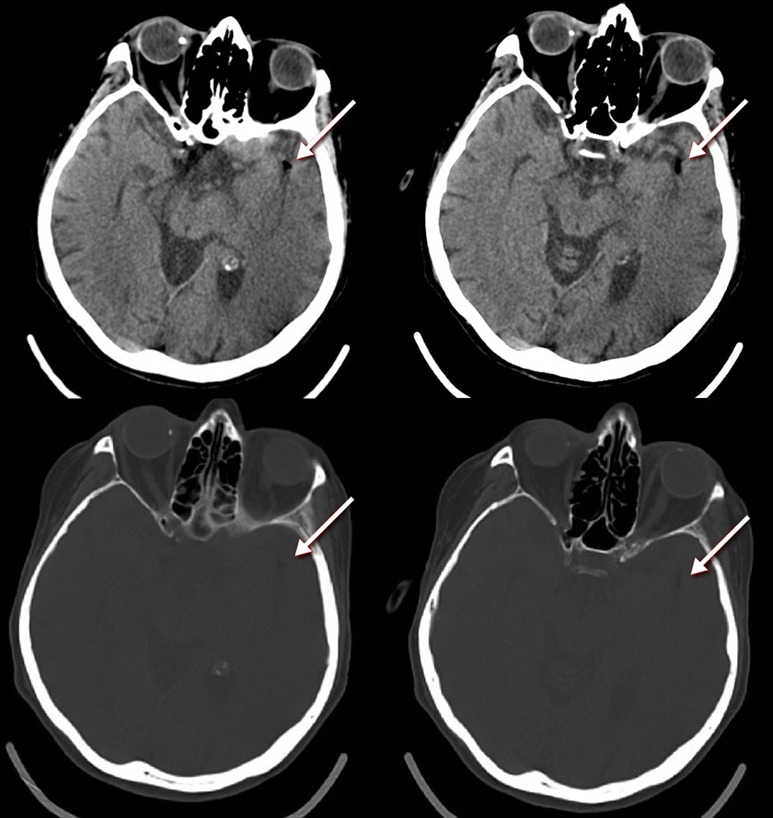
Noncontrast portable head CT revealing cerebral fat embolism in left MCA. CT, computed tomography; MCA, middle cerebral artery.
Cerebral fat embolism (CFE) is an uncommon cause of embolic stroke. In the setting of cardiac surgery, it can arise from extrication of epicardial and pericardial fat, median sternotomy, aortic cannulation during cardiopulmonary bypass, and aortic clamping.1,2 The CFE most commonly manifests as the “hypodense artery sign,” although the number of referenced cases has been minimal.2–4 This case emphasizes that pHCT quality may be sufficient to diagnose CFE, and underscores the importance of this portable modality being readily available in hospitals that actively participate in cardiac surgery as it offers an alternative to patients who may have absolute or relative contraindications to receiving brain MRI or dedicated HCT.
References
- 1. Hedberg M, Boivie P, Edstrom C, Engstrom KG. Cerebrovascular accidents after cardiac surgery: an analysis of ct scans in relation to clinical symptoms. Scand Cardiovasc J. 2005;39(5):299–305 [DOI] [PubMed] [Google Scholar]
- 2. Lee TC, Bartlett ES, Fox AJ, Symons SP. The hypodense artery sign. Am J Neuroradiol. 2005;26(8):2027–2029 [PMC free article] [PubMed] [Google Scholar]
- 3. Abend NS, Levine JM. Hypodense middle cerebral artery with fat embolus. Neurocrit Care. 2007;6(2):147–148 [DOI] [PubMed] [Google Scholar]
- 4. Wang YC, Fu JH, Lai PH. Teaching neuroimages: hypodense artery sign in acute cerebral infarction by contrast-enhanced CT. Neurology. 2009;73(4):e16. [DOI] [PubMed] [Google Scholar]