

Abstract
Fecalomas represent firm organized form of impacted feces. They are commonly seen in sigmoid colon. We report a case of large fecaloma in young adult female with chronic constipation, which was managed conservatively.
Keywords: Fecaloma, Sigmoid colon, Constipation
Case Summary
A 22-year-old female came with complains of chronic constipation for the last 3 months. On examination, abdomen was distended, more on left side. A vague mass was palpated in the left iliac fossa. Per-rectal examination revealed empty rectum with no palpable mass or stricture. Plain abdominal X-rays showed dilatation of distal transverse colon and entire descending colon that was filled with fecal matter. Small bowel loops were displaced to the right side of the abdomen. Ultrasonography of abdomen revealed no contributory finding due to gaseous abdominal distension. A contrast-enhanced computed tomography (CT) of the abdomen was performed. CT showed markedly dilated descending and sigmoid colon filled with intraluminal fecal residue that appeared organized in distal descending and sigmoid colon forming a well-defined intraluminal fecal mass of approximately 12 × 11 × 10 cm in size (Figs. 1 and 2). Transverse colon was also dilated. No obstructing intraluminal mass or stricture was seen in rectosigmoid region. The patient was managed conservatively with enemas and laxatives.
Fig. 1.

Contrast-enhanced axial CT section showing well-formed, large fecal ball in dilated sigmoid colon
Fig. 2.
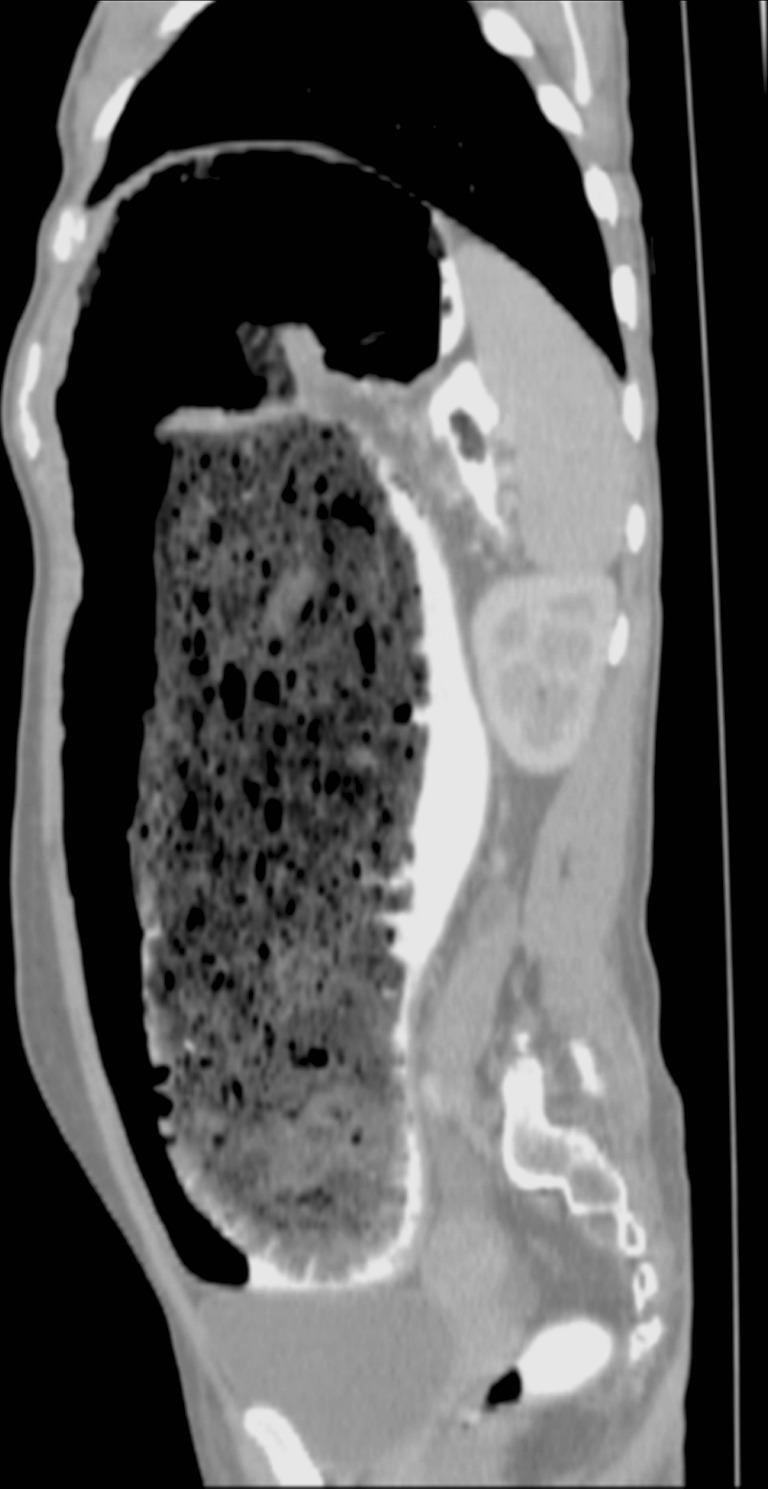
Contrast-enhanced sagittal CT section showing the extent of retained fecal residue in the distal colon
Discussion
Fecaloma is a severe form of fecal impaction. Fecalomas are formed due to prolonged retention of intracolonic fecal residue which gets organized with time to form a well-formed, hard intraluminal fecal mass. Calcification can also be seen. Sigmoid colon and rectum are common sites for fecaloma [1]. Fecalomas are common in Hirschsprung’s disease, Chagas disease, in-patients with spinal injuries, behavioral abnormality, and in elderly patients with chronic constipation [2]. Complications of fecaloma include intestinal obstruction, colonic ulceration, stercoral perforation and hydronephrosis due to mass effect [3, 4]. Treatment options include use of enema, laxatives, and rectal evacuation to relieve fecal impaction and surgical intervention if conservative methods fail.
References
- 1.Rajagopal A, Martin J. Giant fecaloma with idiopathic sigmoid megacolon: report of a case and review of the literature. Dis Colon Rectum. 2002;45:833–835. doi: 10.1007/s10350-004-6306-x. [DOI] [PubMed] [Google Scholar]
- 2.Campbell JB, Robinson AE. Hirschsprung’s disease presenting as calcified fecaloma. Pediatr Radiol. 1973;1:161–163. doi: 10.1007/BF00974061. [DOI] [PubMed] [Google Scholar]
- 3.Knobel B, Rosman P, Gewurtz G. Bilateral hydronephrosis due to fecaloma in an elderly woman. J Clin Gastroenterol. 2000;30:311–313. doi: 10.1097/00004836-200004000-00022. [DOI] [PubMed] [Google Scholar]
- 4.Ouaïssi M, Sielezneff I, Benoist S, Pirró N, Cretel E, Chaix JB, Peschaud F, Consentino B, Malafosse R, Penna C, Sastre B, Nordlinger B. Lethal fecaloma. J Am Geriatr Soc. 2007;55:965–967. doi: 10.1111/j.1532-5415.2007.01191.x. [DOI] [PubMed] [Google Scholar]