

Abstract
To hypothesize that mobile cecum is a rare etiological factor and cecopexy is the choice of treatment in patients with recurrent right lower abdominal pain. Prospective study was conducted in the department of general surgery, SSG Hospital, Baroda, from January 2008 to December 2009. Patients with recurrent right lower abdominal pain were planned for appendectomy. In those patients with intraoperative findings suggestive of macroscopically normal appendix while cecum found to be mobile and no other gross abnormality, appendectomy was performed with cecopexy, fixing cecum to lateral abdominal wall with polypropylene 3-0 suture in interrupted manner. Histopathological examination was confirmed in all the cases. A total of 110 patients complaining of recurrent right lower abdominal pain, with clinical and radiological findings suggestive of appendicitis, were planned for appendectomy. Of 110 patients, 20 were found to have macroscopically normal appearing appendix and of those 20 patients, 8 had cecum unattached to the lateral peritoneal wall. The rest of 90 patients had grossly inflamed appendix in which 10 patients had cecum unattached to the lateral peritoneal wall. Appendectomy and cecopexy were performed in all the patients. On histological examination of the excised appendices, of those 20 with macroscopically normal appearance, 11 had features suggestive of chronic appendicitis and remaining 9 patients were found to have normal histology. While the other 90 with grossly inflamed appendix showed pathological changes of acute inflammation. A total of 64 patients of 110 were followed up till date with no recurrence of abdominal pain. A mobile cecum should be considered a cause of recurrent right lower abdominal pain, and cecopexy is easy to perform and good treatment of choice for a mobile cecum.
Keywords: Mobile cecum, Cecopexy
Introduction
Mobile cecum is defined as a failure of cecum, terminal ileum, and right colon along with the mesentery to fuse to the posterior parietal peritoneal wall (Fig. 1). Abnormal mobility of the cecum and ascending colon has been estimated to occur in 10–20 % of population [1, 2]. Despite the high incidence of anatomic variant, abnormal cecal mobility and ascending colon is an uncommon cause of recurrent right lower abdominal pain [1–3]. Mobile cecum hardly manifests into volvulus; once it does, strangulation ileus follows, developing into gangrene necessitating an emergency surgery if diagnosis of volvulus is delayed [4].
Fig. 1.

Mobile cecum with cecum, appendix, terminal ileum and right colon without lateral peritoneal attachments (artery forceps pointing ileocecal junction)
Patients and Methods
This study had been conducted in the Department of General Surgery, SSG Hospital, Baroda, between January 2008 and December 2009.
A total of 110 patients with history of recurrent right lower abdominal pain were included in the study. Informed written consent was obtained, and the procedure and its outcome were well explained. The operative procedure was performed by the same consultant in all the patients.
All the patients underwent open appendectomy using McBurney’s grid incision, while those with mobile cecum underwent cecopexy. Cecopexy was performed with creating a lateral peritoneal wall flap carefully without injuring any of the retroperitoneal structures and suturing its free edge with taenia coli of cecum using polypropylene (3-0) suture in an interrupted manner (Fig. 2). Extra sutures were taken performing a cecocolopexy where a longer length of the right colon was found unfixed.
Fig. 2.
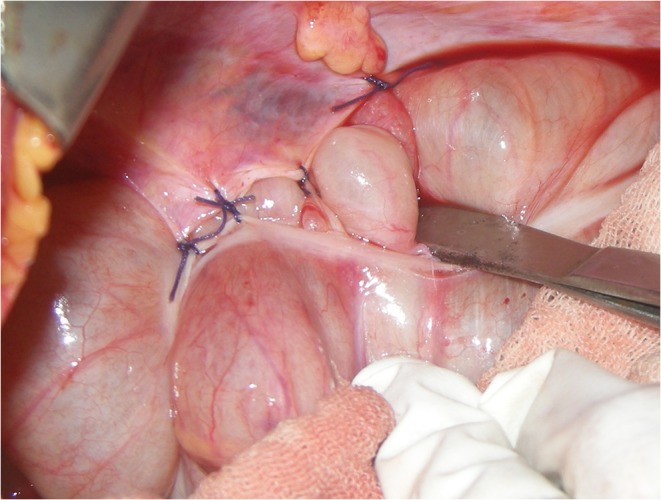
Cecopexy with interrupted sutures between lateral peritoneal flap and cecum
Histopathological diagnoses were confirmed in all the patients.
Postoperative recovery was satisfactory in all the patients with complete healing of the abdominal wound, and subsequently patients were discharged after removal of wound sutures between eighth and tenth postoperative days.
Patients were followed up twice monthly basis for the first 2 months, and thrice monthly basis thereafter. Patients were evaluated for gastrointestinal complaints and other complaints, if any.
Result and Analysis
A total of 110 patients underwent open appendectomy.
60 % patients were females and mean age was 22 years.
Of 110 patients, 90 had grossly inflamed appendix while 20 had no such signs of inflammation (Table 1).
Table 1.
Incidence of inflammation
| Total patients | 110 |
|---|---|
| Grossly inflamed appendix | 90 |
| Grossly normal appendix | 20 |
In 90 patients with grossly inflamed appendix, 10 patients had mobile cecum to the lateral peritoneal wall. While in 20 patients with grossly normal appearing appendix, 8 patients had mobile cecum (Table 2).
Table 2.
Incidence of mobile cecum
| Mobile cecum | |
|---|---|
| Grossly inflamed appendix(90) | 10 |
| Grossly normal appendix(20) | 8 |
On histopathological examination, in grossly normal appearing appendices, 11 had signs of chronic inflammatory changes while rest 9 showed normal histology (Table 3).
Table 3.
Histopathological incidence
| Histopathological changes | |
|---|---|
| Chronic appendicitis | 11 |
| Normal histology | 9 |
Discussion
Embryologically, the cecum and the ascending colon are usually attached retroperitoneally by the posterior peritoneum. Failure of right colonic mesentery to fuse to the lateral peritoneum may lead to an unattached cecum and ascending colon that causes it to be highly mobile [5]. Other reason for mobile cecum is long floppy mesentery fixed to the retroperitoneum by a narrow base of origin [5].
Intermittent bouts of abdominal pain occur as the mobile cecum permits intermittent episodes of isolated cecal obstruction that gets spontaneously resolved as the cecum falls back into its normal position [6].
It is a rare cause of chronic recurrent abdominal pain and is usually found in patients diagnosed with and operated for appendicitis [7].
It may manifest as cecal volvulus presenting with sudden onset abdominal pain, vomiting and abdominal distention which if neglected may result into frank gangrene in which case an emergent surgery with right colectomy is required with a probable defunctioning ileostomy [4, 6].
While it is rare and accounts for only 1 % of mechanical bowel obstructions, it is associated with significant morbidity and mortality, which increases with delay in diagnosis [4, 7]. Santos et al. cited mobile cecum as the first anatomical marker for irritable bowel syndrome [8].
Cecopexy, using lateral peritoneal flap, which was first described by Dixon and Meyers in 1948[9, 10], best achieves fixation of the mobile cecum. It is said to be the surgery of choice for the mobile cecum which is an easy and quick procedure. A large series of 327 patients with mobile cecum it is found that if effectiveness of cecopexy is not satisfactory, ileocecal junction resection or right hemicolectomy can be done [11]. In recent times laparoscopic cecopexy is gaining popularity and is fast becoming the treatment of choice [4, 12]. Other methods for treatment such simply suturing the cecum and ascending colon to the lateral peritoneum and interposition with a sponge have become obsolete due to high rates of failure and recurrence [13].
Hence, whenever a mobile cecum is encountered, it is recommended that a cecopexy should be performed which helps prevent a subsequent cecal volvulus.
Contributor Information
Kirti Garude, Phone: +91-90-51454667, Email: autumn_ksg@yahoo.com.
Sandeep Rao, Email: pgiluvu@gmail.com.
References
- 1.Rogers RL, Harford FJ. Mobile caecum syndrome. Dis Colon Rectum. 1984;27:399–402. doi: 10.1007/BF02553011. [DOI] [PubMed] [Google Scholar]
- 2.Lee YJ, Lee YA, Liu TJ, Chang TH. Mobile caecum syndrome: a report of two cases. Chin Med J (Taipei) 1996;57:380–383. [PubMed] [Google Scholar]
- 3.Pirro N, Corroller LE, Solari C, Merad A, Sielezneff I, Sastre B, Champsaur P, et al. Caecal volvulus: anatomical bases and physiopathology. Morphologie. 2006;90:197–202. doi: 10.1016/S1286-0115(06)74506-4. [DOI] [PubMed] [Google Scholar]
- 4.Tsushimi T, Kurazumi H, Takemoto Y, Oka K, Inokuchi T, Seyama A, et al. Laparoscopic caecopexy for mobile caecum syndrome manifesting as caecal volvulus: Report of a case. Surg Today. 2008;38:359–362. doi: 10.1007/s00595-007-3620-7. [DOI] [PubMed] [Google Scholar]
- 5.Makama JG, Ahmed A. Mobile caecum and ascending colon syndrome in a Nigerian adult. Ann Afr Med. 2009;8(2):133–135. doi: 10.4103/1596-3519.56243. [DOI] [PubMed] [Google Scholar]
- 6.Townsend CM, Beauchamp RD, Evers BM, Mattox KL (eds) (2008) Sabiston Textbook of Surgery, 18th edn., vol. 2. Saunders-Elsevier, Philadelphia, PA, pp 1370–1371
- 7.Rogers RL, Harford FJ. Mobile cecum syndrome. Dis Colon Rectum. 1984;27(6):399–402. doi: 10.1007/BF02553011. [DOI] [PubMed] [Google Scholar]
- 8.Santos JCM, Jr, Cavalca AC, Quiroz CE. Um Marcador Anatômico e a Proposta de Tratamento Rev bras Coloproct. 2006;26(3):300–309. [Google Scholar]
- 9.Dixon CF, Meyer AC. Volvulus of the caecum. Surg Clin North Am. 1948;28:953–963. doi: 10.1016/s0039-6109(16)32484-7. [DOI] [PubMed] [Google Scholar]
- 10.Ris HB, Stirnemann H, Doram JE. The mobile caecum syndrome appendectomy and caecopexy or only appendectomy? Chirurg. 1989;60:277–282. [PubMed] [Google Scholar]
- 11.Wei-Liang Y, Dong-Wei Z, Hao-Gang Z, et al (2009) Diagnosis and treatment of mobile cecum syndrome in 327 patients. J Abdom Surg. http://en.cnki.com.cn/Article_en/CJFDTOTAL-FBWK200904015.htm
- 12.Thanapongsathron W, Kanjanabut B, Vaniyapong T, Thaworncharoen S. Chronic right lower quadrant abdominal pain: laparascopic approach. J Med Assoc Thai. 2005;88:542–547. [PubMed] [Google Scholar]
- 13.El-Katib U. Volvulus of the caecum: caecopexy by polyvinyl alcohol sponge. Br J Surg. 1973;60:475–478. doi: 10.1002/bjs.1800600615. [DOI] [PubMed] [Google Scholar]