

Abstract
Purpose. It is assumed that osteosarcomas of the jaws mainly occur at older ages, whereas the most prominent sites, that is, the long bones, are more affected at ages <20. Jaw-localized tumors are less malignant and have lower metastatic spread rates. Patients and Methods. This study analyses the nationwide data of the Dutch Cancer Registry on osteosarcoma during the period from 1991 to 2010. Age-corrected incidence rates were calculated. Results. In 949, 38 patients had tumors in the maxilla and in 58 in the mandible. Median age for maxilla, mandible, and other localizations was 45.5, 49, and 23 years, respectively. Age-corrected incidence for osteosarcomas increased after a steep decline for the age cohorts from 20 to 60 years to nearly the same level as the younger patients. The incidence for maxillary lesions showed a steady increase from 0.46 to 1.60 per million over all age ranges; the highest incidence for mandibular lesions was found in the age cohort from 60 to 79 years. In respect to histology, no shifts for age were found, except for Paget's disease-related osteosarcoma. In older patients, chemotherapy was omitted more often. Overall survival was similar for all age groups, except for extragnatic tumor patients in the age range of 60–79 years. Conclusions. Osteosarcomas have comparable incidences below the age of 20 as compared with ages >60 years. Poorer outcome in older people is likely due to refraining from chemotherapy.
1. Introduction
Osteosarcoma is the most common malignancy of bone. Based on location of the tumor differences in occurrence, clinical behavior and outcome are assumed. This is especially the case for osteosarcoma of the maxilla and mandible. These locations are presumed to be rare. Percentages of 1 to 9% of the total number of osteosarcomas are mentioned [1–5]. It is further claimed that the mean age of presentation of craniofacial osteosarcomas is at least 10 to 15 years later than osteosarcomas in other parts of the body. However, reports are based on data sources from single institutions or are compiled from registries [4, 6–11]. It is further claimed that tumors in mandible and maxilla are less malignant as based on more often occurrence of low malignant histology and in particular on clinical outcome, that is, a better event, and overall prognosis, and lower incidence of metastatic spread as compared with osteosarcomas arising elsewhere in the body. Metastatic spread at initial presentation up to 16% is reported [3, 7, 11–16]. In this paper the nationwide data on osteosarcomas, as registered by the Netherlands, Cancer Registry of the Comprehensive Cancer Centers of the Netherlands are described.
2. Methods
The retrospective study was carried out on basis of the nationwide coverage of the Netherlands Cancer Registry over the period 1991–2010. Data that could be collected were year of diagnosis, age at diagnosis, localization, histological type of osteosarcoma, occurrence of death, duration of followup, and type of treatment (surgery, radiotherapy, and chemotherapy). Calculations on incidence were done on basis of population data, as obtained from the Statline database of Statistics Netherlands. Statistics Netherlands, a governmental institution, is responsible for collecting and processing population data in order to publish statistics to be used in practice, by policymakers and for scientific research (http://www.cbs.nl/). For statistical analysis, the SPSS version 19.0 was used. Approval of this retrospective study of blinded data was not needed by law.
3. Results
In total, 949 patients were registered, that is, 499 males and 450 females. In 96 patients, the osteosarcoma was localized in the mandible (n = 38, 4%) or in the maxilla, inclusive adjacent bones (n = 58, 6%). Ages ranged from 0 to 95 years, median 25.00 years and mean 34.68 years. For nonfacial bones ages ranged from 0 to 92 years, median 23.00 and mean 33.52 years, for maxilla and adjacent bones ages ranged from 3 to 92 years, median 45.50 and mean 44.29 years, for mandibular lesion ages ranged from 6 to 75 years, median 49.5 years and mean 46.16. Distribution of osteosarcomas according to age is depicted in Figure 1.
Figure 1.
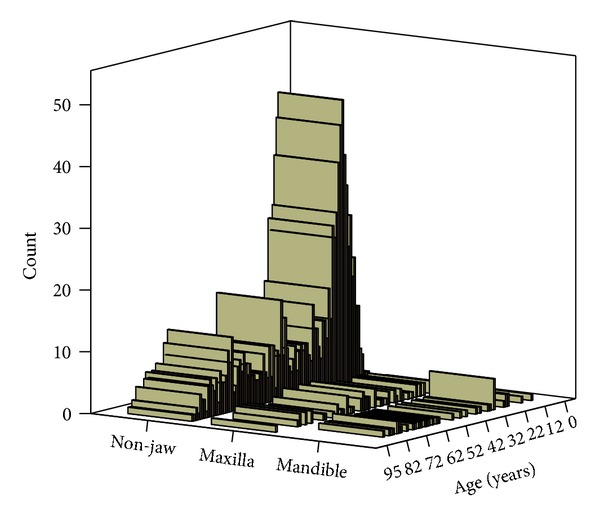
Number of patients per age.
Age-corrected incidence rates were calculated on basis of 20-year age cohorts. These data were related to the distribution of the population in the year 2000. That year was selected since the year 2000 represents the median year of our cohort. In that year, 3.873.008 inhabitants of the Netherlands were 0–19 years of age, 4.761.504 were 20–39 years, 5.076.996 were 40–59 years, 1.652.103 were 60–79 years, and 500.339 were 80–99 years of age. Sites of involvement related to age categories are given in absolute numbers in Table 1. Figure 2 provides data on age-corrected incidence per localization. Calculated age-specific incidences per million are given in Table 2. The highest percentages of jaw tumors were found in the three age categories from 20 to 79 years; 12.0, 17.4, and 14.8, percent, respectively. Whereas in younger (<20 years) and older patients (>79 years) only 3.9 and 2.0 percent of cases were jaw tumors (P < 0.001). In respect to histological type of tumors, the following categories were defined: conventional osteosarcoma (covering osteogenic as well as chondroblastic and fibroblastic osteosarcoma), telangiectatic osteosarcoma, secondary osteosarcoma related to Paget's disease, intraosseous low-grade osteosarcoma, parosteal osteosarcoma, periosteal sarcoma, and high-grade surface osteosarcoma. Distribution over the ages and various age-groups is given in Table 3. Table 4 gives total numbers of non-gnatic, maxilla and mandible tumors according to histology; differences were significant (P = 0.01). Age-corrected incidence for histology figures is given in Table 5. Significances found were as follows: Paget's-related osteosarcoma was less frequent in ages < 60, and para-osteal osteosarcoma less prominent in the age range 0–19 and more frequent in the age range 20–39 (all P < 0.05). Assessing per age category the histological types in relation to localization significance was only found for conventional osteosarcoma, occurring more frequent in extragnatic sites in patients under the age of 20 years. But after correction for age-adjusted incidence, significance was lost. Modes of therapy are depicted in Table 6. After correction for age-specific incidence significantly more treatments with chemotherapy only were given below the age of 60 years, and only radiotherapy was given more frequent in patient above the age of 80 years, and only surgery was less done below the age of 40 years. Table 7 gives data on therapy given per localization; differences were not significant (P = 0.10). Data on the analysis for tumors generally acknowledged to be in need for multimodality treatment; that is, conventional osteosarcomas, teleangiectatic osteosarcomas, and high-grade surface osteosarcomas are given in Table 8. After subanalysis per age group, patients <20 years of age more often received combination therapy (P < 0.001), and patients >80 years of age were treated with surgery only (P = 0.035). Additional separate analysis of conventional osteosarcomas for the separate age-groups revealed for nongnatic, maxilla and mandible following data: P < 0.000, P = 0.288, P = 0.128, respectively. For nonconventional osteosarcomas a P value of <0.000 was computed for nongnatic tumors; for other localizations numbers were too low.
Table 1.
Number of cases in relation to localization and age.
| Number of cases | Nongnatic | Maxilla | Mandible |
|---|---|---|---|
| Age category | |||
| 0–19 year | 367 | 9 | 6 |
| 20–39 year | 190 | 15 | 11 |
| 40–59 year | 133 | 21 | 7 |
| 60–79 year | 127 | 9 | 13 |
| 80–99 year | 36 | 4 | 1 |
Figure 2.
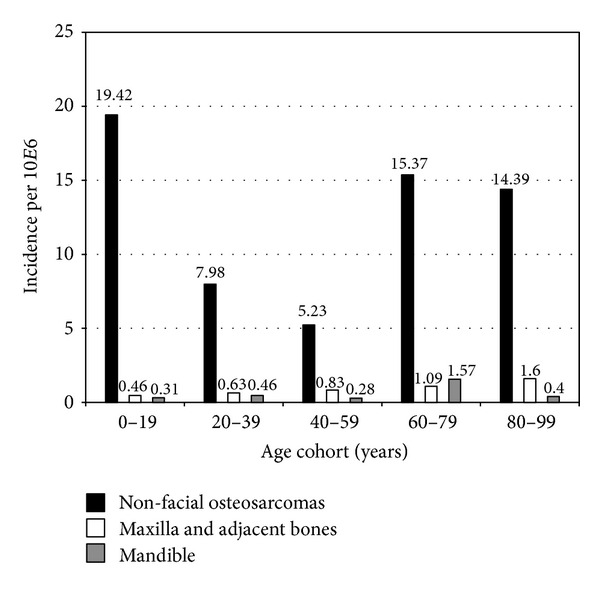
Age-corrected incidence per localization.
Table 2.
Age-corrected incidence rates per million.
| Age category (years) | Total incidence | Extragnatic | Maxilla | Mandible |
|---|---|---|---|---|
| 0–19 | 19.72 | 19.42 | 0.46 | 0.31 |
| 20–39 | 9.07 | 7.98 | 0.63 | 0.46 |
| 40–59 | 6.34 | 5.23 | 0.83 | 0.28 |
| 60–79 | 18.03 | 15.37 | 1.09 | 1.57 |
| 80–99 | 16.39 | 14.39 | 1.60 | 0.40 |
Table 3.
Distribution over the various age groups.
| Conventional OS | Telangiectatic OS | Paget disease-related OS | Intraosteal low malignant OS | Paraosteal OS | Peri-osteal OS | High-grade surface OS | |
|---|---|---|---|---|---|---|---|
| 0–19 years | |||||||
| N = | 348 | 22 | 0 | 1 | 7 | 4 | 0 |
| % | 42.0% | 48.9% | .0% | 100.0% | 12.3% | 80.0% | .0% |
| 20–39 years | |||||||
| N = | 180 | 9 | 0 | 0 | 26 | 1 | 0 |
| % | 21.7% | 20.0% | .0% | .0% | 45.6% | 20.0% | .0% |
| 40–59 years | |||||||
| N = | 137 | 7 | 1 | 0 | 15 | 0 | 1 |
| % | 16.5% | 15.6% | 9.1% | .0% | 26.3% | .0% | 100.0% |
| 60–79 years | |||||||
| N = | 130 | 5 | 7 | 0 | 7 | 0 | 0 |
| % | 15.7% | 11.1% | 63.6% | .0% | 12.3% | .0% | .0% |
| 80–99 years | |||||||
| N = | 34 | 2 | 3 | 0 | 2 | 0 | 0 |
| % | 4.1% | 4.4% | 27.3% | .0% | 3.5% | .0% | .0% |
OS: osteosarcoma.
Table 4.
Distribution of histology per localization.
| Non-jaw | Maxilla | Mandible | |
|---|---|---|---|
| Conventional osteosarcoma | 736 | 56 | 37 |
| Telangiectatic osteosarcoma | 44 | 0 | 1 |
| Paget's disease-related osteosarcoma | 11 | 0 | 0 |
| Intraosseal low malignant osteosarcoma | 0 | 1 | 0 |
| Paraosteal osteosarcoma | 56 | 1 | 0 |
| Periosteal osteosarcoma | 5 | 0 | 0 |
| High-grade surface osteosarcoma | 1 | 0 | 0 |
Table 5.
Age-corrected incidence rates per million for histology.
| Age category (years) | Conventional osteosarcoma | Telangiectatic osteosarcoma | Paget-related osteosarcoma | Intraosseal low malingant osteosarcoma | Paraosteal osteosarcoma | Periosteal osteosarcoma | High-grade surface osteosarcoma |
|---|---|---|---|---|---|---|---|
| 0–19 | 17.97 | 0.93 | 0.00 | 0.05 | 0.36 | 0.21 | 0.00 |
| 20–39 | 7.56 | 0.32 | 0.00 | 0.00 | 1.09 | 0.04 | 0.00 |
| 40–59 | 5.40 | 0.21 | 25.38 | 0.00 | 0.59 | 0.00 | 0.04 |
| 60–79 | 15.74 | 1.91 | 57.82 | 0.00 | 0.85 | 0.00 | 0.00 |
| 80–99 | 13.59 | 5.43 | 7.51 | 0.00 | 0.80 | 0.00 | 0.00 |
Table 6.
Modes of therapy.
| No therapy | Chemotherapy only | Radiotherapy only | Surgery only | Chemotherapy + radiotherapy | Surgery + chemotherapy and/or radiotherapy | Total | |
|---|---|---|---|---|---|---|---|
| 0–19 years | |||||||
| N = | 9 | 33 | 5 | 6 | 6 | 311 | 370 |
| % | 2.4% | 8.9% | 1.4% | 1.6% | 1.6% | 84.1% | 100.0% |
| 20–39 years | |||||||
| N = | 3 | 27 | 1 | 22 | 2 | 134 | 189 |
| % | 1.6% | 14.3% | .5% | 11.6% | 1.1% | 70.9% | 100.0% |
| 40–59 years | |||||||
| N = | 9 | 14 | 4 | 27 | 3 | 88 | 145 |
| % | 6.2% | 9.7% | 2.8% | 18.6% | 2.1% | 60.7% | 100.0% |
| 60–79 years | |||||||
| N = | 24 | 17 | 9 | 57 | 2 | 26 | 135 |
| % | 17.8% | 12.6% | 6.7% | 42.2% | 1.5% | 19.3% | 100.0% |
| 80–99 years | |||||||
| N = | 10 | 0 | 8 | 12 | 0 | 6 | 36 |
| % | 27.8% | .0% | 22.2% | 33.3% | .0% | 16.7% | 100.0% |
|
| |||||||
| Total | |||||||
| N = | 55 | 91 | 27 | 124 | 13 | 565 | 875 |
| % | 6.3% | 10.4% | 3.1% | 14.2% | 1.5% | 64.6% | 100.0% |
Table 7.
Distribution of multimodality treatment per localization.
| Non-jaw | Maxilla | Mandible | |
|---|---|---|---|
| Conventional osteosarcoma | 480 | 30 | 14 |
| Telangiectatic osteosarcoma | 40 | 0 | 1 |
| Paget's-disease related osteosarcoma | 4 | 0 | 0 |
| Intraosseal low malignant osteosarcoma | 0 | 0 | 0 |
| Paraosteal osteosarcoma | 16 | 0 | 0 |
| Periosteal osteosarcoma | 2 | 0 | 0 |
| High-grade surface osteosarcoma | 0 | 0 | 0 |
Table 8.
Therapy for tumors needing multimodality treatment.
| Age | No therapy | Chemotherapy only | Radiotherapy only | Surgery only | Chemotherapy + radiotherapy | Surgery + chemotherapy and/or radiotherapy | Total |
|---|---|---|---|---|---|---|---|
| 0–19 years | |||||||
| N = | 9 | 33 | 5 | 6 | 6 | 311 | 370 |
| % | 2.4% | 8.9% | 1.4% | 1.6% | 1.6% | 84.1% | 100.0% |
| 20–39 years | |||||||
| N = | 3 | 27 | 1 | 22 | 2 | 134 | 189 |
| % | 1.6% | 14.3% | .5% | 11.6% | 1.1% | 70.9% | 100.0% |
| 40–59 years | |||||||
| N = | 9 | 14 | 4 | 27 | 3 | 88 | 145 |
| % | 6.2% | 9.7% | 2.8% | 18.6% | 2.1% | 60.7% | 100.0% |
| 60–79 years | |||||||
| N = | 24 | 17 | 9 | 57 | 2 | 26 | 135 |
| % | 17.8% | 12.6% | 6.7% | 42.2% | 1.5% | 19.3% | 100.0% |
| 80–99 years | |||||||
| N = | 10 | 0 | 8 | 12 | 0 | 6 | 36 |
| % | 27.8% | .0% | 22.2% | 33.3% | .0% | 16.7% | 100.0% |
|
| |||||||
| Total | |||||||
| N = | 55 | 91 | 27 | 124 | 13 | 565 | 875 |
| % | 6.3% | 10.4% | 3.1% | 14.2% | 1.5% | 64.6% | 100.0% |
Higher percentages of older patients did not receive multimodality (surgery, chemotherapy, and/or radiotherapy) treatment (P < 0.05); single modality treatment is more often given to older patients as compared with younger individuals. In patients >79 years, the percentage of patients treated with only radiotherapy are substantially higher (P < 0.05).
From the database details on relapse and other events were incomplete. As a result no figures on event-free survival can be given. However, sound data on occurrence of death were available and overall survival rates (OS) could be computed. In respect to OS, no differences in gnatic versus nongnatic sites were found (Figure 3; log-rank 0.61). Assessment per age category revealed that patients aged between 60 to 79 years had a poorer outcome in case of extra-gnatic locations as compared to gnatic lesions (P = 0.031; Figure 4).
Figure 3.
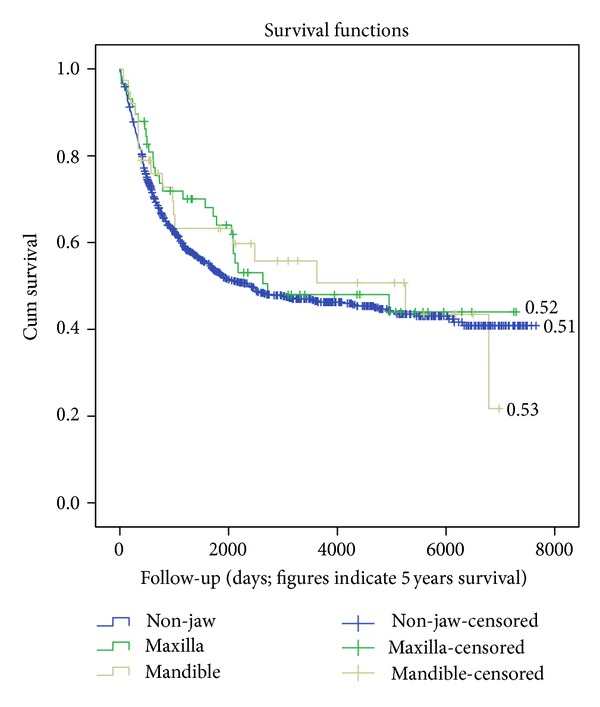
Overall survival according to localization.
Figure 4.
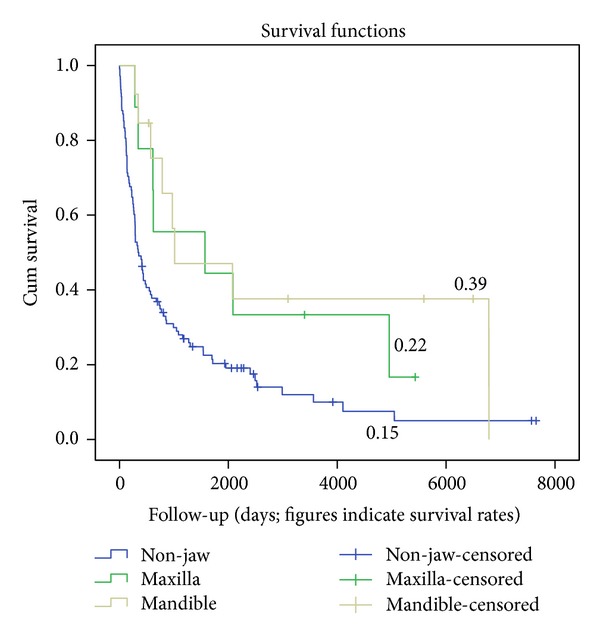
Overall survival in 60 to 79 year old persons.
After sorting out the various pathology subsets also in the mentioned age-group only significance was found for conventional osteosarcomas (P = 0.013). Log-rank correlations revealed high significance for the various modes of treatment (P < 0.001). The highest survival rates were seen for combined modality treatment and surgery only versus the other modes of treatment. However, further analysis comparing combined modality treatment with surgery only was not significant (P = 0.084; see Figure 5).
Figure 5.
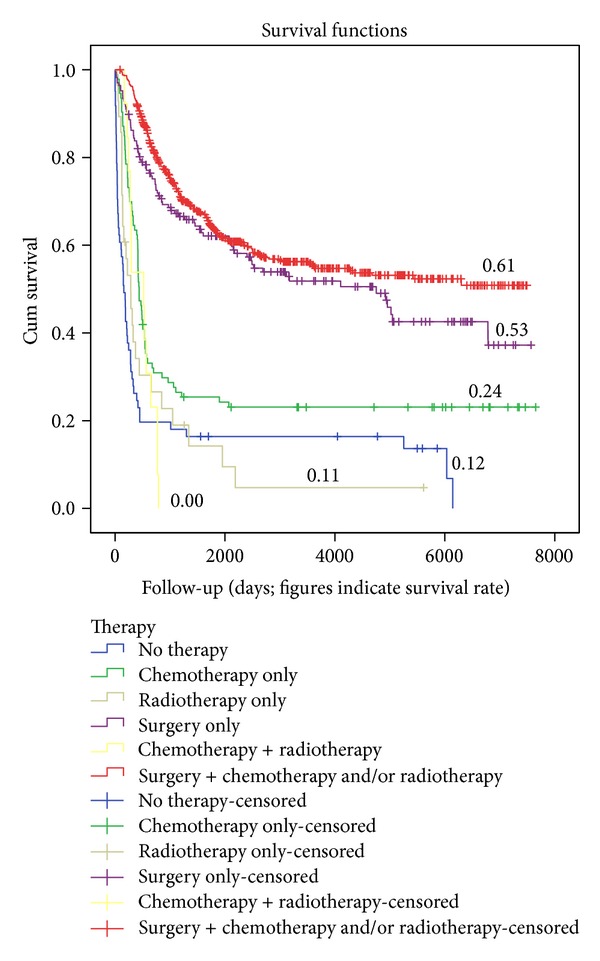
Overall survival in relation to therapy.
Splitting it up into age categories only in the age category from 20 to 39 years, a significance was documented (P = 0.006). Analysis per age category revealed that with increasing age, overall survival showed a significant trend for poorer outcomes at older age (P < 0.001). Splitting the data up in nonjaw, maxilla, and mandible locations, significance for maxillary lesions was still prominent (P = 0.020) whilst the significance for mandible lesion overall survival in relation to age was lost, which might in part be due to the low numbers (see figure for non-gnatic lesions). Coxanalysis revealed that mode of therapy had the strongest influence on survival favoring multimodality treatment.
4. Discussion
Osteosarcomas are mostly noted in the long bones, and it is assumed that they have the highest incidence in the second decade of life. Although the number of craniofacial osteosarcomas is very low, the prevalence of jaw osteosarcoma is in fact 10 times greater than that of osteosarcoma in the total body skeleton, considering that jaws represent only 0.86% of total body volume [17]. International studies on osteosarcomas exclude craniofacial osteosarcomas based on the general assumption that these tumors have a histological lower malignancy grading and have a lower tendency for metastatic spread. Collecting data from the literature a number of problems arose if comparisons with our data were made. In the literature, many reports originate from single institutions or from, sometimes, voluntary registries. A summary of the reports that were found is depicted in Table 9 [1–4, 6–8, 10–12, 14–34]. These reports mentioned in total 1382 cases. The number of patients per report ranges from 7 to 496, with a mean of 45 cases per report. Three other problems hamper assessment of our data. The histopathological diagnosis is taken “as read” and probably there has been no histopathological review of several cases in this study. We were also not able to discern primary versus secondary tumors, except for those patients with Paget's disease of the bone as underlying disease. But this condition was not diagnosed in the mandible or maxilla in our group. Also, in the various reports from the literature, discrimination of primary osteosarcomas versus secondary disease was also not possible.
Table 9.
Manuscripts in the literature specific for gnatic osteosarcomas.
| Report | Origin of the data | Total number of patients | Number of primary tumors | Number of patients with underlying bone disease | Percentage of tumors expressed on total of tumors located in the yaws | |
|---|---|---|---|---|---|---|
| Mandible | Maxilla | |||||
| Oda et al. [8] | SI | 13 | 9 | 2 | 62 | 38 |
| Vege et al. [10] | SI | 34 | 34 | 0 | 64 | 36 |
| van Es et al. [18] | MI | 46 | 37 | 7 | 49 | 51 |
| Delgado et al. [2] | SI | 28 | 27 | 1 | 48 | 52 |
| Padilla and Murrah [19] | SI | 7 | 7 | 0 | 71 | 29 |
| Caron et al. [6] | SI | 43 | 29 | 11 | 53 | 47 |
| Mark et al. [20] | SI | 18 | 14 | 4 | 67 | 33 |
| Gadwal et al. [3] | SR | 22 | 22 | 0 | 95 | 5 |
| Junior et al. [21] | SI | 24 | 21 | 0 | 63 | 37 |
| Huh et al. [22] | SI | 12 | 12 | 0 | 75 | 25 |
| Lewis et al. [23] | SI | 12 | 9 | 1 | 41 | 59 |
| Clark et al. [14] | SI | 66 | 59 | 2 | 49 | 51 |
| Forteza et al. [12] | SI | 9 | 9 | 0 | 44 | 56 |
| Bertoni et al. [4] | SI | 28 | 27 | 0 | 71 | 29 |
| Doval et al. [1] | SI | 8 | NR | 50 | 50 | |
| Tanzawa et al. [24] | MI | 114 | NR | 59 | 41 | |
| Slootweg and Muller [16] | SI | 18 | 17 | 0 | 44 | 56 |
| Daw et al. [34] | SI | 18 | 10 | 40 | 60 | |
| Can Soc OLHNSOSG | MR | 35 | NR | 57 | 43 | |
| August et al. [15] | MR | 30 | 27 | 0 | 57 | 43 |
| Smith et al. [25] | SR | 496 | NR | 47 | 53 | |
| Nissanka et al. [17] | SI | 19 | NR | 58 | 42 | |
| Bennett et al. [26] | SI | 25 | 16 | 1 | 70 | 30 |
| McHugh et al. [27] | SI | 21 | 15 | 0 | 50 | 50 |
| Fernandes et al. [28] | SI | 16 | 13 | 2 | 56 | 44 |
| Jasnau et al. [29] | SR | 49 | 36 | 56 | 44 | |
| Guadagnolo et al. [30] | SI | 62 | NR | 53 | 47 | |
| Huber et al. [31] | MI | 14 | 8 | 2 | 50 | 50 |
| Garrington et al. [7] | SR | 56 | 51 | 2 | 68 | 32 |
| Ha et al. [32] | SR | 27 | 20 | 2 | 46 | 54 |
| Thiele et al. [33] | SI | 12 | NR | 42 | 58 | |
S: single, M: multiple, I: institution, and R: registry.
Based on the distribution of ages in our cohort, it is likely that osteosarcomas of the jaws have a nonequal distribution of age-specific incidence across the age ranges. Generally, a peak incidence in the 4th and 5th decade of life is mentioned [1, 7, 12, 14, 16, 19]. This is in contrast to the Japanese data and the data from Bologna stating that the occurrence is similar across age groups, but unfortunately these data were not corrected for age [4, 24]. Based on our data a substantial increase of age-corrected incidence occurs after the age of 60 in non-gnatic as well as gnatic tumors. The absence of the peak in the first two decades of life is specific for gnatic tumors. In the older age ranges, a possible bias might have occurred due to previous radiotherapy for nonmalignant diseases in the head-neck region [35–37]. Due to the number of patients treated with radiotherapy and the decreasing dosages and smaller fields of irradiation currently used, it is likely that the number of secondary tumors will decrease in the coming decades. The lower percentage in older patients treated with multimodality treatment can be explained by the choice of both physicians and older patients to go for care instead of cure in these often frail patients [38–40]. Localization in the maxillary region exceeded mandible localizations, which is not in line with other publications [41]. A predominance in relation with gender was not noted in our cohort, which is also in contrast with some other reports mentioning either male or female but confirms data of others on the equal distribution among genders [6, 14, 15, 42]. The peculiar peak incidences noted in Japan of mandibular tumors in females only were not seen in our cohort [10, 24].
In respect to pathology grading, the current statement that craniofacial osteosarcomas are relatively benign cannot be confirmed from our data. The majority are conventional osteosarcomas, and the relative benign parosteal osteosarcoma was only found once in the jaws, whereas relative benign periosteal osteosarcoma was not diagnosed. However part of the statement on the mild character of these tumors is based on the assumed incidence of metastatic spread. We do not have data on distant metastatic lesions and later outcome in respect to recurrence. Reports in literature are contradictive. The finding that in only one cohort (60–79 years) the overall survival was significantly poorer for extra-gnatic tumors is not fully reassuring on a more benign behavior either, since they are occurring in an older population in which the baseline all-cause survival is lower.
Since we have limited data on outcome and treatment modalities, we can make only limited statements. From our data some conclusions, can be made: (1) at an older age treatment is more often confined to surgery or radiotherapy, and from the age of 60 years onwards chemotherapy is less often given in malignant diseases. (2) Outcome decreases with increasing age. (3) No significant differences could be attributed to site of the osteosarcoma in the maxilla, mandible or extra-gnatic sites. (4) No significant differences in relation to age were found based on histology. Based on our data, the mode of treatment clearly favors multimodality treatment combining chemotherapy with surgery. For combination of chemotherapy and radiotherapy, no conclusions can be made due to the low frequency of radiotherapy, which is clearly related to the low efficacy of radiotherapy in osteosarcomas. In the literature, two meta-analyses gave opposite results in respect to the chemotherapy issue in jaw tumors. In the meta-analysis of Smeele et al., statistical analysis revealed that surgical margins and chemotherapy were independent significant factors for disease-free and overall survival and radiotherapy had an insignificant effect [43]. Kassir et al. mention a poorer survival in case adjuvant chemotherapy was given. This study might be biased as the authors have no data on surgical margins [44]. Other studies suggest a survival benefit if chemotherapy is added, which confirm our findings [8, 17]. Other prognostic factors such as completeness of resection and chemotherapy-induced tumor necrosis, which is the major prognostic factor in osteosarcomas in general, are not available for craniofacial tumors [45]. Size of the tumor and low-grade histology have been assumed to reflect a better prognosis [1, 14, 20].
We conclude that osteosarcomas have comparable incidences below the age of 20 years as compared with ages >60 years. Poorer outcome in older people might be due to refraining from chemotherapy. Treatment of both nonjaw and jaw osteosarcomas is in the far majority based on multimodality treatment composed of chemotherapy and surgery.
Conflict of Interests
There is no conflict of interest for each of the authors.
References
- 1.Doval DC, Kumar RV, Kannan V, et al. Osteosarcoma of the jaw bones. British Journal of Oral and Maxillofacial Surgery. 1997;35(5):357–362. doi: 10.1016/s0266-4356(97)90410-1. [DOI] [PubMed] [Google Scholar]
- 2.Delgado R, Maafs E, Alfeiran A, et al. Osteosarcoma of the jaw. Head and Neck. 1994;16(3):246–252. doi: 10.1002/hed.2880160307. [DOI] [PubMed] [Google Scholar]
- 3.Gadwal SR, Gannon FH, Fanburg-Smith JC, Becoskie EM, Thompson LD. Primary osteosarcoma of the head and neck in pediatric patients: a clinicopathologic study of 22 cases with a review of the literature. Cancer. 2001;91:598–605. [PubMed] [Google Scholar]
- 4.Bertoni F, Dallera P, Bacchini P, Marchetti C, Campobassi A. The Istituto Rizzoli-Beretta experience with osteosarcoma of the jaw. Cancer. 1991;68(7):1555–1563. doi: 10.1002/1097-0142(19911001)68:7<1555::aid-cncr2820680717>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 5.Raubenheimer EJ, Noffke CE. Low-grade intraosseous osteosarcoma of the jaws. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics. 1998;86(1):82–85. doi: 10.1016/s1079-2104(98)90154-8. [DOI] [PubMed] [Google Scholar]
- 6.Caron AS, Hajdu SI, Strong EW. Osteogenic sarcoma of the facial and cranial bones. A review of forty-three cases. The American Journal of Surgery. 1971;122(6):719–725. doi: 10.1016/0002-9610(71)90434-x. [DOI] [PubMed] [Google Scholar]
- 7.Garrington GE, Scofield HH, Cornyn J, Hooker SP. Osteosarcoma of the jaws. Analysis of 56 cases. Cancer. 1967;20(3):377–391. doi: 10.1002/1097-0142(1967)20:3<377::aid-cncr2820200306>3.0.co;2-t. [DOI] [PubMed] [Google Scholar]
- 8.Oda D, Bavisotto LM, Schmidt RA, et al. Head and neck osteosarcoma at the University of Washington. Head and Neck. 1997;19(6):513–523. doi: 10.1002/(sici)1097-0347(199709)19:6<513::aid-hed9>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- 9.Stein JJ. Osteogenic sarcoma (osteosarcoma): results of therapy. American Journal of Roentgenology. 1975;123(3):607–613. doi: 10.2214/ajr.123.3.607. [DOI] [PubMed] [Google Scholar]
- 10.Vege DS, Borges AM, Aggrawal K, Balasubramaniam G, Parikh DM, Bhaser B. Osteosarcoma of the craniofacial bones. A clinico-pathological study. Journal of Cranio-Maxillo-Facial Surgery. 1991;19(2):90–93. doi: 10.1016/s1010-5182(05)80614-6. [DOI] [PubMed] [Google Scholar]
- 11.Osteogenic sarcoma of the mandible and maxilla: a Canadian review (1980–2000) Journal of Otolaryngology. 2004;33(3):139–144. doi: 10.2310/7070.2004.03013. [DOI] [PubMed] [Google Scholar]
- 12.Forteza G, Colmenero B, López-Barea F. Osteogenic sarcoma of the maxilla and mandible. Oral Surgery, Oral Medicine, Oral Pathology. 1986;62(2):179–184. doi: 10.1016/0030-4220(86)90042-3. [DOI] [PubMed] [Google Scholar]
- 13.Unni KK, Dahlin DC. Osteosarcoma: pathology and classification. Seminars in Roentgenology. 1989;24(3):143–152. doi: 10.1016/0037-198x(89)90010-2. [DOI] [PubMed] [Google Scholar]
- 14.Clark JL, Unni KK, Dahlin DC, Devine KD. Osteosarcoma of the jaw. Cancer. 1983;51(12):2311–2316. doi: 10.1002/1097-0142(19830615)51:12<2311::aid-cncr2820511224>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 15.August M, Magennis P, Dewitt D. Osteogenic sarcoma of the jaws: factors influencing prognosis. International Journal of Oral and Maxillofacial Surgery. 1997;26(3):198–204. doi: 10.1016/s0901-5027(97)80819-3. [DOI] [PubMed] [Google Scholar]
- 16.Slootweg PJ, Muller H. Osteosarcoma of the jaw bones. Analysis of 18 cases. Journal of Maxillofacial Surgery. 1985;13(4):158–166. doi: 10.1016/s0301-0503(85)80040-0. [DOI] [PubMed] [Google Scholar]
- 17.Nissanka EH, Amaratunge EAPD, Tilakaratne WM. Clinicopathological analysis of osteosarcoma of jaw bones. Oral Diseases. 2007;13(1):82–87. doi: 10.1111/j.1601-0825.2006.01251.x. [DOI] [PubMed] [Google Scholar]
- 18.van Es RJJ, Keus RB, van der Waal I, Koole R, Vermey A. Osteosarcoma of the jaw bones: long-term follow up of 48 cases. International Journal of Oral and Maxillofacial Surgery. 1997;26(3):191–197. doi: 10.1016/s0901-5027(97)80818-1. [DOI] [PubMed] [Google Scholar]
- 19.Padilla RJ, Murrah VA. The spectrum of gnathic osteosarcoma: caveats for the clinician and the pathologist. Head and Neck Pathology. 2011;5(1):92–99. doi: 10.1007/s12105-010-0218-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mark RJ, Sercarz JA, Tran L, Dodd LG, Selch M, Calcaterra TC. Osteogenic sarcoma of the head and neck: the UCLA experience. Archives of Otolaryngology. 1991;117(7):761–766. doi: 10.1001/archotol.1991.01870190073015. [DOI] [PubMed] [Google Scholar]
- 21.Junior AT, de Abreu AF, Pinto CA, et al. Clinicopathological and immunohistochemical analysis of twenty-five head and neck osteosarcomas. Oral Oncology. 2003;39(5):521–530. doi: 10.1016/s1368-8375(03)00017-4. [DOI] [PubMed] [Google Scholar]
- 22.Huh WW, Holsinger FC, Levy A, Palla FSL, Anderson PM. Osteosarcoma of the jaw in children and young adults. Head and Neck. 2011;34(7):981–984. doi: 10.1002/hed.21850. [DOI] [PubMed] [Google Scholar]
- 23.Lewis M, Perl A, Som PM, Urken ML, Brandwein MS. Osteogenic sarcoma of the jaw: a clinicopathologic review of 12 patients. Archives of Otolaryngology. 1997;123(2):169–174. doi: 10.1001/archotol.1997.01900020051007. [DOI] [PubMed] [Google Scholar]
- 24.Tanzawa H, Uchiyama S, Sato K. Statistical observation of osteosarcoma of the maxillofacial region in Japan. Analysis of 114 Japanese cases reported between 1930 and 1989. Oral Surgery Oral Medicine and Oral Pathology. 1991;72(4):444–448. doi: 10.1016/0030-4220(91)90558-t. [DOI] [PubMed] [Google Scholar]
- 25.Smith RB, Apostolakis LW, Karnell LH, et al. National cancer data base report on osteosarcoma of the head and neck. Cancer. 2003;98(8):1670–1680. doi: 10.1002/cncr.11716. [DOI] [PubMed] [Google Scholar]
- 26.Bennett JH, Thomas G, Evans AW, Speight PM. Osteosarcoma of the jaws: a 30-year retrospective review. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics. 2000;90(3):323–332. doi: 10.1067/moe.2000.108274. [DOI] [PubMed] [Google Scholar]
- 27.McHugh JB, Thomas DG, Herman JM, et al. Primary versus radiation-associated craniofacial osteosarcoma: biologic and clinicopathologic comparisons. Cancer. 2006;107(3):554–562. doi: 10.1002/cncr.22019. [DOI] [PubMed] [Google Scholar]
- 28.Fernandes R, Nikitakis NG, Pazoki A, Ord RA. Osteogenic sarcoma of the jaw: a 10-year experience. Journal of Oral and Maxillofacial Surgery. 2007;65(7):1286–1291. doi: 10.1016/j.joms.2006.10.030. [DOI] [PubMed] [Google Scholar]
- 29.Jasnau S, Meyer U, Potratz J, et al. Craniofacial osteosarcoma. Experience of the cooperative German-Austrian-Swiss osteosarcoma study group. Oral Oncology. 2008;44(3):286–294. doi: 10.1016/j.oraloncology.2007.03.001. [DOI] [PubMed] [Google Scholar]
- 30.Guadagnolo BA, Zagars GK, Raymond AK, Benjamin RS, Sturgis EM. Osteosarcoma of the jaw/craniofacial region: outcomes after multimodality treatment. Cancer. 2009;115(14):3262–3270. doi: 10.1002/cncr.24297. [DOI] [PubMed] [Google Scholar]
- 31.Huber GF, Dziegielewski P, Matthews TW, Dort JC. Head and neck osteosarcoma in adults: the province of alberta experience over 26 years. Journal of Otolaryngology. 2008;37(5):738–743. [PubMed] [Google Scholar]
- 32.Ha PK, Eisele DW, Frassica FJ, Zahurak ML, McCarthy EF. Osteosarcoma of the head and neck: a review of the Johns Hopkins experience. Laryngoscope. 1999;109(6):964–969. doi: 10.1097/00005537-199906000-00023. [DOI] [PubMed] [Google Scholar]
- 33.Thiele OC, Freier K, Bacon C, Egerer G, Hofele CM. Interdisciplinary combined treatment of craniofacial osteosarcoma with neoadjuvant and adjuvant chemotherapy and excision of the tumour: a retrospective study. British Journal of Oral and Maxillofacial Surgery. 2008;46(7):533–536. doi: 10.1016/j.bjoms.2008.03.010. [DOI] [PubMed] [Google Scholar]
- 34.Daw NC, Mahmoud HH, Meyer WH, et al. Bone sarcomas of the head and neck in children: the St Jude Children's Research Hospital experience. Cancer. 2000;88:2172–2180. doi: 10.1002/(sici)1097-0142(20000501)88:9<2172::aid-cncr25>3.0.co;2-7. [DOI] [PubMed] [Google Scholar]
- 35.Little JB. Radiation carcinogenesis. Carcinogenesis. 2000;21(3):397–404. doi: 10.1093/carcin/21.3.397. [DOI] [PubMed] [Google Scholar]
- 36.Doll R. Hazards of ionising radiation: 100 years of observations on man. British Journal of Cancer. 1995;72(6):1339–1349. doi: 10.1038/bjc.1995.513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.van der Putten L, de Bree R, Kuik DJ, Rietveld DHF, Langendijk JA, Leemans CR. Hypopharyngeal carcinoma after radiation for tuberculosis: radiation-induced carcinoma. Oral Oncology. 2010;46(9):672–677. doi: 10.1016/j.oraloncology.2010.06.013. [DOI] [PubMed] [Google Scholar]
- 38.Terret C, Droz JP. Editorial. The perception and dissemination of geriatric oncology. Critical Reviews in Oncology/Hematology. 2010;75:43–46. doi: 10.1016/j.critrevonc.2010.04.010. [DOI] [PubMed] [Google Scholar]
- 39.Sifer-Rivière L, Girre V, Gisselbrecht M, Saint-Jean O. Physicians’ perceptions of cancer care for elderly patients: a qualitative sociological study based on a pilot geriatric oncology program. Critical Reviews in Oncology/Hematology. 2010;75(1):58–69. doi: 10.1016/j.critrevonc.2010.04.001. [DOI] [PubMed] [Google Scholar]
- 40.Silveira AP, Gonçalves J, Sequeira T, et al. Geriatric oncology: comparing health related quality of life in head and neck cancer patients. Head and Neck Oncology. 2011;3(1, article 3) doi: 10.1186/1758-3284-3-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Koka V, Vericel R, Lartigau E, Lusinchi A, Schwaab G. Sarcomas of nasal cavity and paranasal sinuses: chondrosarcoma, osteosarcoma and fibrosarcoma. Journal of Laryngology and Otology. 1994;108(11):947–953. doi: 10.1017/s0022215100128609. [DOI] [PubMed] [Google Scholar]
- 42.Granados-Garcia M, Luna-Ortiz K, Castillo-Oliva HA, et al. Free osseous and soft tissue surgical margins as prognostic factors in mandibular osteosarcoma. Oral Oncology. 2006;42(2):172–176. doi: 10.1016/j.oraloncology.2005.06.027. [DOI] [PubMed] [Google Scholar]
- 43.Smeele LE, Kostense PJ, van der Waal I, Snow GB. Effect of chemotherapy on survival of craniofaciai osteosarcoma: a systematic review of 201 patients. Journal of Clinical Oncology. 1997;15(1):363–367. doi: 10.1200/JCO.1997.15.1.363. [DOI] [PubMed] [Google Scholar]
- 44.Kassir RR, Rassekh CH, Kinsella JB, Segas J, Carrau RL, Hokanson JA. Osteosarcoma of the head and neck: meta-analysis of nonrandomized studies. Laryngoscope. 1997;107(1):56–61. doi: 10.1097/00005537-199701000-00013. [DOI] [PubMed] [Google Scholar]
- 45.Davis AM, Bell RS, Goodwin PJ. Prognostic factors in osteosarcoma: a critical review. Journal of Clinical Oncology. 1994;12(2):423–431. doi: 10.1200/JCO.1994.12.2.423. [DOI] [PubMed] [Google Scholar]